Original Article
Original Article

Affiliation:
1Department of Orthopedics and Traumatology, Erasme University Hospital, 1070 Brussels, Belgium
ORCID: https://orcid.org/0000-0001-7163-3794
Affiliation:
2Department of Orthopedics and Traumatology, EpiCURA Baudour, Hornu and Ath Hospitals, 7331 Mons, Belgium
ORCID: https://orcid.org/0009-0000-9999-1104
Affiliation:
1Department of Orthopedics and Traumatology, Erasme University Hospital, 1070 Brussels, Belgium
ORCID: https://orcid.org/0000-0001-6356-4645
Affiliation:
2Department of Orthopedics and Traumatology, EpiCURA Baudour, Hornu and Ath Hospitals, 7331 Mons, Belgium
3Medical Faculty, University of Mons, 7000 Mons, Belgium
ORCID: https://orcid.org/0000-0001-9402-6401
Affiliation:
2Department of Orthopedics and Traumatology, EpiCURA Baudour, Hornu and Ath Hospitals, 7331 Mons, Belgium
Email: sagimartinov@gmail.com
ORCID: https://orcid.org/0000-0001-8191-950X
Explor Musculoskeletal Dis. 2026;4:1007127 DOI: https://doi.org/10.37349/emd.2026.1007127
Received: November 16, 2025 Accepted: May 05, 2026 Published: June 30, 2026
Academic Editor: Ashok N. Johari, Children’s Orthopaedic Centre, India
The article belongs to the special issue Innovation in Orthopedics
Aim: Distal locking during intramedullary nailing remains a technically demanding step. The aim of this study was two-fold: first, to evaluate whether the proposed locking technique reduces radiation exposure and operative duration compared with the conventional free-hand technique across surgeons with different levels of experience; second, to compare its performance with previously published alternative distal locking methods.
Methods: A retrospective observational study was conducted across three trauma centers in Belgium. A total of 432 patients undergoing intramedullary nailing for long-bone fractures were included. Thirty surgeons (10 junior residents, 10 senior residents, 10 board-certified surgeons) performed distal locking using both the conventional free-hand technique and the proposed method. Radiation exposure and procedure duration were recorded and compared. Results were also compared with published data on alternative distal locking techniques.
Results: The proposed technique significantly reduced radiation exposure, fluoroscopy time, and procedure duration across all experience levels. Mean radiation dose decreased from 35.47 ± 8.9 to 4.43 ± 1.1 cGy/cm2 (p < 0.0001). Fluoroscopy time decreased from 19.33 ± 6.2 to 11.5 ± 2.0 seconds (p = 0.003). Procedure duration decreased from 9.53 ± 3.1 to 4.23 ± 1.2 minutes (p < 0.0001). The greatest improvement was observed among less experienced surgeons. Compared with published techniques, the method demonstrated non-inferior or superior results in terms of radiation exposure and procedure duration.
Conclusions: This simple and reproducible technique significantly reduces radiation exposure and operative time compared with the free-hand method. By eliminating the need to obtain a nearly perfectly round fluoroscopic image of the locking hole, the technique relies on hand-eye coordination and cognitive alignment rather than fixed geometric positioning. It requires fewer adjustments and repositioning of the C-arm. Its performance is comparable or superior to alternative techniques. It requires no additional equipment, making it practical for routine trauma practice.
Intramedullary nailing (IMN) is widely used for the management of long-bone fractures, providing stable fixation and early mobilization [1]. Distal locking preserves fracture reduction, prevents shortening, and increases stability. However, it remains a technically demanding step of the procedure, heavily relying on fluoroscopy use, particularly for less experienced surgeons [1]. The free-hand technique is still the most commonly used method for distal screw insertion. The reliance on fluoroscopy during standard free-hand distal locking exposes both patients and operating room staff to ionizing radiation, highlighting the need for exposure reduction. We present a simple and reproducible distal locking technique that requires only standard surgical tools and a conventional C-arm. By eliminating the need to visualize a nearly perfectly round locking hole, this technique avoids continuous fluoroscopy and cumbersome C-arm manipulation, resulting in a substantial reduction in both procedural time and radiation exposure.
The primary aim of this study was to evaluate whether this technique could significantly reduce radiation exposure, fluoroscopy, and operative duration compared with the conventional free-hand method across surgeons with varying levels of experience. In addition, we compared the radiation exposure and surgical duration with previously published alternatives for distal screw insertion, including targeting devices [2, 3], electromagnetic navigation [4–7], mixed-reality navigation [8], laser guidance [9], endoscopy-assisted techniques [10], the Kirschner wire method [11], fluoroscopy-free approaches [12], the Steinmann pin technique [13], and computer-assisted 3D-printed guides [14]. Although the techniques that rely on newer technology have demonstrated effectiveness, many require costly equipment and/or advanced training, limiting their routine use in daily trauma practice. Alternative techniques, including those using Kirschner wires, Steinmann pins, or fluoroscopy-free approaches, represent relevant alternatives to the conventional free-hand method. Given their previously established technical feasibility, these techniques were selected for comparison with our method in terms of radiation exposure and procedure duration. The novelty of this technique lies in its reliance on hand-eye coordination and on cognitive alignment rather than on additional tools for locking screw insertion.
We hypothesized that the proposed technique would achieve efficiency that is comparable to, or greater than, conventional free-hand distal locking. Further, we sought to demonstrate that this technique is not inferior to other distal locking techniques with respect to ionizing radiation and procedure duration.
This retrospective observational study was conducted at three orthopedic trauma centers in Belgium (EpiCURA Hospitals: Hornu, Baudour, and Ath). Procedures were performed between January 2024 and May 2025. The study evaluated distal locking during IMN performed as part of routine trauma care.
A total of 432 patients undergoing IMN for acute diaphyseal or distal/unstable metaphyseal long-bone fractures were included. Patients were adults aged 35.7 ± 14.3 years. The male to female ratio was 65:35. A total of 203 femoral, 181 tibial and 48 humeral fractures were analyzed. Patients under 18 years were excluded. Cases in which longer nails were used for revision surgery were excluded. No pathological fractures were included.
Thirty orthopedic and trauma surgeons participated in the study and were stratified according to experience level: ten junior residents (1–3 years), ten senior residents (4–6 years), and ten board-certified surgeons (7–22 years). Each surgeon performed distal locking using both the conventional free-hand technique and the proposed technique during the study period. The described technique was chosen for residents or seniors when one of the authors was attending.
Each surgeon performed 3–10 distal locking procedures of various long bones using the free-hand technique. This required positioning the C-arm perpendicular to the limb, often using a continuous fluoroscopic mode, to visualize a round locking hole. The same surgeons also performed 4–13 procedures using our method (Figure 1).
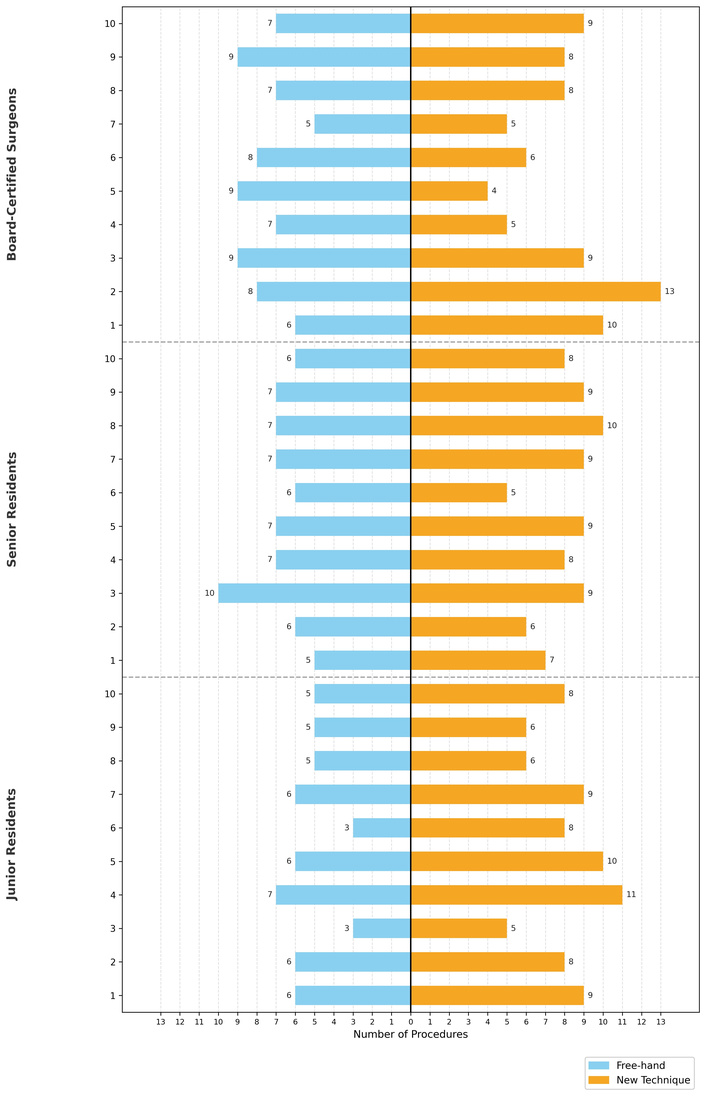
Number of free-hand and proposed technique procedures. On the y-axis, three groups of surgeons are presented with ascending level of experience: junior residents (1 to 10), senior residents (1 to 10), and board-certified surgeons (1 to 10). On the x-axis, the number of procedures performed using free-hand or the technique described in this article.
The distal locking part of the surgery was measured in minutes. Surgical duration was calculated from the time signature of the C-arm, the time elapsed between the first image taken of the distal part of the bone and the last image controlling the final construct. The duration of radiation exposure was measured in seconds, and the dose of ionizing radiation exposure was recorded in cGy/cm2, both parameters read from the intraoperative fluoroscopy units used during surgery.
Commercially available intramedullary nail systems were used, including implants from the following manufacturers: Stryker T2 femoral, T2 tibial and T2 humeral nails, Stryker Gamma 3 long nail (Kalamazoo, MI, USA), Zimmer Biomet Affixus long femoral nail (Warsaw, IN, USA), DePuy Synthes MultiLoc Humerus nail (Oberdorf, Switzerland). Nail selection was based on fracture characteristics and surgeon preference.
All procedures were performed using standard orthopedic surgical instruments and a mobile fluoroscopy unit (Siemens Arcadis Varic C-arm or equivalent models available at the participating institutions). No dedicated targeting devices, navigation systems, or additional equipment were used.
Quantitative variables were first assessed for normality using the Shapiro-Wilk test. Normally distributed data were compared between the two groups using the Student’s t-test (two-tailed, unpaired). Non-normally distributed data were compared using the Mann-Whitney U test. Data were presented as means ± standard deviation (SD). A p-value < 0.05 was considered statistically significant.
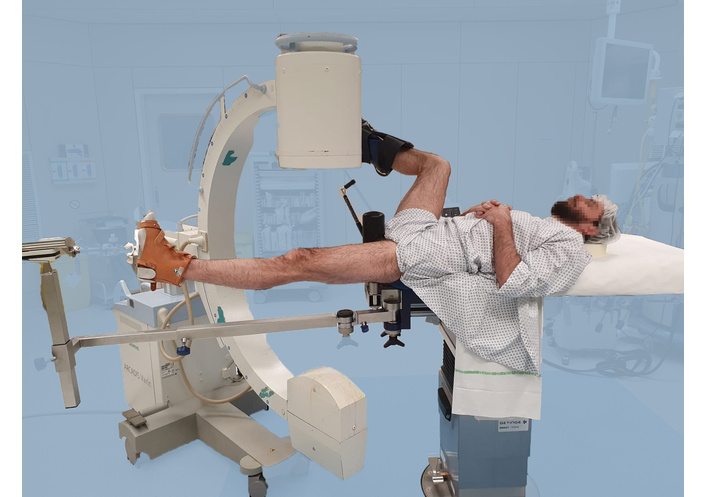
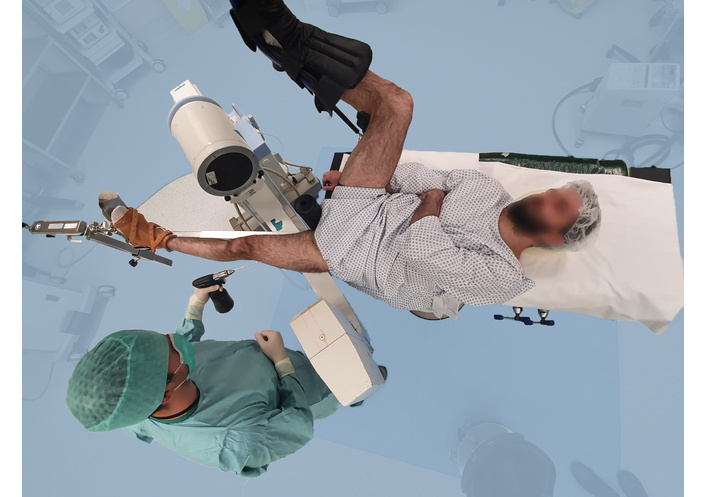
Step 1. Position patient and prepare limb in standard IMN setup (Figure 2). Femoral fracture IMN installation on a fracture table is shown in this example. C-arm is positioned for anteroposterior (AP) view, and the nail is introduced in the classic manner. The key advantage of this technique is that the C-arm positioning does not require strict perpendicular alignment with the limb of the patient. This avoids excessive flexion of the contralateral hip and makes C-arm positioning easier for the radiology assistant.
Step 2. Take an AP fluoroscopic image with a scalpel placed in a coronal plane in the approximate position. Based on the scalpel position relative to the nail locking holes, which are visible as notches on the AP image, make a longitudinal lateral incision to gain access to the distal locking holes. The lateral aspect of the notch of a locking hole is indicated in red inside a red circle (Figure 3).
Step 3. Place drill bit on cortex opposite visible AP notch of locking hole; maintain bone contact (Figures 4 and 5).
Step 4. Once the drill is positioned in front of the notch, keep the drill tip in contact with the bone. Deviate the power tool distally to bring the C-arm into a lateral view (Figures 6 and 7).
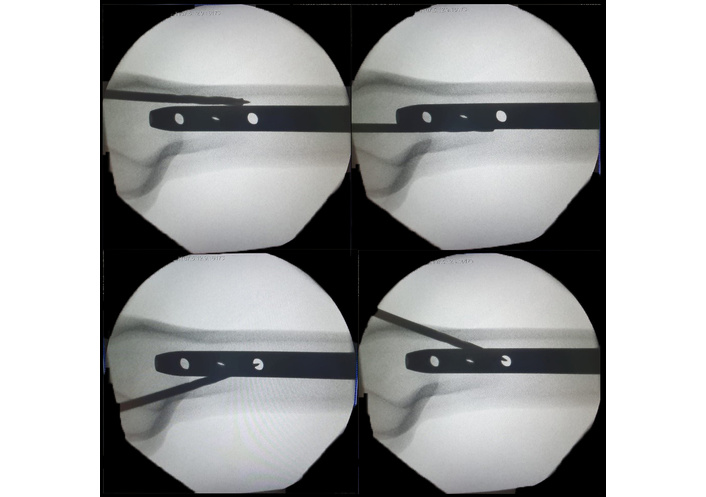
Step 5. While the power tool is in this deviated (tangential) position, adjustments to the lateral view are performed. The drill is placed in a continuous line with the nail. Commonly seen pictures are depicted in Figure 8. Top left the drill is too anterior. Top right—too posterior. Bottom left and right pictures show the power tool being too ascending or descending, respectively. On this lateral view, the adjustments are made. Note that the “perfectly” round locking hole was never searched.
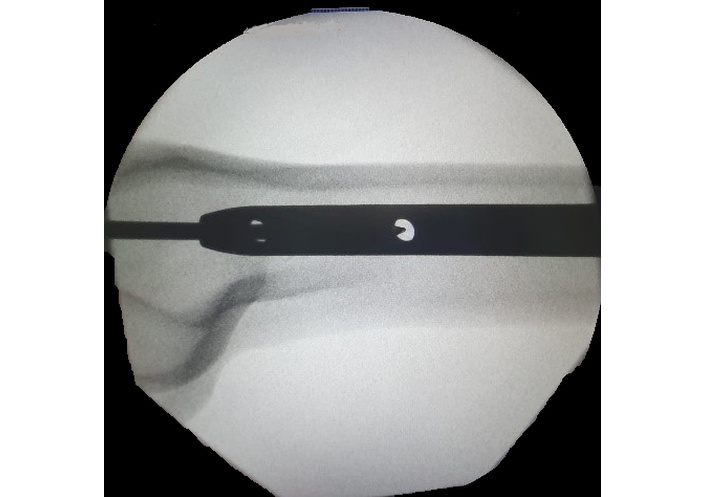
Step 6. Once the position in the lateral plane is correct and the drill bit is in line with the nail (Figure 9), position the drill perpendicular to the nail axis, keeping in mind proper coronal and sagittal alignment (Figures 10 and 11). Advance the drill bicortically. The tapered design of the locking hole allows for minor deviations in alignment during drilling and screw placement (Figure 12).
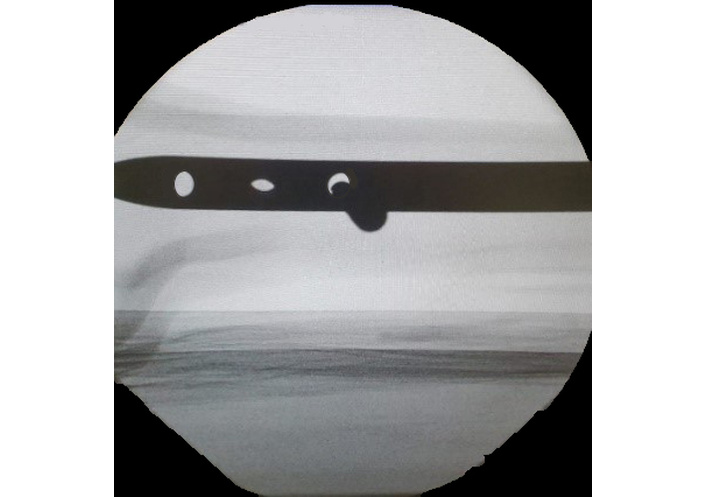
A fluorograph before drilling. Note that the holes do not need to be “perfectly” round for the drilling.
Step 7. To place the second screw, the C-arm can be kept in a lateral position and the drill left in place and detached from the power tool to provide the orientation for the second screw. The AP orientation and the axis of drilling are based on the position of the first drill. The only missing parameter is the distal-proximal placement. After the initial positioning of the second drill, obtain an image. Adjust proximally or distally as needed and advance the drill parallel to the placement of the first drill. If there is any uncertainty in placement or if a second drill piece is not available, repeat steps 3–8.
Step 8. Measure screw length, insert screws, and confirm placement with AP/lateral fluoroscopy. The rest of the procedure is standard.
The results comparing the free-hand and technique described here in terms of radiation dose, radiation and procedure duration are presented in Table 1.
Relative reduction in radiation dose, radiation and procedure duration with our method compared to free-hand (mean ± SD).
| Parameter | Surgeon experience | Free-hand mean ± SD | Our method mean ± SD | Relative reduction ratio (%) | p-value |
|---|---|---|---|---|---|
| Radiation dose (cGy/cm2) | Junior residents | 47.2 ± 5.8 | 5.1 ± 1.2 | 89.2 | - |
| Senior residents | 35.7 ± 4.6 | 4.7 ± 1.0 | 86.8 | - | |
| Board-certified surgeons | 23.5 ± 3.9 | 3.5 ± 0.9 | 85.1 | - | |
| Radiation time (s) | Junior residents | 26.5 ± 3.1 | 13.6 ± 2.2 | 48.7 | - |
| Senior residents | 19.4 ± 2.8 | 12.0 ± 1.9 | 38.1 | - | |
| Board-certified surgeons | 12.1 ± 1.7 | 9.0 ± 1.4 | 25.6 | - | |
| Procedure duration (min) | Junior residents | 12.4 ± 1.9 | 5.6 ± 1.1 | 54.8 | - |
| Senior residents | 10.1 ± 1.6 | 4.7 ± 1.0 | 53.5 | - | |
| Board-certified surgeons | 6.1 ± 0.9 | 2.4 ± 0.6 | 60.7 | - | |
| Radiation dose (cGy/cm2) | Mean (all participants) | 35.47 ± 8.9 | 4.43 ± 1.1 | 87.5 | < 0.0001 |
| Radiation time (s) | 19.33 ± 6.2 | 11.5 ± 2.0 | 40.5 | 0.003 | |
| Procedure duration (minutes) | 9.53 ± 3.1 | 4.23 ± 1.2 | 55.6 | < 0.0001 |
cGy/cm2: centigray per square centimeter.
We further analyzed the results available in the literature for distal locking using different methods. Comparative values presented in Table 2 were extracted directly from original peer-reviewed publications and are reported using the measurement units and outcome definitions used in each study. Radiation metrics (dose-area product, emitted dose, effective dose) differ across studies and are presented in original units; direct numerical comparison between studies is therefore limited. Our study results are presented in the last row of Table 2.
The results of distal locking from the literature comparing free-hand and other targeting devices to our technique.
| Study | Technique | Year | Radiation metric (as reported) | Fluoroscopy time (s) | Distal-locking time |
|---|---|---|---|---|---|
| Boraiah et al. [2] | Free-hand | 2009 | Not reported | 28.9 ± 16.4 | 12.1 ± 3.2 min |
| Boraiah et al. [2] | Targeting device | 2009 | Not reported | 9.2 ± 4.9 | 7.1 ± 2.4 min |
| Ehlinger et al. [3] | Targeting device | 2013 | DAP 241.3 mGy/cm2* | 13.5 (median) | Not reported |
| Maqungo et al. [4] | Electromagnetic navigation | 2014 | Emitted dose 230.5 mGy | 7 | 11.0 min |
| Grimwood and Harvey-Lloyd [5] | Electromagnetic navigation | 2016 | DAP reduction reported† | 10 | 3.28 min |
| Wang et al. [6] | Free-hand | 2018 | Not reported | 2.13 ± 0.73 | 5.89 ± 2.02 min |
| Wang et al. [6] | Electromagnetic navigation | 2018 | Effective dose 22.7 mSv | 40.41 ± 25.55 | Not reported |
| Davut and Doğramacı [10] | Endoscopy-assisted | 2021 | Not reported | 2 | 3.73 min |
| Gao et al. [9] | Laser navigation | 2022 | Not reported | 46.5 | 10.0 min |
| Shang and Wang [11] | Kirschner wire technique | 2023 | Not reported | Not reported | 27.82 min |
| Menekse [12] | Fluoroscopy-free | 2023 | 0 | 0 | Entire procedure‡ |
| Deslivia et al. [13] | Steinmann pin + hammer | 2024 | Lower vs free-hand§ | Not reported | Shorter vs free-hand§ |
| This study | Proposed method | 2025 | DAP 4.43 cGy/cm2 | 11.5 ± 2.0 | 4.23 ± 1.2 min |
DAP: dose-area product. *: Radiation units are reported exactly as published; values were not converted unless explicitly stated in the original article. †: Grimwood and Harvey-Lloyd [5] reported relative reductions in DAP rather than absolute mean values. ‡: Menekse [12] reported fluoroscopy-free distal locking; operative time corresponds to the entire procedure, not isolated distal locking. §: Deslivia et al. [13] reported statistically significant reductions in radiation exposure and distal-locking time compared with free-hand technique (p < 0.05), but did not publish numerical mean values; therefore, only directional outcomes are reported here.
The present study evaluated a simplified distal locking technique designed to reduce dependence on continuous fluoroscopy and complex C-arm manipulation while using only standard operative equipment. In line with our hypothesis, the proposed method significantly reduced radiation exposure, fluoroscopy and surgical duration compared with the conventional free-hand technique, across surgeons with varying levels of experience. Moreover, it showed a non-inferior result when compared with other techniques published in recent literature.
The magnitude of these reductions is clinically relevant, particularly in high-volume trauma settings. Distal locking is one of the most fluoroscopy-dependent steps of IMN, and prolonged exposure contributes to cumulative ionizing radiation for both patients and operating room staff. The observed decrease in fluoroscopy time and radiation dose therefore represents an important safety advantage. Notably, the greatest absolute improvements were observed among less experienced surgeons, suggesting that the technique may help standardize performance and reduce variability during training. This may also reflect greater adaptability among less experienced surgeons and less reliance on established habits.
The effectiveness of the proposed approach appears to stem from its underlying principle: eliminating the need to achieve a nearly perfectly round fluoroscopic image of the locking hole. It has been shown that fluoroscopy-guided procedures can be optimized through enhanced hand-eye coordination and cognitive alignment rather than reliance on fixed geometric positioning [15]. By prioritizing relative drill-to-nail alignment rather than repeated geometric correction, the technique reduces iterative adjustments, continuous imaging, and extensive C-arm repositioning. This simplified workflow likely explains both the reduction in operative duration and radiation exposure.
Multiple alternative strategies for distal locking have been reported, including mechanical targeting devices, electromagnetic navigation, laser guidance, endoscopy-assisted techniques, fluoroscopy-free methods, and computer-assisted or 3D-printed guides. While many of these techniques have demonstrated effectiveness in reducing fluoroscopy use, they often rely on additional equipment, higher costs, or advanced training. When compared with distal locking techniques reported in the recent literature, the proposed method demonstrated non-inferior performance with respect to radiation exposure and procedural duration, while requiring no additional equipment.
This study has limitations. Its retrospective design and non-randomized technique selection may introduce selection bias. Radiation exposure was assessed indirectly through fluoroscopy unit metrics rather than direct staff dosimetry. In addition, although the technique was applied across different bones and nail systems, the study was not powered for bone-specific subgroup analyses. Furthermore, distal locking time is difficult to isolate from the overall procedure, and inconsistent reporting across studies may introduce variability.
Prospective studies incorporating precise radiation measurements, complication rates, direct occupational exposure, and cost assessment would further strengthen these findings.
In conclusion, consistent with our initial hypothesis, this simple and reproducible distal locking technique reduced radiation exposure and surgical duration compared with conventional free-hand locking. Furthermore, its performance was non-inferior to that of other distal locking techniques reported in the literature with respect to these parameters. Its ease of implementation and favorable safety profile make it a practical option for everyday trauma practice.
AP: anteroposterior
IMN: intramedullary nailing
SD: Conceptualization, Investigation, Writing—original draft. LF: Data curation, Investigation. HM: Conceptualization, Methodology. JH: Formal analysis, Resources, Software. SM: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. All authors read and approved the submitted version.
The authors have no conflicts of interest to declare that are relevant to the content of this article.
The study was approved by the Ethics Committee of EpiCURA Hospitals (approval number P2025/025) and was conducted in accordance with the Declaration of Helsinki.
Informed consent to participate in the study was obtained from all participants, including the colleague modeling for illustrations.
Informed consent to publication was obtained from the participants.
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 350
Download: 18
Times Cited: 0
Ali Yüce ... Abdülhamit Misir
Tanja Neussl ... Johannes Dominikus Pallua
Ashok N. Johari
Ashok N. Johari, Ritesh A. Pandey