 Mini Review
Mini Review

Affiliation:
1International Sonoguide Pain School, Tehran 1951799864, Iran
Email: helengharaei@gmail.com
ORCID: https://orcid.org/0000-0001-5379-8667
Affiliation:
2Department of Radiology, Sri Aurobindo Institute of Medical Science, Saims Indore 453555, Madhya Pradesh, India
ORCID: https://orcid.org/0009-0002-1085-9882
Affiliation:
1International Sonoguide Pain School, Tehran 1951799864, Iran
ORCID: https://orcid.org/0009-0004-7822-5928
Affiliation:
3Tata Memorial Hospital, Mumbai 400 012, Maharashtra, India
4Urgent Care at the Estates, St. George BB19136, Barbados
ORCID: https://orcid.org/0009-0001-7489-775X
Explor Musculoskeletal Dis. 2026;4:1007126 DOI: https://doi.org/10.37349/emd.2026.1007126
Received: March 14, 2026 Accepted: May 27, 2026 Published: June 22, 2026
Academic Editor: Carlo Massaroni, Università Campus Bio-Medico di Roma, Italy
The article belongs to the special issue Data-Driven and AI-Based Approaches for Musculoskeletal Disease Monitoring and Rehabilitation
Precision Spine Care integrates individualized diagnostics and interventions tailored to the unique anatomical and clinical characteristics of each patient. Recent advances in artificial intelligence (AI) and machine learning are addressing these challenges by enabling automated image interpretation, tissue segmentation, quantitative analysis of muscular and fascial features, and longitudinal tracking of structural and functional changes. These AI-driven capabilities support objective assessment, early detection of pathology, personalized rehabilitation planning, and continuous monitoring of treatment response. This approach becomes increasingly complex when incorporating advanced interventional techniques such as ultrasound-guided pain injections and AI tools. AI facilitates automated image interpretation, tissue characterization, and structure recognition, improving efficiency and diagnostic consistency. Augmented reality (AR) and mixed reality (MR) technologies enhance spatial orientation, procedural guidance, and anatomy education, while tele-ultrasound expands access to expert consultation, imaging support, and training in underserved regions. Although ultrasound remains operator dependent and AI outputs require ongoing physician oversight, the integration of ultrasound with AI, AR/MR, and telemedicine represents a significant advancement in spine care. These technologies complement traditional anatomical and clinical approaches, improving diagnostic accuracy, procedural precision, and personalized rehabilitation strategies. As healthcare systems face increasing demand and workforce constraints, technology-assisted ultrasound is positioned to play a pivotal role in advancing spine assessment, education, and comprehensive spine-focused musculoskeletal management. Ultimately, AI, ultrasound, and telemedicine serve to augment, not replace clinicians, enabling precision spine care that is safe, effective, and patient-centered.
Precision spine care is reshaping musculoskeletal medicine by advancing from generalized treatment paradigms toward individualized diagnostic and therapeutic strategies tailored to each patient’s unique anatomical, clinical, genetic, psychosocial, lifestyle, and environmental profile [1–5]. This shift is particularly relevant in the management of chronic low back pain, where heterogeneous pain mechanisms, variable treatment responses, and under-recognized contributors, such as thoracolumbar fascia dysfunction, often limit the effectiveness of standardized approaches [4, 5].
Precision medicine offers a framework for addressing this complexity by integrating advanced imaging, interventional techniques, and data-driven decision support. Musculoskeletal ultrasound has emerged as a key enabling technology within Precision Spine Care. Beyond its established role in ultrasound-guided interventional pain procedures, ultrasound provides real-time, radiation-free assessment of spine-related muscles and fascial structures [6, 7]. It allows dynamic evaluation of muscle morphology, thickness, echogenicity, fatty infiltration, and functional behavior during movement, offering clinically meaningful insights into neuromuscular dysfunction, degeneration, and load-transfer abnormalities that are not captured by static imaging modalities. Ultrasound-guided spinal interventions have demonstrated accuracy comparable to fluoroscopy for soft-tissue targets, while avoiding radiation exposure and improving procedural flexibility. However, technical limitations persist, including operator dependence, reduced visualization of deep structures, and challenges in obese patients [8–12].
Despite its clinical value, conventional musculoskeletal ultrasound remains largely qualitative, limiting reproducibility, standardization, and scalability, particularly for longitudinal monitoring and large-scale implementation. Recent advances in artificial intelligence (AI) and machine learning are addressing these challenges by enabling automated image interpretation, tissue segmentation, quantitative analysis of muscular and fascial features, and longitudinal tracking of structural and functional changes. These AI-driven capabilities support objective assessment, early detection of pathology, personalized rehabilitation planning, and continuous monitoring of treatment response.
This article examines the role of AI-driven spine ultrasound in musculoskeletal monitoring, emphasizing clinical evaluation techniques, ultrasound-guided interventional procedures, and the ethical integration of AI into spine care. By combining real-time ultrasound imaging with data-driven analysis, spine assessment is evolving from an operator-dependent, descriptive modality into an objective and scalable tool for precision musculoskeletal medicine, supporting personalized, patient-centered, and ethically responsible spine care.
AI applications in spine care extend beyond ultrasound analysis to include diagnostic support (e.g., magnetic resonance imaging [MRI] interpretation), treatment outcome prediction, automated clinical documentation, consent generation, and decision support for interventional strategies. While these tools hold significant promise, their clinical integration raises important ethical concerns related to informed consent, data privacy, algorithmic transparency, and accountability [13]. Moreover, current evidence suggests that AI models demonstrate only moderate accuracy in diagnosing complex spinal conditions, underscoring the necessity for rigorous validation and responsible implementation within clinical workflows [14].
In parallel, ultrasound remains a widely used imaging modality in clinical practice due to its portability, accessibility, and real-time imaging capability, particularly in limited-resource and point-of-care settings where it provides important diagnostic and procedural support [14]. Its established role in these environments underscores its continued relevance alongside emerging AI-enabled approaches in spine and musculoskeletal care.
Recent advances in AI, particularly deep learning and big data analytics, have further accelerated the evolution of tele-ultrasound platforms. AI-enhanced systems can support automated image optimization, real-time procedural guidance, tissue recognition, and quantitative analysis, reducing operator dependence and improving consistency. AI-enhanced spine ultrasound also offers opportunities in education, tele ultrasound, and workforce augmentation. By integrating real-time imaging with automated guidance, annotation, and feedback, AI-supported ultrasound platforms can bridge the gap between anatomical knowledge and clinical application. This is particularly relevant in settings with limited access to specialized musculoskeletal or pain medicine expertise, where AI-assisted imaging and remote monitoring may expand access to high-quality care while improving consistency and efficiency.
Telemedicine has evolved substantially over the past five decades, transforming healthcare delivery by overcoming barriers related to geography, workforce shortages, and cost. Its integration across multiple medical domains has enabled high-quality care in settings with limited access to specialized providers. Ultrasound, as a portable, cost-effective, and radiation-free imaging modality, aligns particularly well with telemedicine applications, giving rise to tele-ultrasound, defined as the remote acquisition and interpretation of ultrasound images with real-time audio-visual guidance from an expert operator. Systematic reviews suggest that remotely supervised ultrasound is not consistently inferior to traditional in-person ultrasound services, with diagnostic image quality generally sufficient for clinical decision-making even in resource-limited environments [15, 16].
Available evidence indicates that the physical distance between the scanning site and the expert interpreter does not significantly affect diagnostic effectiveness, supporting the feasibility of tele-ultrasound as an alternative or adjunct to conventional imaging models in underserved settings [15]. Although the overall quality of evidence remains moderate and heterogeneous, these findings reinforce the potential role of tele-ultrasound in expanding access to diagnostic imaging where conventional services are unavailable or inconsistent. In spine care and pain medicine, AI-integrated telemedicine platforms offer opportunities for objective pain assessment, decision support, and standardized musculoskeletal evaluation [17]. However, the integration of AI into remote care environments also raises ethical and regulatory concerns, including data security, informed consent, algorithmic transparency, and protection of vulnerable patient populations [18].
Tele-ultrasound has demonstrated particular value in medical education and point-of-care ultrasound (POCUS) training. Multiple studies have shown that tele-ultrasound-based education is comparable to traditional in-person instruction in terms of learner performance, skill acquisition, and cognitive workload. Tele-education has been well accepted by learners and has proven effective for teaching both diagnostic and procedural ultrasound skills, supporting its role as a scalable alternative to conventional training models [19–22].
These findings have important implications for workforce development, particularly in regions with limited access to experienced sonographers or educators. In rural and resource-limited settings, tele-ultrasound addresses critical disparities in access to diagnostic imaging. Rural general practitioners and prehospital providers often lack sufficient imaging resources and trained personnel. Tele-mentored handheld ultrasound systems have demonstrated feasibility and clinical utility, enabling non-expert operators to acquire diagnostically meaningful images under remote expert guidance [23]. Similarly, prehospital tele-ultrasound models, where paramedics perform ultrasound examinations with real-time specialist support, have shown promise in facilitating earlier diagnosis, improving triage, and streamlining treatment pathways for patients in geographically isolated regions [24, 25].
Technological innovations such as robot-assisted tele-echography and mixed-reality tele-ultrasound represent emerging frontiers in remote imaging. Robot-based systems allow specialists to remotely manipulate ultrasound probes with force feedback, enabling reliable examinations from isolated sites and small healthcare centers [26]. Mixed-reality and human teleoperation models further extend this concept by allowing experts to guide novice operators through immersive visual and haptic interfaces across large geographic distances, demonstrating high feasibility and image quality even with inexperienced scanners [27]. While these technologies remain in early stages of clinical adoption, they highlight the expanding technical possibilities of remote ultrasound practice.
Despite these advances, challenges remain. Concerns persist regarding operator variability, image quality assurance, cybersecurity, medicolegal responsibility, and standardization of training. Although current evidence does not demonstrate that tele-ultrasound is inferior to in-centre imaging, further high-quality, condition-specific studies are needed, particularly in musculoskeletal and spine applications [15, 16]. The integration of AI into tele-ultrasound workflows may help address several of these limitations by enhancing standardization, reducing operator dependency, and enabling objective, longitudinal musculoskeletal monitoring.
Within the framework of precision spine care, AI-enabled tele-ultrasound may offer a scalable solution for evaluating muscles and fascia, guiding interventional procedures, monitoring treatment response, and extending specialist expertise beyond traditional clinical settings. When ethically implemented and rigorously validated, tele-ultrasound augmented by AI has the potential to improve access, consistency, and quality of musculoskeletal imaging, supporting patient-centered care across diverse healthcare environments.
AI is increasingly transforming ultrasound-guided spine interventions by improving procedural precision, safety, and workflow efficiency, particularly in lumbar facet joint injections and perineural nerve blocks [28]. These procedures are inherently challenging due to the deep anatomical location of lumbar targets, complex osseous architecture, acoustic shadowing, and patient-related factors such as obesity and degenerative spinal disease, all of which contribute to significant operator dependency and technical variability [29]. AI-driven image analysis algorithms address these challenges by enabling real-time recognition and labeling of key lumbar sonoanatomical landmarks, including spinous processes, laminae, transverse processes, facet joints, and exiting nerve roots [28]. Automated anatomical identification reduces cognitive load, enhances spatial understanding, and shortens the learning curve, particularly for less experienced clinicians performing ultrasound-guided spinal procedures. By improving real-time anatomical clarity, AI facilitates optimal probe positioning and accurate planning of needle trajectories, which are critical determinants of success in intra-articular facet joint injections and selective nerve root or perineural blocks [23].
Beyond landmark identification, machine learning models integrated into ultrasound platforms can continuously track the needle tip, predict its trajectory, and provide real-time visual or auditory feedback during needle advancement. These systems enhance procedural safety by alerting operators when needle deviation places critical structures such as vascular elements, the dural sac, or adjacent neural tissue at risk [30]. Enhanced image processing may also improve visualization of poorly defined targets, including inflamed nerve roots or narrowed facet joint spaces frequently encountered in degenerative spine disease, further expanding the applicability of ultrasound-guided interventions [29].
AI also plays a growing role in pre-procedural planning and outcome prediction through the integration of clinical data with prior ultrasound, MRI, or computed tomography (CT) datasets. Such multimodal data integration supports patient selection, intervention planning, and personalized treatment strategies, reinforcing the principles of precision spine care [31].
Augmented reality (AR) represents an emerging adjunct to AI-enhanced ultrasound guidance, offering improved procedural accuracy, spatial orientation, and reduced cognitive burden. By overlaying virtual anatomical structures, ultrasound imaging planes, or planned needle trajectories directly into the operator’s field of view using head-mounted displays or smart glasses, AR bridges the gap between image interpretation and hand–eye coordination. Recent phantom-based and trainee-focused clinical studies have demonstrated reductions in cognitive load and shorter planning and needle-placement times compared with conventional ultrasound guidance [32, 33].
Mixed reality (MR), an extension of AR, further enables interactive manipulation and spatial anchoring of three-dimensional holographic anatomical models aligned with patient anatomy. Platforms integrating portable three-dimensional ultrasound tracking with MR headsets have demonstrated the feasibility of generating holographic reconstructions that support both procedural navigation and advanced training applications [32].
Fusion imaging represents another important AI-adjacent advancement by combining real-time ultrasound with pre-acquired CT or MRI datasets to improve anatomical localization in regions where sonographic landmarks are limited or deeply situated. This approach allows clinicians to leverage the superior soft-tissue contrast of MRI or the detailed osseous depiction of CT while preserving the real-time, radiation-free advantages of ultrasound [34]. AR-enhanced fusion techniques further reduce cognitive burden by projecting fused datasets directly into the operator’s field of view, although early phantom studies demonstrate feasibility rather than definitive accuracy advantages over conventional fusion systems [35].
Although AI-assisted image generators are still in their early stages of development, they are already sufficiently capable of helping to illustrate this novel topic clearly. Figure 1 illustrates the integration of AI, AR, fusion imaging, and tele-ultrasound in spine interventions. Tele-ultrasound allows remote expert guidance, supporting clinicians in resource-limited settings. Ethical and safety considerations are highlighted at the top, including informed consent, data security, and explainable AI. A patient receives a lumbar ultrasound while the clinician uses AI-assisted real-time anatomical landmark recognition, including spinous processes, facet joints, and nerve roots. AI-guided needle tracking provides continuous feedback on trajectory and proximity to critical structures, enhancing procedural safety. Clinical outcomes of AI-integrated ultrasound, depicted at the bottom, include pain relief, improved mobility, and personalized rehabilitation planning. This figure demonstrates the convergence of advanced imaging, AI, telemedicine, and ethical frameworks in precision spine care.
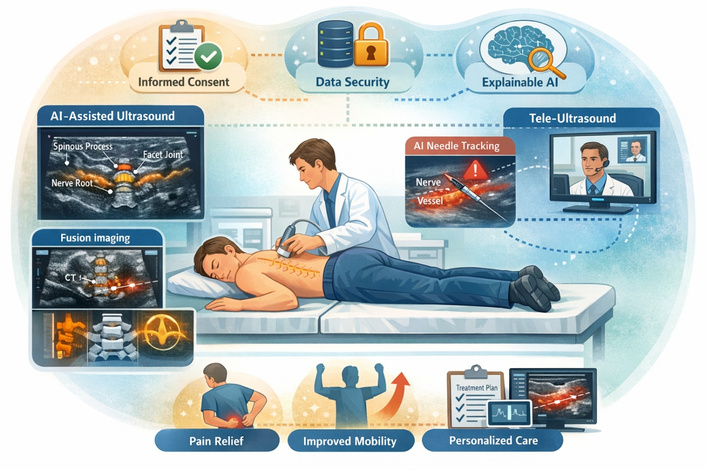
AI-enhanced spine ultrasound workflow for precision musculoskeletal care. The schematic illustrates the integration of artificial intelligence (AI), augmented reality (AR), fusion imaging, and tele-ultrasound in spine interventions.
Looking forward, emerging innovations suggest increasing convergence among AI, AR/MR, fusion imaging, and robotics. Robotic platforms integrating cone-beam CT with robotic ultrasound acquisition enable automated image co-registration and fusion without manual probe manipulation, offering a pathway toward greater procedural reproducibility and reduced operator strain [36]. When combined with immersive visualization overlays, such systems may allow clinicians to plan and execute complex spine interventions with enhanced anatomical awareness and reduced cognitive load. As hardware becomes more ergonomic and software integration more seamless, AI-augmented and AR-enabled ultrasound technologies are likely to evolve into routine adjuncts for advanced spine interventions, representing a significant advance in both interventional efficacy and clinician training. The conceptual workflow illustrated in Figure 2 is an integration of ultrasound, AI analysis, and telemedicine via a secure cloud platform. Fusion imaging combines real-time ultrasound with pre-acquired CT or MRI datasets to improve anatomical localization. This system enables remote consultation, real-time image interpretation, and collaborative clinical decision-making. In AR-assisted ultrasound-guided spine injection, the operator wears an AR headset that projects real-time ultrasound images, reconstructed anatomical targets, and planned needle trajectories directly into the visual field. Virtual overlays highlight the target region and guide needle advancement, enhancing hand–eye coordination, spatial orientation, and procedural accuracy. This immersive visualization reduces cognitive load by minimizing attention shifts between the patient and external monitors, supporting safer and more efficient interventions, AR-assisted ultrasound-guided spine injection, demonstrating holographic overlays of anatomical targets and projected needle trajectories within the operator’s field of view. AR-assisted ultrasound-guided spine injection uses holographic overlays of anatomical targets and projected needle trajectories within the operator’s field of view. This immersive visualization reduces cognitive load by minimizing attention shifts between the patient and external monitors, thereby supporting safer and more efficient interventions. This visualization further improves spatial orientation, hand–eye coordination, and procedural accuracy, fusion imaging combining real-time sonography with pre-acquired CT or MRI datasets, allowing enhanced visualization of vertebral anatomy and target structures. Comparison between standard ultrasound and fused imaging highlights improved anatomical localization and guidance for interventional planning.
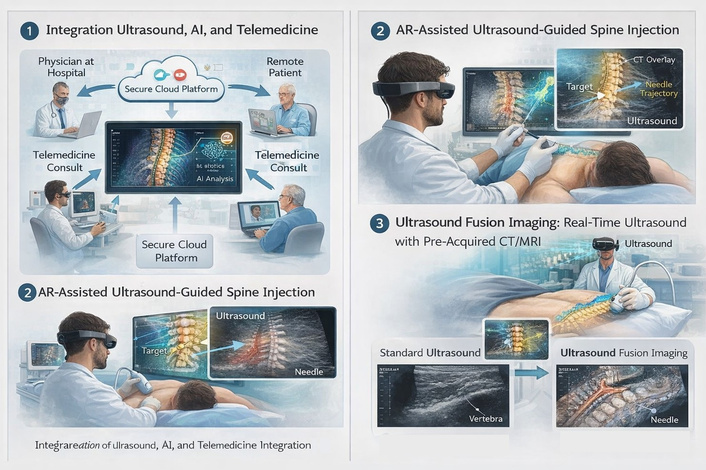
Integration of artificial intelligence (AI), augmented reality (AR), and fusion imaging in ultrasound-guided spine care. (1) Integration of ultrasound, AI analysis, and telemedicine. (2) AR-assisted ultrasound-guided spine injection. (3) Ultrasound fusion imaging combining real-time sonography with pre-acquired computed tomography (CT) or magnetic resonance imaging (MRI).
Compared with conventional in-person ultrasound, tele-ultrasound primarily improves access and workforce distribution but remains constrained by operator dependence, variable network performance, and heterogeneous evidence quality, with current studies supporting non-inferiority only in selected clinical contexts rather than across all musculoskeletal and spine applications [15, 16].
In contrast, AI-augmented ultrasound offers added value through automated landmark detection, needle tracking, and real-time decision support, which may reduce inter-operator variability and cognitive load; however, its clinical maturity is limited by moderate diagnostic performance in complex spinal pathology, restricted external validation, and a lack of large-scale prospective outcome studies [14, 28].
In limited-resource and point-of-care settings, ultrasound remains a valuable and accessible imaging modality for procedural guidance and clinical assessment [14]. In addition, AI-augmented ultrasound may provide added value through automated landmark detection, deep learning-based needle tracking, and real-time anatomical structure recognition, which could help reduce inter-operator variability and cognitive workload during musculoskeletal imaging and interventions [28, 29]. However, broader clinical implementation still requires stronger external validation and larger prospective outcome studies to establish reliability and generalizability across complex clinical applications.
Augmented and MR systems, as well as fusion imaging techniques, primarily enhance spatial orientation and multimodal anatomical correlation, respectively, but their supporting evidence remains largely derived from phantom models and early feasibility studies, limiting conclusions regarding superiority over standard ultrasound-guided practice and raising unresolved questions regarding cost-effectiveness, usability, and training requirements [32–35].
Robot-assisted and remotely operated ultrasound platforms further improve procedural precision and reproducibility by minimizing manual probe variability, yet their adoption is currently limited by infrastructure demands, system complexity, and latency-related constraints, which restrict scalability in routine clinical spine care [26, 36].
Overall, while tele-ultrasound addresses access barriers, AI improves interpretative and procedural intelligence, AR/MR enhances visualization, fusion imaging strengthens anatomical integration, and robotics increases mechanical accuracy, the evidence base for each remains predominantly feasibility-oriented, with limited head-to-head comparative trials or long-term outcome data.
The integration of AI into spine and musculoskeletal care introduces significant ethical considerations, particularly regarding patient autonomy, privacy, and clinical oversight. AI tools must be transparently disclosed during the informed consent process. Patients should understand the role of AI in decision-making, its limitations, and the degree of human supervision involved. Explainable AI (XAI) is essential in meeting the standards of informed consent, ensuring that patients can meaningfully comprehend how AI informs their care [37–39].
AI systems rely on access to large-scale patient datasets, raising concerns regarding de-identification, unauthorized access, and potential data breaches. Compliance with privacy regulations such as the Health Insurance Portability and Accountability Act (HIPAA) in the United States and the General Data Protection Regulation (GDPR) in the European Union is mandatory, and implementation of encrypted databases with restricted access protocols is recommended to safeguard patient information [40]. Additionally, AI-generated outputs must always be reviewed by qualified clinicians, as inaccurate, biased, or misleading recommendations could compromise patient safety [12, 41].
Specific challenges in AI-assisted ultrasound and interventional spine care include operator dependency, limited imaging visibility, and moderate accuracy in complex decision-making scenarios. Addressing these challenges requires combining imaging modalities where necessary, applying explainable AI with visual aids to improve patient understanding, and maintaining clinician oversight throughout diagnosis and intervention [12, 42].
Addressing these challenges requires combining complementary imaging approaches with clinician oversight to improve diagnostic interpretation and medical decision-making. Ultrasound-based imaging has demonstrated value in enhancing anatomical visualization and interpretation skills in medical training environments [42], while the integration of AI into healthcare can support more accurate and efficient clinical assessment when applied alongside human expertise and supervision [12].
Telemedicine and tele-ultrasound introduce additional ethical considerations related to privacy, data security, and equitable access. Remote delivery of care must adhere strictly to applicable regulations while ensuring high-quality imaging and interpretation, even in resource-limited or rural settings [43–46].
The responsible integration of AI also requires structured guidance in clinical education. Ultrasound-based training enhances anatomical understanding, palpation skills, and spatial reasoning, yet machine- and AI-assisted platforms can impose additional cognitive load on learners. Structured curricula, repeated practice, and supervision are critical to ensure competence without overwhelming trainees. Adoption of standardized frameworks for AI evaluation, including Consolidated Standards of Reporting Trials-Artificial Intelligence (CONSORT-AI) and Developmental and Exploratory Clinical Investigations of Decision Support Systems Driven by Artificial Intelligence (DECIDE-AI), remains limited but is necessary to promote consistent and safe implementation in clinical practice [47, 48].
Adoption of standardized educational and methodological approaches remains important for the effective integration of ultrasound technologies into healthcare training and practice. Recent studies have emphasized the role of structured ultrasound-based educational strategies in improving learner performance, anatomical understanding, and musculoskeletal palpation skills among medical trainees [47, 48].
Overall, precision spine care using AI and ultrasound offers remarkable opportunities for personalized diagnostics, real-time monitoring, and procedural guidance. However, these benefits must be balanced with ethical vigilance. Ensuring informed consent, maintaining patient confidentiality, applying explainable AI, and enforcing rigorous clinician oversight are all essential to delivering safe, transparent, and patient-centered care. AI should complement, rather than replace, professional judgment, fostering responsible integration of emerging technologies into musculoskeletal medicine.
AI-driven spine ultrasound is transforming musculoskeletal care by enhancing diagnostic precision, enabling objective tissue assessment, and supporting personalized rehabilitation strategies. When combined with tele-ultrasound, these technologies expand access to expert musculoskeletal evaluation and intervention, particularly in remote or resource-limited settings. AI-augmented procedural guidance, including real-time landmark recognition, needle tracking, and fusion imaging, improves the safety, accuracy, and efficiency of spine interventions.
Responsible implementation requires adherence to ethical principles, including transparent informed consent, explainable AI, secure data handling, and continuous clinician oversight. While technological advances offer powerful educational and clinical benefits, operator skill, structured training, and thoughtful integration remain essential to maximize outcomes. Ultimately, AI, ultrasound, and telemedicine serve to augment, not replace clinicians, enabling precision spine care that is safe, effective, and patient-centered.
AI: artificial intelligence
AR: augmented reality
CT: computed tomography
MR: mixed reality
MRI: magnetic resonance imaging
The authors confirm that all figures were created by the authors. AI-assisted tools were used during the drafting and visualization refinement process; however, all final figures were author-generated and manually edited. The authors confirm compliance with journal policies regarding the use of AI-assisted technologies in scientific writing. All copyright and ethical requirements have been fully addressed.
HG: Conceptualization, Resources, Software, Formal analysis, Supervision, Investigation, Methodology, Writing—original draft, Project administration, Writing—review & editing. PG: Conceptualization, Data curation, Formal analysis, Validation, Methodology, Writing—original draft. ZB: Writing—original draft, Project administration. SM: Resources, Software, Investigation, Visualization, Writing—original draft. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
The authors received no financial support for the research, authorship, and/or publication of this article.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 624
Download: 25
Times Cited: 0
