 Systematic Review
Systematic Review

Affiliation:
School of Law, Business and Psychology, University of Chichester, PO19 6PE Chichester, UK
Email: e.obine@chi.ac.uk
ORCID: https://orcid.org/0000-0002-3697-9025
Affiliation:
School of Law, Business and Psychology, University of Chichester, PO19 6PE Chichester, UK
ORCID: https://orcid.org/0000-0002-9187-0639
Affiliation:
School of Law, Business and Psychology, University of Chichester, PO19 6PE Chichester, UK
ORCID: https://orcid.org/0000-0001-5206-4063
Affiliation:
School of Law, Business and Psychology, University of Chichester, PO19 6PE Chichester, UK
ORCID: https://orcid.org/0000-0001-8539-9935
Explor Neuroprot Ther. 2026;6:1004144 DOI: https://doi.org/10.37349/ent.2026.1004144
Received: October 12, 2025 Accepted: March 06, 2026 Published: April 09, 2026
Academic Editor: Marco Cavallo, eCampus University, Italy
The article belongs to the special issue Innovations in Neurotechnology: Integrating AI, Neuroimaging, and VR for the Assessment and Treatment of Neurological Conditions
Background: Fully immersive virtual reality (IVR) is an emerging technology approach for cognitive training in individuals with mild cognitive impairment (MCI) and dementia. While interest in fully IVR continues to grow, it remains unclear the extent of effectiveness and the key components that contribute to successful implementation. This study aimed to explore the effectiveness of fully IVR cognitive training for individuals with MCI or dementia from previous research literature.
Methods: A scoping review was conducted using a systematic search strategy based on the population, concept, and context framework.
Results: Out of the 816 records identified, 123 full texts were screened, and eight studies were included in the review. The included studies all involved participants completing a cognitive training intervention using fully IVR headsets, with cognitive outcomes measured before and after the intervention. The most consistent improvements across the included studies were executive function, memory, and visuospatial abilities. Only two studies explicitly referenced a theoretical model.
Discussion: Fully IVR cognitive training demonstrates promise for improving specific cognitive domains in individuals living with MCI or dementia. However, inconsistencies in outcomes and limited theoretical grounding highlight the need for further exploration. Broader considerations are discussed in the discussion section.
Globally, more than 55 million people are affected by dementia and incur costs of approximately US$ 1.3 trillion worldwide, in 2019 [1]. In the UK, there are currently an estimated 982,000 individuals living with dementia, a figure projected to exceed 1.4 million by 2040 [2]. The financial burden of dementia in the UK was forecasted to be £42 billion in 2024, projected to rise to £90 billion by 2040 [2]. As life expectancy increases, a key challenge is not only supporting longevity but also maintaining quality of life and cognitive functioning in later life. While dementia is not an inevitable consequence of aging, it significantly affects individual well-being and places pressure on health and social care systems, underscoring the need for effective and accessible interventions to support those individuals living with this condition [3, 4]. Pharmaceutical interventions remain limited in their effectiveness and do not offer a cure, while nonpharmaceutical approaches have demonstrated promising outcomes in slowing cognitive decline and enhancing quality of life [5]. Cognitive training can be classified as a nonpharmaceutical intervention, which involves the engagement in structured practice activities designed to target specific cognitive domains. Despite the rising interest in nonpharmaceutical approaches, there remains limited evidence and consensus on the effectiveness and optimal intervention design for specifically fully immersive virtual reality (IVR) cognitive training for individuals living with mild cognitive impairment (MCI) or dementia.
MCI is defined as the transitional phase from healthy ageing and dementia, offering a unique window for early intervention [6]. Implementing Interventions at this stage for amnesic MCI or non-amnesic MCI may delay the progression to dementia [7]. A promising nonpharmaceutical intervention is computerized cognitive training (CCT), which refers to employing computer-generated tasks/activities to stimulate various cognitive domains [8], and fully IVR technology provides an immersive and engaging platform that is suggested to enhance cognitive training outcomes [9, 10]. Fully IVR systems aim to create a strong sense of presence, allowing users to experience and interact with realistic 3D environments via head-mounted displays and motion tracking [11–13]. For the present review, fully IVR is defined based on the following criteria: 1) 3D visual display through head-mounted displays and 2) interactive engagement with the virtual environment. Given the characteristics of fully IVR, it has the potential to boost motivation [14, 15] and reduce cognitive load by creating engaging, virtual environments that eliminate the need to mentally transform 2D elements to 3D representation [16, 17]. Recent reviews and meta-analyses support the potential of fully IVR cognitive training in improving cognitive functioning in individuals with MCI or dementia [18–21]. Moulaei et al. [19] further demonstrated significant improvements in cognitive function, highlighting the feasibility and benefits of fully IVR cognitive training [22]. However, there is little to no agreement on the most effective cognitive training design features, training intensity, or content. The present scoping review focuses solely on fully IVR technology in the form of head mount displays, not as other studies that have combined various levels of immersive technologies.
The broader field of cognitive training has faced criticism, specifically on the overall effectiveness of cognitive training on global cognition [23–25]. For example, Sala and Gobet [26] contend that cognitive training has minimal impact on general cognitive ability, emphasizing the need for more robust evidence. Nevertheless, studies have demonstrated positive change in cognitive outcomes after completing cognitive training [27, 28]. Studies have also demonstrated positive change after VR-based cognitive training on cognitive ability [18, 29, 30]. Chiu et al. [31] found significant positive outcomes of fully IVR on cognitive functioning in older adults with cognitive impairments. Moreover, there is no clear theoretical explanation for the effectiveness or behavioural change when fully IVR cognitive training is implemented [12]. One relevant theory is the cognitive reserve hypothesis [32, 33], which suggests that engaging in stimulating and challenging tasks can enhance the brain’s resilience to cognitive impairments. Few studies have explicitly linked fully IVR cognitive training to theoretical models, and identifying relevant theories and models within fully IVR cognitive training could highlight components to elicit positive cognitive changes.
To address these gaps, the present study aims to review the current evidence on the effectiveness of fully IVR cognitive training for individuals living with MCI or dementia. The findings aim to inform future research, support the development of fully IVR cognitive interventions, and establish a foundation for best practices.
The review is reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) extension for Scoping Reviews (PRISMA-ScR; Tricco et al. [34]). Prior to the initial searches and screening, the review protocol was pre-registered with the Open Science Framework (https://doi.org/10.17605/OSF.IO/8ERVH).
Scoping review: To what extent… is fully IVR cognitive training effective for individuals living with MCI or dementia, in relation to global cognition and specific cognitive domain outcomes.
The eligibility for our study was guided by the population, concept, and context (PCC) framework. The population included individuals living with predementia or dementia, the concept focused on fully IVR cognitive training, and the context was cognitive functioning. Eligible studies had to meet the following criteria: 1) empirical research; 2) published in English in peer-reviewed journals; and 3) included participants diagnosed with predementia or dementia (refer to Table 1). The population of interest consisted of individuals with cognitive decline, specifically those diagnosed with MCI or dementia, with clear diagnostic criteria such as Petersen’s guidelines [35]. The primary concept of interest was fully IVR, defined by the use of head-mounted displays (e.g., Oculus Quest Rift). Studies combining other interventions (e.g., physical exercise, diet) were included if at least one intervention group used only IVR. Cognitive training was defined as repeated, guided practice of standardized tasks aimed at improving specific cognitive domains [36]. The context involved fully IVR cognitive training targeting multiple or specific cognitive domains and its effect on cognitive function. Outcome measures were required to assess cognitive function, including near or far transfer effects. Neurological measures related to cognitive domains of interest [e.g., electroencephalogram (EEG)] were also included. However, studies focusing solely on non-cognitive outcomes, such as activities of daily living, were excluded, as our study focuses on the impact of cognitive training on cognitive outcomes.
Search string.
| Block | PCC criteria | Search terms |
|---|---|---|
| #1 | Population | “Cognitive Dysfunction” [MeSH] OR “Dementia” [MeSH] OR “Cognitive Decline” [tw] OR “Cognitive Impairment” [tw] OR “Mild Cognitive Impairment” [tw] OR “Early onset Dementia” [tw] OR “Young Onset Dementia” [tw] |
| #2 | Context | “Cognitive Training” [MeSH] OR “Cognitive Training” [tw] OR “Cognitive Intervention” [tw] OR “Cognitive Rehabilitation” [tw] OR “Cognitive Stimulation” [tw] |
| #3 | Concept | “Virtual Reality” [MeSH] OR “Virtual reality” [tw] OR “Fully Immersive Virtual Reality” [tw] OR “Immersive Virtual Reality” [tw] OR “Virtual Technolog*” [tw] |
MeSH: Medical Subject Headings; tw: text word. *: truncation.
The search strategy was developed through discussions with the research team and guidance from an academic librarian. On June 20, 2024, the first author conducted searches across four databases: PubMed (Medline), Web of Science, PsycINFO, and PsycARTICLES. Additional searches were conducted using Taylor and Francis Online and Google Scholar. The search terms were designed to capture the population (MCI or dementia), concept (fully IVR cognitive training), and context (cognitive functioning), and were appropriately adapted for each database. In addition to database searches, relevant literature was identified through manual searches of reference lists, forward citation tracking of included studies, and existing reviews. Duplicates were automatically removed. The first and last authors independently screened titles and abstracts using Rayyan. They met on July 8, 2024, to review outcomes and resolve any conflicts from the initial screening. The full texts of the remaining studies were then independently reviewed by the same authors. On August 21, 2024, the authors met again to discuss their findings, resolve any conflicts by discussing their rationale, and confirm whether the studies met the eligibility criteria for final inclusion.
Following McHugh’s guidelines [37] for interpreting kappa values, the agreement between the first and last authors was appropriate. At the title and abstract screening stage, the kappa value was κ = 0.69, and at the full-text review stage, the agreement improved to κ = 0.84.
To address the research question, we created a data extraction table in Microsoft Word. This was designed to capture relevant information related to the study characteristics, cognitive training components, and main outcomes. The data extraction table included information on authors, publication year, county, study design, participant characteristics, head-mounted technology, cognitive training, training duration, outcome measures, main results, and comments on any additional information of interest. The first author independently extracted the data from the included articles, and this was subsequently reviewed and discussed with the last author to ensure accuracy and consistency in the data extraction process.
The PRISMA flow diagram shows the selection process for the scoping review. The search strings identified 816 articles, 8 were included in the review (see Figure 1). All studies included participants who were diagnosed with MCI or dementia. Table 2 provides a breakdown of all the included studies.
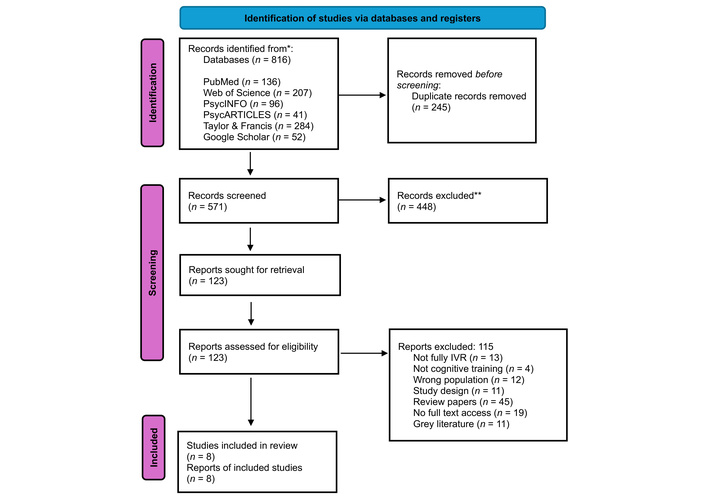
PRISMA flowchart for articles included in the scoping review. Adapted from [34]. © The Author(s) 2018. Licensed under a Creative Commons Attribution (CC BY 4.0). IVR: immersive virtual reality; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analysis. *: identified studies; **: excluded studies.
Characteristics of included studies.
| Author(s), publication year; country | Sample | Participants (n); mean age and SD | Study design | HMD technology | Cognitive training | Training duration (days × weeks × minutes) | Outcome measure | Main results | Notes |
|---|---|---|---|---|---|---|---|---|---|
| Park et al. [38], 2020; Republic of Korea | Amnestic MCI | Fully IVR (n = 10); 71.80 ± 6.61Control group (n = 11); 69.45 ± 7.45 | RCT | HTC Vive, VR controllers | Memory, executive function, processing speed, attention | 2 d × 12 w × 30 min | K-MMSEKorean Colour-Word Stroop TestSGDS-K | Within-group analysis did not indicate any significant change after 12 weeks. | Control group participants continued their normal activities.No clear theoretical framework or model was reported as the rationale for the intervention. The authors proposed some explanations for the non-significant results: 1) The relatively short intervention duration compared to studies with longer training periods (e.g., 6 months), 2) the intervention did not include physical exercise components, which the authors suggest may be critical for dementia prevention.Reported methodological limitation: small sample size. |
| Zhu et al. [39], 2022; China | MCI & MD | MCI (n = 18); 82.94 ± 6.44MD (n = 13); 85.76 ± 4.67 | Pretest-posttest study design | HTC Vive Pro Eye, VR controllers | Memory, attention, executive function, calculation ability | 3 d × 5 w × 20–30 min | MMSE & MoCAAVLTSTTSDMT | Within-group analysis indicated significant change after 5 weeks for both MCI and MD groups. | No control group was included in the study.No specific theory was used to explain the reported cognitive outcomes.However, the neural mismatch model was referenced to explain participants’ discomfort experienced in the fully IVR environment. The authors suggested that increasing exposure time during the session may help reduce discomfort and improve user adaptation.Reported methodological limitation: small sample size, lack of active comparison groups. |
| Zając-Lamparska et al. [40], 2019; Poland | MD | MD (n = 27); 72.04 ± 7.43Healthy adults (n = 72); 67.86 ± 5.83 | Pretest-posttest study design | Oculus Rift DK2, Xbox 6DOF control pad | Attention, memory, language, and visuospatial processing | 2 d × 4 w × 45 min | AttentionMemory, languageVisuospatial processing | Within-group analysis indicated some significant change after 4 weeks of fully IVR intervention for the MD group. There were some non-significant cognitive measures. | No control group was included for this fully IVR intervention. The cognitive training games used in the study were not described in full detail; however, a brief description of GRADYS training software is provided in Zając-Lamparska et al. [41]. No specific theoretical framework was used to explain the reported results.Reported methodological limitation: lack of an active comparison group. |
| Kang et al. [42], 2021; Republic of Korea | Predementia {MCI or Subject cognitive decline}* | Total (n = 41); 74.51 ± 5.81 | RCT | Oculus Rift CV1 display,Oculus Touch controllers | Attention, executive function, and memory | 2 d × 4 w × 20–30 min | MMSEAttentionLanguage abilityMemoryFrontal executive functionMRI | Within-group analysis indicated a significant change in verbal memory, language, and related functions, and TMT-B for the fully IVR group after 4 weeks of intervention. | A control group was included with participants continuing “business as usual”.The cognitive reserve model was used to provide the rationale for the study. The Van Sommers model was applied to explain improvements observed in the RCFT copy test, based on proposed links between visuospatial construction demands in the fully IVR environments and frontal-occipital functional connectivity.Reported methodological limitation: small sample size, lack of an active comparison group. |
| Maeng et al. [43], 2021; Republic of Korea | MCI | MCI (n = 31); 73.2 ± 7.3Healthy adults (n = 25); 71.6 ± 4.4 | Not reported | Samsung Odyssey HMD, motion controllers | Memory, attention, executive function | 8 sessions × 4 w × 50–60 min | CERAD-K (each cognitive domain) | Within-group analysis indicated significant change in some CERAD-K outcomes (Word list memory, word list recall, word list recognition, constructional recall, TMT-A, Stroop-C, Stroop-CW) after 4 weeks of intervention for the MCI group. | No control group was included in this study.There was no specific theoretical framework or model that was used. However, the authors examined the sense of presence, hypothesising that it would differ from that of cognitively normal individuals; however, no significant difference was found.Reported methodological limitation: small sample size, no follow-up tests. |
| Yang et al. [44], 2022; Republic of Korea | MCI* | Fully IVR (n = 33); 72.5 ± 5Exercise (n = 33); 67.9 ± 3.6Control (n = 33); 72.6 ± 5.6 | RCT | Oculus Quest headset, VR controllers | Attention, working memorySourced from Thapa et al. [30] (2020) | 3 d × 8 w × 100 min | MMSE TMT-ASDSTNCGG-FAT | Within-group analysis indicated a significant change in global cognitive function (MMSE, TMT-A, and SDST) after 8 weeks of training intervention. | Three comparison groups were included: exercise intervention group, a control group receiving 30-min educational seminars, and a fully IVR group.No specific theory was used to provide a rationale for the study or to explain the cognitive outcomes. However, the authors’ reference to the sense of presence to interpret observed neural-level changes in the brain.Reported methodological limitation: inconsistent intervention frequency, female-dominant sample. |
| Thapa et al. [30], 2020; Republic of Korea | MCI | Fully IVR (n = 34); 72.6 ± 5.4Control (n = 34); 72.7 ± 5.6 | RCT | Oculus Quest headset, VR controllers | Memory | 3 d × 8 w × 100 min | MMSE-DSNCGG-FATTMT-ATMT-BSDSTEEG recording | Within-group analysis indicated a significant change in global cognitive function (TMT-A, TMT-B, SDST) after 8 weeks of training intervention. | A control group was included; participants completed eight sessions of an educational program or general healthcare, delivered once per week, with each session lasting 30–50 min. The intervention group also received educational content. No specific theoretical framework or model was provided for the rationale or to explain the significant findings.Reported methodological limitation: no follow-up test during the intervention. |
| White and Moussavi [45], 2016; Canada | Individual with the onset stage of AD | 74-year-old male | Case study | Oculus Rift DK VRN, wheelchair motion sensors | Spatial navigation | 3 d × 7 w × 45 min | MoCA | The participant’s MoCA score increased from 24 to 26 after 7 weeks of training intervention. | The cognitive reserve model was used as the theoretical rationale for the study. The Morris water task was used as a model for IVR-based spatial navigation assessment. The authors suggested that including periodic “booster” sessions to maintain and reinforce any potential improvements in cognitive reserve. |
*: Studies that conducted a power analysis. AVLT: Auditory Verbal Learning Test; CERAD: Consortium to Establish a Registry for Alzheimer’s Disease; EEG: electroencephalogram; HMD: head-mounted display; IVR: immersive virtual reality; MCI: mild cognitive impairment; MD: mild dementia; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; NCGG-FAT: National Center for Geriatrics and Gerontology Functional Assessment Tool; RCFT: Rey-Osterrieth Complex Figure Test; RCT: randomized controlled trial; SD: standard deviation; SDMT: Symbol Digit Modalities Test; SDST: Symbol Digit Substitution Test; SGDS-K: Short Form Geriatric Depression Scale-Korean version; STT: Shape Trial Test; TMT: Trial-Making Test.
Among the eight included studies, seven articles implemented multi-domain cognitive training intervention targeting memory, attention, executive functioning, and visuospatial processing. White and Moussavi [45] was the only study that implemented a single cognitive training intervention, focused on visuospatial processing, following a case study design. Across the eight studies, the duration of individual sessions ranged from 20 to 100 min, with sessions delivered either two or three times per week. The total training duration ranges from 4 to 12 weeks.
All the included studies provided inclusion criteria for individuals with MCI or dementia. Of the included studies, the samples included MCI (K = 4), amnesic MCI (K = 1), predementia combining MCI and cognitive decline sample (K = 1), mild dementia (K = 2), and onset stage Alzheimer’s disease (K = 1). Maeng et al. [43] and Zając-Lamparska et al. [40] compared the sample group diagnosed with MCI and mild dementia (respectively) with the healthy adult sample group.
Out of the included studies, changes in global cognition (K = 5), memory (K = 5), attention (K = 6), visuospatial (K = 4), executive function (K = 6), and language (K = 4) were measured pre-and post- virtual reality cognitive training intervention (see Table 3 for all the cognitive measures). There were no consistent significant within-subject results across the outcome measures. Significant within-subject effects on global cognition were found in 2 studies (K = 2/5), on language ability were found in one study (K = 1/4), on executive function were found in five studies (K = 5/6), on visuospatial were found in three studies (K = 3/4), on attention were found in three studies (K = 3/6), on memory were found in four studies (K = 4/5). Park et al. [38] was the only study that found a non-significant difference pre- and post-fully IVR intervention across all cognitive outcome measures. White and Moussavi’s case study [45] found a change in global cognition, visuospatial ability, and memory, which were assessed quantitatively through tests [e.g., Montreal Cognitive Assessment (MoCA)] and qualitatively from the participant’s wife’s feedback. Four out of the eight studies included a control/comparison group. Two studies compared the virtual reality cognitive training intervention with an active educational program control. While the other two studies used a control group with a passive “business as usual” approach.
Cognitive domains and measures from scoping review (K = 8).
| Cognitive domain | Cognitive measures |
|---|---|
| Memory | Auditory Verbal Learning Test (AVLT)Digit Symbol test from Wechsler Adult Intelligence Scale-Revised (WAIS-R)Benton Visual Retention Test (BVRT)The Famous Faces TestDelayed recall [Rey-Osterrieth Complex Figure Test (ROCF/RCFT)]Seoul Verbal Learning Test (SVLT) |
| Attention | Symbol Digit Modalities Test (SDMT)Trial-Making Test Part A (TMT-A)Digit Symbol Test from WAIS-RColour Trial Test (CTT)The d2 Test of Attention |
| Visuospatial | Block Design test from WAIS-RROCF/RCFT—direct copying |
| Executive function | Shape Trial Test (STT)TMT-BStroop Colour TestPhonemic Word Fluency Testing |
| Language | Verbal Fluency from Addenbrooke Cognitive Examination III (ACE-III)Boston Naming Test (BNT) |
| Global cognition | Mini-Mental State Examination (MMSE)Montreal Cognitive Assessment (MoCA)Consortium to Establish a Registry for Alzheimer’s Disease (CERAD)National Center for Geriatrics and Gerontology Functional Assessment Tool (NCGG-FAT)Cognitive Assessment Screening Instrument (CASI)Clock Drawing Test-Drawing Part (CDT-D) |
Among the included studies, two (K = 2/8) explicitly referenced a cognitive theory or model. White and Moussavi [45] applied cognitive reserve theory and the Morris water task model to justify their focus on virtual cognitive training solely targeting spatial navigation. Their case study involving a patient with early-onset Alzheimer’s disease found improvement in the participant’s global cognition after the cognitive training, but the gains declined at a 28-week follow-up. They suggested that continued training sessions may help maintain cognitive reserve. Kang et al. [42] also highlighted cognitive reserve theory, proposing that continued cognitive practice could help restore cognitive reserve, which would improve overall cognition. Additionally, they introduced the Van Sommers model of drawing as a theoretical explanation for the observed improvements in participants’ performance on the Rey-Osterrieth Complex Figure Test copy task after the virtual cognitive training. While cognitive reserve was not explicitly measured in either study, Kang et al. [42] measured brain functional connectivity; findings showed increased connectivity within the visual network after training.
The present review aimed to explore the effectiveness of fully IVR cognitive training games for individuals living with MCI or dementia. The scoping review identified eight studies investigating changes in cognition in individuals with MCI or dementia following cognitive training delivered through IVR head-mounted displays. Global cognition was commonly measured using the Mini-Mental State Examination (MMSE) and MoCA, often together (Table 3). While improvements were reported across multiple cognitive domains, the most consistent positive changes were found in memory (4 out of 5 studies; 80%), executive functioning (5 out of 6; 83%), and visuospatial skills (3 out of 4; 75%). In contrast, improvements in global cognition were observed in only two out of five studies, suggesting that fully IVR cognitive training may potentially be more reliable in enhancing specific cognitive domains than overall cognitive ability. This pattern is consistent with prior literature on cognitive training, which has also highlighted domain-specific effects rather than improvements in global cognition. Regardless of how cognitive training is administered (face-to-face or CCT), evidence for the far transfer effect remains limited, with cognitive training only demonstrating improvements in specific trained cognitive domains [25]. Nevertheless, global cognition measures, like the MMSE, may not be as sensitive enough to demonstrate far transfer effects after cognitive training [46].
Theoretical grounding appears to remain limited, as only two studies explicitly referenced a cognitive theory or model. The cognitive reserve hypothesis was applied as a rationale for intervention and a framework for interpreting findings [42, 45]. However, cognitive reserve was not directly measured in either study, making it difficult to determine whether observed changes could be attributed specifically to the maintenance of cognitive reserve in participants. The lack of theoretical grounding in current studies presents an opportunity for future research to align intervention designs with established frameworks (e.g., cognitive reserve or the Van Sommers drawing model), which may provide a clearer rationale and strengthen the interpretation of observed cognitive behavioural changes. For instance, cognitive load theory is particularly relevant in fully immersive environments, as fully IVR technology can reduce cognitive demand by reducing the need for users to mentally transform information from 2D to 3D representations [16]. This also has direct implications for task design, including simplifying instructions or avoiding competing stimuli. Interestingly, the included studies varied slightly in their level of immersion, specifically in how the participant interacted with the virtual environment. Among the included studies, six articles used wireless handheld motion controllers (e.g., Oculus Touch controllers), and one used a controller without motion sensors (i.e., an Xbox controller pad [40]). In contrast, White and Moussavi [45] had their participant interact with the virtual environment using a specially designed wheelchair equipped with motion sensors [47]. Hand movement and controller type, in relation to level of immersion, were not initially considered during the conception of the scoping review. However, with the advancement of fully IVR technology, eliminating the use of controllers through hand tracking may be more feasible for individuals who are unfamiliar with the technology [48]. This may further help reduce the cognitive demands associated with learning controller-based instructions [40], making it an important design element for future research to consider. In addition to cognitive load theory, principles associated with neuroplasticity support the inclusion of adaptive difficulty progression, ensuring that training remains challenging across each session. Interestingly, across the included studies, difficulty progression varied; some studies did not explicitly mention difficulty progression (e.g., Thapa et al. [30]), while other studies used a fixed progression approach (e.g., Kang et al. [42]) or adjusted task difficulty based on previous performance (e.g., Zhu et al. [39]). Implementing adaptive approaches in task design across sessions and in-game may be valuable for people living with MCI or dementia, as this can account for individual differences in cognitive functioning and learning rate. However, caution needs to be adopted in implementing difficulty progression, as demanding tasks may reduce motivation or lead to decreased engagement, especially for individuals living with dementia. For those with more severe cognitive decline, designing engaging and emotionally positive virtual experiences [49], alongside responsive in-game adaptivity, may support sustained participation and improve performance outcomes. Overall, we propose that future research would benefit from more intentional and explicit application of theory to guide fully IVR cognitive task design, and selection of sensitive outcome indicators (see Table 4).
Conceptual table of the design elements and relevant theoretical frameworks involved in fully IVR cognitive training intervention.
| Design elements | Theoretical frameworks |
|---|---|
| Head-mounted displayHand tracking technologyIntegrated narrative storylineTraining durationLength of trainingDifficulty progressions | NeuroplasticityCognitive load theorySense of presenceSpatial navigation theoryThe Van Sommers modelCognitive reserveSelf-determination theory |
IVR: immersive virtual reality.
While this review highlights the promise of fully IVR cognitive training for individuals with MCI or dementia, there are several broader considerations to highlight during any development and implementation. Beyond cognitive outcomes, there may be indirect benefits with fully IVR in terms of economic benefits. The financial burden of dementia is substantial and is expected to rise in the coming years [2]; interventions that delay the progression of severe cognitive decline and promote independence may offer significant cost savings at the individual and societal level [21, 50]. A well-designed fully IVR cognitive training game can be self-administered, dependent on the severity of the condition, without the need for direct supervision by healthcare professionals. Findings from the present review revealed variations in the development and design elements of fully IVR cognitive training intervention, such as differences in training duration (i.e., minutes and days per week), length of training (i.e., number of weeks), difficulty progression, in-game adaptivity, and integration of narrative storyline. Given these variations, establishing consensus on the optimal core elements necessary for an effective fully IVR cognitive training intervention would be valuable. Future research exploring fully IVR cognitive training from a mechanistic perspective, rooted in theoretical grounding, could provide strong foundations for developers and researchers. For instance, designing cognitive tasks that specifically align with cognitive strategy training, rather than restorative practice-based training, may be more beneficial for individuals with MCI. Moreover, the scalability of the technology can allow for delivery in home-based or residential settings, reducing the need for travel to specialist clinic visits. The present review does not suggest that fully IVR cognitive training should be implemented in isolation. Rather, it is important to recognise the potential benefits of cognitive interventions as part of a holistic approach to nonpharmaceutical support for individuals living with MCI or dementia. This is consistent with the ecological models of care, which emphasize the importance of addressing the individuals within their broader interpersonal, physical, and environmental context. In this broader perspective, dementia has been discussed as a lifestyle-related disorder by some authors [51, 52]. A relatively recent concept, “vitaction”, is described as “vitamins for the brain”, referring to lifestyle-related actions that may support brain health (e.g., socializing, learning, having personal relationships, etc.) [53]. The concept proposes that deficiencies in vitaction (e.g., lack of interest in learning) may contribute to neurodegenerative diseases (i.e., Alzheimer’s disease), and supplementing these deficiencies with relevant vitaction could support brain health and potentially reduce dementia risk [52]. In this context, engagement with novel technology (i.e., fully IVR) represents an important component of modern lifestyle and may contribute to brain health depending on how it is used and designed for people living with MCI or dementia. Fully IVR cognitive training should be researched both as a standalone cognitive intervention and in terms of how they complement established care strategies and broader lifestyle-related approaches. That said, conducting experimental research in this population presents inherent challenges, particularly due to the variability and complexity of individual care plans, which are rarely standardized (see Table 2 for some reported methodological limitations). Beyond the focus on within-subject comparison in the present review, establishing an active comparison group when assessing the effectiveness of fully IVR cognitive training would strengthen the evidence of integrating fully IVR into care plans. It is also essential to collect contextual information regarding participants’ engagement with other therapies or activities, for example, their diet or physical engagement. Among the studies included in this review, only the case study [45] collected qualitative data outside of just cognitive measures; the participant’s wife reported changes in driving performance and involvement with other activities.
The economic and contextual factors are important to consider in the future of fully IVR cognitive training. However, there are other factors that should be equally considered, such as data protection and ethics. Policymakers should begin to establish regulatory frameworks that ensure safe use of IVR technologies and support initiatives that promote digital literacy within the population. For instance, digital exclusion is still a concern, as individuals living with MCI or dementia in underserved communities may face significant challenges accessing the technology required for fully IVR cognitive interventions. Furthermore, it is essential that these cognitive training tools are co-designed with, rather than merely for, individuals living with MCI or dementia to ensure that their voices, preferences, and lived experiences are integrated into development [54–56].
The present scoping review provides a summary of the literature on fully IVR cognitive training for individuals living with MCI or dementia. Although the number of included studies was sparse, the findings highlight the potential of fully IVR to enhance specific cognitive domains, such as memory, executive functioning, and visuospatial abilities. Overall, these findings offer a valuable foundation for advancing research and practice in this field. Future research should aim to establish consensus on the optimal elements necessary for designing and developing fully IVR cognitive training for this population and to conduct experimental research examining the impact of specific key design elements. The present review contributes to the growing literature supporting the use of fully IVR as a promising tool for cognitive intervention. The authors aim to build upon these insights by developing a fully IVR cognitive training game adopting a co-design approach with individuals with lived experience. With continued development and evaluation, fully IVR may become a significant tool for maintaining or enhancing cognitive functioning and quality of life for individuals affected by MCI or dementia. The future of cognitive care must be guided not only by advanced technologies but also by compassion, ensuring that these novel interventions are co-designed, equitable, and grounded in the lived experience of those they intend to support.
CCT: computerized cognitive training
IVR: immersive virtual reality
MCI: mild cognitive impairment
MMSE: Mini-Mental State Examination
MoCA: Montreal Cognitive Assessment
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analysis
EACO: Conceptualization, Methodology, Formal analysis, Investigation, Writing—original draft, Project administration, Writing—review & editing. RK: Methodology, Validation, Writing—review & editing. AP: Methodology, Validation, Writing—review & editing. BTS: Supervision, Validation, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflict of interest.
Not applicable.
Not applicable.
Not applicable.
The datasets supporting the findings of this study are available from the corresponding author upon reasonable request.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 2724
Download: 19
Times Cited: 0
