 Review
Review

Affiliation:
1Integrative Metabolic Fluxomics Lab, Lee Gil Ya Cancer and Diabetes Institute, Gachon University, Incheon 21999, Republic of Korea
ORCID: https://orcid.org/0000-0002-9127-9494
Affiliation:
2Department of Sports Medicine and Science, Graduate School, Konkuk University, Seoul 05029, Republic of Korea
3Physical Activity and Performance Institute, Konkuk University, Seoul 05029, Republic of Korea
Email: parkhy1980@konkuk.ac.kr
ORCID: https://orcid.org/0000-0002-9901-7624
Explor Med. 2026;7:1001409 DOI: https://doi.org/10.37349/emed.2026.1001409
Received: January 27, 2026 Accepted: April 24, 2026 Published: June 03, 2026
Academic Editor: Lindsay A. Farrer, Boston University School of Medicine, USA
Obesity during the menopausal transition accelerates vascular aging through systemic inflammation, insulin resistance, and estrogen loss. These pathological processes impair endothelial function and arterial compliance, thereby increasing cardiovascular risk while simultaneously disrupting cerebral circulation, neurovascular regulation, and neuroendocrine stability that contribute to cognitive decline and psychological vulnerability. Regular exercise has emerged as an important non-pharmacological strategy to counteract these multidimensional impairments. Particular attention has been given to the modifying role of hormonal status and the differential adaptations observed between premenopausal and postmenopausal states. Evidence indicates that aerobic and multimodal programs enhance nitric oxide bioavailability, vascular elasticity, and cerebral perfusion, whereas resistance training contributes to musculoskeletal strength, metabolic regulation, and psychological resilience. Novel approaches such as interval-based or hypoxic exercise may provide additional benefits for postmenopausal women but require individualized supervision. Importantly, exercise-induced vascular improvements extend beyond cardiovascular protection, restoring cerebral blood flow, promoting hippocampal plasticity, and stabilizing hypothalamic–pituitary–adrenal axis function. These adaptations mediate enhancements in memory, executive performance, mood regulation, and stress resilience. This review synthesizes current findings across aerobic training, resistance training, combined training, high-intensity interval training, and hypoxic conditioning, and proposes an integrative vascular–cognitive–mental health framework that unifies these domains into a coherent model, with vascular function as a central mechanistic pathway linking exercise to cognitive and psychological outcomes, while underscoring the need for precision exercise prescriptions tailored to hormonal status, vascular risk, and functional capacity in obese women.
Obesity has become a critical global health concern, particularly among women, with prevalence continuing to rise in both developed and developing countries. More than 40% of adult women are categorized as overweight or obese, a condition that strongly contributes to cardiovascular disease, metabolic dysfunction, and diminished quality of life [1]. The menopausal transition represents a vulnerable stage in which estrogen deficiency, accumulation of visceral adiposity, and systemic inflammation converge, accelerating vascular aging and heightening cardiometabolic risk [2, 3]. Endothelial dysfunction, arterial stiffness, and chronic low-grade inflammation emerge as principal mechanisms through which obesity and menopause jointly increase the burden of cardiovascular disease [3–5].
The consequences of vascular impairment extend beyond the cardiovascular system. Reduced cerebral blood flow, microvascular dysfunction, and heightened systemic inflammation increase the likelihood of cognitive decline and dementia in obese postmenopausal women [6–8].
Mental health is another domain adversely influenced by both obesity and menopausal status. Midlife women frequently report elevated rates of depression, anxiety, and lower quality of life, and these outcomes are further exacerbated by vascular dysfunction and cognitive deterioration [9]. These findings highlight the interdependence of vascular, cognitive, and psychological health, suggesting that vascular dysfunction may act as a central mechanism linking impaired cerebral perfusion, neurovascular dysregulation, and adverse psychological outcomes in obese postmenopausal women, while underscoring the role of exercise as an effective non-pharmacological strategy to improve outcomes across these domains.
Despite these advances, the majority of prior reviews have addressed vascular outcomes or cognitive and mental health outcomes separately, often in mixed-gender populations. As a result, sex-specific adaptations have been insufficiently characterized. Few efforts have systematically integrated evidence across vascular, cognitive, and psychological domains in obese women undergoing menopause. Moreover, the extent to which hormonal status modulates exercise-induced responses remains underexplored. The purpose of this narrative review is therefore to synthesize current findings on the effects of exercise on vascular health, cognition, and mental health in obese women across the menopausal transition. By merging mechanistic insights with clinical evidence, the review seeks to clarify hormone-dependent adaptations and provide a foundation for precision exercise prescriptions that reduce cardiovascular burden, preserve cognitive function, and enhance psychological well-being in this high-risk group. To enhance transparency, this mini review adopts a structured narrative approach. Relevant literature was identified through searches of PubMed, Scopus, and Web of Science using combinations of keywords related to menopause, obesity, vascular function, cognitive function, mental health, and exercise modalities. Studies were selected based on relevance to the target population and outcomes of interest, with priority given to randomized controlled trials and meta-analyses where available. Additional mechanistic and observational studies were included when necessary to support physiological interpretation. Given the narrative nature of this review, a qualitative synthesis approach was applied rather than a formal systematic analysis.
Obesity in postmenopausal women is commonly defined using body mass index (BMI), with thresholds of ≥ 30 kg/m2 or ≥ 25 kg/m2 in Asian populations [1]. However, BMI does not reflect fat distribution, which is a critical determinant of cardiometabolic risk during menopause.
Central adiposity increases markedly following estrogen decline and is strongly associated with vascular dysfunction and metabolic impairment [3]. Therefore, additional anthropometric indices such as waist circumference and waist-to-hip ratio should be considered. Waist circumference (≥ 88 cm in women) and waist-to-hip ratio (> 0.85) are established indicators of abdominal obesity and cardiovascular risk [1].
Variability in obesity definitions across studies may contribute to inconsistent findings. Accordingly, the combined use of BMI and central adiposity markers provides a more comprehensive framework for evaluating obesity-related risk in postmenopausal women. Key anthropometric indices used to define general and central obesity in postmenopausal women are summarized in Table 1.
Anthropometric indices for defining general and central obesity in postmenopausal women.
| Index | Definition | Cut-off (women) | Clinical relevance |
|---|---|---|---|
| Body mass index (BMI) | Weight (kg)/height (m)2 | ≥ 30 kg/m2 (≥ 25 kg/m2 in Asian populations) | General obesity classification |
| Waist circumference(WC) | Abdominal girth | ≥ 88 cm | Indicator of central obesity and cardiometabolic risk |
| Waist-to-hip ratio(WHR) | WC/hip circumference | > 0.85 | Reflects fat distribution and cardiovascular risk |
Vascular dysfunction constitutes a central mechanism linking obesity, menopausal transition, and heightened cardiometabolic vulnerability in women. Endothelial impairment, increased arterial stiffness, and chronic inflammation accelerate cardiovascular disease progression while simultaneously predisposing to cognitive decline and psychological disturbances. The loss of estrogen following menopause amplifies these adverse processes, producing a distinct phenotype of accelerated vascular aging [2, 10]. Clarifying the biological drivers of this dysfunction is essential for identifying therapeutic strategies and understanding how exercise delivers multidimensional health benefits. This section outlines the key mechanisms, including endothelial dysfunction, arterial stiffening, inflammation, oxidative stress, and hormonal influences.
The combined effects of obesity and menopause hasten vascular aging through multiple interacting pathways. Endothelial dysfunction, marked by reduced nitric oxide (NO) availability and impaired vasodilation, is a defining feature [4, 10, 11]. During the menopausal transition, estrogen withdrawal removes an important protective signal, as estrogen receptor–mediated activation of endothelial NO synthase (eNOS) normally sustains NO production and limits oxidative stress [10, 11]. Loss of this regulatory pathway weakens endothelial repair capacity and heightens vulnerability to vascular injury. Clinical and mechanistic evidence indicate that postmenopausal status, particularly in the presence of obesity, is associated with impaired flow-mediated dilation (FMD) and elevated pulse wave velocity (PWV), reflecting compounded vascular risk [2, 3]. While obesity and menopause independently contribute to vascular dysfunction through distinct mechanisms, their coexistence may exert additive and potentially synergistic effects. Obesity primarily promotes chronic inflammation and oxidative stress, whereas menopause-related estrogen deficiency impairs endothelial repair and NO signaling. When combined, these processes may amplify endothelial dysfunction and arterial stiffness beyond the effects of either condition alone.
Obesity also intensifies oxidative stress, partly through the accumulation of asymmetric dimethylarginine (ADMA), an endogenous eNOS inhibitor, which further disrupts vasodilatory signaling [12]. Adipose tissue contributes to additional vascular injury by releasing adipokines and pro-inflammatory cytokines, including tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), which suppress eNOS activity, induce endothelial apoptosis, and sustain chronic inflammation [4, 13]. Together, these mechanisms create a pro-constrictive vascular environment with impaired endothelial responsiveness.
Arterial stiffness is another hallmark of vascular aging in obese postmenopausal women. Mechanisms include advanced glycation end-product (AGE) deposition, sympathetic overactivation, and structural remodeling of the vascular wall through collagen accumulation and elastin degradation [14, 15]. These alterations reduce arterial compliance, elevate systolic blood pressure (SBP), and worsen cardiovascular burden. Collectively, obesity-related inflammation and oxidative stress, combined with estrogen deficiency, impose a synergistic strain on the vasculature, markedly increasing cardiovascular risk in postmenopausal women.
The progression of vascular aging is closely tied to cognitive decline in women. Reduced cerebral perfusion, impaired microvascular integrity, and increased arterial stiffness limit the delivery of oxygen and nutrients to the brain, thereby promoting neurodegenerative processes [16, 17]. Obese postmenopausal women are particularly susceptible to dementia and Alzheimer’s disease due to the convergence of vascular dysfunction, systemic inflammation, and hormonal loss [6]. Small vessel disease, associated with stiffened arteries, contributes to deficits in executive function and memory, while white matter hyperintensities and microinfarcts further exacerbate declines in processing speed and working memory [18, 19].
Estrogen deficiency worsens these processes by weakening neurovascular coupling and reducing NO-mediated support for cerebral blood flow [2, 17, 20], changes that may indirectly contribute to impaired hippocampal neurogenesis and synaptic plasticity. These observations suggest that vascular dysfunction is not merely a comorbid feature but a primary determinant of cognitive aging during the menopausal transition. Improving vascular health may enhance cerebral perfusion and support cognitive function, with exercise interventions demonstrating improvements in memory and executive performance [7, 21, 22].
Vascular pathology also contributes to psychological disturbances. Endothelial dysfunction, dysregulated hypothalamic–pituitary–adrenal (HPA) axis activity, and systemic inflammation act together to increase the risk of depression and anxiety [23]. Cerebral hypoperfusion and impaired NO signaling have been linked to mood disorders, while pro-inflammatory cytokines amplify vulnerability to depression through neurotransmitter imbalance [24]. Specifically, mediators such as IL-6 and TNF-α disrupt serotonin and dopamine pathways, alter synaptic plasticity, and activate microglia, thereby connecting peripheral vascular pathology with central mood regulation [23, 24].
Estrogen deficiency during menopause may further exacerbate these pathways by reducing serotonergic and dopaminergic stability and impairing neurovascular support for limbic regions involved in mood regulation [9, 25, 26]. Epidemiological studies indicate a strong association between depression and cardiovascular disease in women, suggesting that vascular impairment may contribute to heightened psychological vulnerability [27, 28]. These findings underscore vascular dysfunction as a biological substrate linking obesity and menopause to mental health decline.
Given the multifactorial nature of vascular dysfunction in obese postmenopausal women, exercise is recognized as one of the most effective non-pharmacological approaches to counteract these impairments. Physical activity improves endothelial function, lowers arterial stiffness, and reduces systemic inflammation, thereby addressing the biological mechanisms that accelerate vascular aging [29–31]. Beyond vascular restoration, exercise enhances cerebral perfusion, stimulates neural plasticity, and stabilizes neuroendocrine function, which collectively support cognitive performance and psychological resilience [7, 21, 22]. These multidimensional benefits underscore the role of exercise as a unifying therapy capable of simultaneously protecting cardiovascular, cognitive, and mental health.
The following sections describe the mechanistic basis of exercise-induced vascular protection, outline the distinct adaptations produced by different training modalities, and integrate these effects into the broader vascular–cognitive–mental health framework relevant to obese women across the menopausal transition.
The menopausal transition is characterized by estrogen deficiency, which disrupts vascular homeostasis and accelerates endothelial dysfunction. Reduced eNOS activity and diminished NO availability impair vasodilation and vascular repair capacity [2, 20]. This deficiency is compounded by obesity-driven inflammation and oxidative stress, heightening arterial stiffness and cardiovascular risk [32, 33].
Exercise partly compensates for the loss of estrogen through several mechanisms. These effects can be conceptually organized into a hierarchical signaling cascade. Hemodynamic stimuli such as exercise-induced shear stress act as primary upstream drivers, initiating eNOS activation and NO production, as well as mitochondrial adaptations that enhance cellular energy efficiency. These upstream events subsequently modulate downstream pathways, including reductions in oxidative stress and inflammatory cytokines, which collectively improve endothelial function and vascular repair capacity. At a higher level of integration, these vascular adaptations support cerebral perfusion, neuroplasticity, and neuroendocrine regulation, ultimately contributing to improvements in cognitive function and mental health. Consistent with this framework, aerobic and interval exercise generate repeated shear stress that stimulates eNOS activity and restores NO-mediated vasodilation, thereby improving endothelial responsiveness [34]. Observational evidence also shows impaired endothelial function across menopausal stages, underscoring the relevance of targeting vascular health in this population [35]. Regular training also strengthens antioxidant defense systems such as superoxide dismutase and glutathione peroxidase, counteracting the oxidative stress burden common in postmenopausal women [32, 36]. In parallel, exercise downregulates pro-inflammatory cytokines, including IL-6 and TNF-α, helping reduce the chronic inflammatory state characteristic of this population [37, 38]. At the cellular level, physical activity improves mitochondrial efficiency, mobilizes endothelial progenitor cells, and activates hypoxia-inducible factor-1α (HIF-1α) signaling, which collectively promotes vascular repair and angiogenesis [39–42].
These adaptations extend into neurocognitive and psychological domains. Enhanced NO signaling and improved endothelial function sustain cerebral perfusion, supporting hippocampal neurogenesis and synaptic plasticity that are essential for memory and executive function [21, 22]. Anti-inflammatory and antioxidant effects further stabilize HPA axis regulation and balance neurotransmitter systems, providing a mechanistic explanation for improved mood and resilience [23, 24]. In this way, exercise exerts multifaceted benefits that restore vascular health, preserve cognitive capacity, and alleviate psychological symptoms in estrogen-deficient women.
Estrogen deficiency accelerates endothelial dysfunction, arterial stiffening, and systemic inflammation, all of which compromise cardiovascular, cognitive, and mental health [2, 33]. Exercise reverses these impairments by improving NO bioavailability, reducing oxidative stress, and modulating inflammatory pathways [34]. The resulting vascular benefits act as mediators of enhanced brain perfusion, synaptic function, and psychological resilience. Distinct exercise modalities provide unique but complementary benefits, and their vascular effects frequently translate into measurable improvements in cognition and mental health. However, these benefits are not uniformly observed across all exercise modalities or populations. Some interventions show variable vascular responses, and several cognitive and mental health findings are derived from non-obese or mixed populations, which warrants cautious interpretation when applying this evidence to obese postmenopausal women.
Aerobic training (AT) is the most extensively studied modality for vascular rehabilitation in postmenopausal women. Regular moderate-intensity training, typically performed at 50–70% of maximal oxygen uptake (VO2max) or 60–75% of maximum heart rate, three to five times per week for at least 8–12 weeks, significantly improves FMD and reduces PWV [43], alongside reductions in inflammatory markers such as C-reactive protein (CRP) and IL-6. Observational data also show impaired endothelial function across menopausal stages, emphasizing the need for exercise-based vascular rehabilitation [35]. Improved vascular function supports cerebral perfusion and hippocampal neurogenesis, thereby enhancing memory consolidation and executive performance [21]. Clinical trials confirm that aerobic interventions improve global cognition and executive function in older women, even without estrogen synergy [7].
Beyond cognition, AT reduces depressive symptoms and enhances quality of life. Walking, cycling, and rhythmic activities not only improve vascular markers but also stabilize HPA axis function, regulate serotonergic pathways, and upregulate brain-derived neurotrophic factor (BDNF), contributing to better mood and reduced anxiety [44–46]. In addition, aerobic interventions have been associated with improved sleep quality and autonomic nervous system balance, factors that play an important role in stress resilience and emotional stability in postmenopausal women. These psychological adaptations appear to be reinforced when AT is performed in group or community-based settings, where social interaction further enhances well-being and adherence to long-term exercise participation. Weight-bearing and non-weight-bearing options (e.g., aquatic exercise) are both effective, with the latter providing safer alternatives for women with joint discomfort or obesity-related mobility limitations [47]. AT, therefore, represents an accessible and versatile intervention that simultaneously addresses vascular, cognitive, and psychological challenges in postmenopausal women [7, 48]. These multidomain effects support the view that improvements in endothelial function and cerebral perfusion may contribute not only to cognitive benefits but also to enhanced psychological resilience in this population.
Resistance training (RT), traditionally prescribed for musculoskeletal health, has growing relevance for vascular outcomes. Moderate-intensity RT (50–70% of one-repetition maximum [1RM], 2–3 times per week for 8–12 weeks) produces mixed effects on central arterial stiffness and vascular compliance. Some trials show no change [49], whereas meta-analyses indicate that low-to-moderate intensity RT may improve arterial elasticity, while high-intensity RT can yield no benefit or adverse effects [50]. These vascular adaptations are closely linked to systemic hemodynamic regulation and influence cerebral blood flow, which is essential for maintaining neuronal metabolism and function. These adaptations facilitate more efficient cerebral circulation, indirectly supporting cognitive performance. Mechanistic studies suggest that RT enhances skeletal muscle perfusion, reduces sympathetic vasoconstrictor tone, and promotes angiogenesis through upregulation of vascular endothelial growth factor (VEGF), thereby contributing to systemic vascular improvements [51–53]. However, most of these findings are derived from studies in mixed adult populations rather than exclusively postmenopausal women, and the evidence specific to obese women in this group remains limited. This limitation is clinically important because estrogen deficiency, central adiposity, and chronic low-grade inflammation may fundamentally alter vascular responsiveness and neurovascular coupling, thereby limiting the direct applicability of findings derived from mixed populations. As a result, the magnitude and even the direction of RT-induced adaptations may differ in obese postmenopausal women, leading to potential misinterpretation when extrapolating existing evidence. Nonetheless, improvements in muscular strength, functional capacity, and psychosocial resilience provide a rationale for potential cognitive and psychological benefits, suggesting that well-designed RT programs may still offer clinically meaningful outcomes for postmenopausal women.
Psychological benefits of RT are increasingly recognized. Improvements in muscle strength and functional capacity enhance self-efficacy, resilience, and independence, which are critical for reducing depressive symptoms in midlife and postmenopausal women [54]. Beyond these psychosocial mechanisms, emerging evidence indicates that RT may influence neurobiological pathways relevant to mental health. In particular, RT may influence neurobiological pathways relevant to mental health, including factors such as insulin-like growth factor-1 (IGF-1), which has been implicated in hippocampal plasticity, serotonergic regulation, and mood stabilization [21, 22]. These neurobiological changes are associated with functional adaptations in brain regions involved in emotion regulation, including the hippocampus and prefrontal cortex. These adaptations provide a mechanistic rationale for observed reductions in depressive symptoms and anxiety among postmenopausal women engaging in regular RT. Moreover, enhanced muscular strength reduces fear of falling and physical frailty, which indirectly supports psychological well-being by improving confidence in daily functioning. However, acute high-intensity RT (> 80% 1RM) can transiently stiffen arteries if not carefully periodized [55]. Well-designed RT programs that emphasize progressive overload, multi-joint exercises, and adequate recovery, therefore, represent safe and effective strategies to reinforce vascular, cognitive, and psychological health while simultaneously improving mobility, independence, and long-term quality of life in obese women. Although direct evidence for cognitive outcomes remains limited in obese postmenopausal women, these findings suggest that RT-induced improvements in muscle perfusion, metabolic regulation, and neurobiological signaling may contribute to broader vascular and psychological adaptations across domains. Future studies should move beyond generalized RT paradigms and specifically examine obese postmenopausal women using integrated, multi-domain outcomes, including endothelial function, cerebral perfusion, neurotrophic signaling, and clinically relevant cognitive and mental health measures, to determine whether RT elicits distinct or attenuated adaptations in this high-risk population.
Combined training (CT), integrating aerobic and resistance modalities, provides complementary stimuli that yield superior outcomes compared with single-modality programs. Meta-analyses in postmenopausal women indicate that CT induces the greatest improvements in FMD and PWV, along with reductions in SBP and inflammatory markers such as CRP and IL-6 [56]. A recent randomized controlled trial further demonstrated that a 12-week multicomponent program significantly improved executive function in postmenopausal women [57], underscoring the cognitive benefits of CT. Broader meta-analytic evidence also confirms that combined aerobic and RT enhances global cognition in adults over 50 years, including memory and processing speed [7]. In addition, clinical studies in midlife women report that CT interventions improve quality of life and psychological well-being, with reductions in depressive symptoms and anxiety [48, 54, 58].
Mechanistically, CT unites the hemodynamic advantages of aerobic activity with the angiogenic and metabolic effects of RT. Together, these adaptations improve vascular elasticity, cerebral perfusion, and inflammatory balance, thereby facilitating hippocampal plasticity and stabilizing HPA axis function [21, 22, 37]. Evidence also indicates that the sequence of exercise may be important, as aerobic exercise performed before RT produces greater improvements in arterial compliance and endothelial function than the reverse order [59]. From a practical perspective, CT programs typically include aerobic sessions at 50–70% VO2max or 60–75% maximal heart rate (HRmax), combined with RT at 60–70% of 1RM for multi-joint exercises performed 2–3 days per week [56, 59]. Sequencing aerobic exercise before RT may optimize endothelial responses and maximize vascular benefits [59].
CT may be particularly advantageous for postmenopausal women, who face overlapping metabolic, vascular, and psychosocial challenges. By simultaneously addressing endothelial dysfunction, muscular strength, and metabolic health, CT provides a holistic and sustainable intervention that not only reduces cardiovascular risk but also enhances cognitive performance, emotional well-being, and long-term adherence to physical activity. This pattern reinforces the proposed vascular–cognitive–mental health framework by showing how concurrent vascular and musculoskeletal adaptations may translate into integrated functional and psychological benefits.
High-intensity interval training (HIIT) is a time-efficient method that induces strong vascular adaptations. Alternating bouts of vigorous effort (85–95% HRmax for 30–90 s) and active recovery generate oscillatory shear stress, powerfully stimulating eNOS activity and NO production [60]. In obese hypertensive postmenopausal women, 8–12 weeks of HIIT, typically consisting of intervals performed at 85–95% of maximum heart rate for 30–90 s interspersed with active recovery at 50–60% HRmax, reduced PWV and systemic inflammation more effectively than moderate-intensity continuous training [61]. These vascular adaptations restore cerebral perfusion and neurovascular coupling, enhancing executive performance and processing speed.
Beyond vascular effects, HIIT also exerts measurable benefits on cognitive and mental health. Acute bouts of HIIT have been shown to improve executive function more robustly than moderate-intensity continuous exercise [62], and meta-analytic evidence indicates that exercise interventions including HIIT enhance global cognition in older adults [7]. In obese hypertensive postmenopausal women, a randomized controlled trial demonstrated that 8–12 weeks of HIIT significantly improved arterial stiffness and reduced systemic inflammation, underscoring its relevance for this population [61]. Additional studies in other groups, including younger adults and women with polycystic ovary syndrome, reported improvements in quality of life, psychological well-being, and reductions in depression, anxiety, and stress [63, 64]. These findings suggest that HIIT may improve vascular and functional outcomes and may also confer cognitive and psychological benefits. However, some of these effects are supported by evidence from populations other than obese postmenopausal women and should therefore be interpreted with caution.
While the efficiency of HIIT makes it attractive for postmenopausal women with limited time, its high cardiovascular demands necessitate careful progression and supervision, especially in those with obesity-related comorbidities. When appropriately prescribed, HIIT may offer a useful strategy to improve vascular function and may also support cognitive performance and psychological well-being in obese postmenopausal women. These convergent effects suggest that exercise-induced vascular adaptations may contribute to changes in neurocognitive and psychological outcomes, although population-specific evidence remains limited.
Hypoxic training introduces exercise under reduced oxygen conditions, stimulating angiogenesis and vascular remodeling. Hypoxia stabilizes HIF-1α, enhances VEGF expression, and increases eNOS activity, amplifying vascular adaptations [65]. In postmenopausal women, interventions such as combined aerobic and RT under normobaric or hypobaric hypoxia have been shown to improve FMD, PWV, and hemorheological function to a greater extent than normoxic exercise [66, 67].
Beyond vascular outcomes, some randomized controlled trials in non-obese and non-postmenopausal populations, including geriatric patients and adults recovering from COVID-19, have reported cognitive, functional, and psychological benefits of hypoxic conditioning or intermittent hypoxia-based training [68–70]. However, direct evidence for these outcomes in obese postmenopausal women remains limited.
Mechanistic investigations support these findings. Exercise performed in moderate normobaric hypoxia increased circulating BDNF to levels comparable with normoxia and did not impair executive function [71]. Controlled hypoxic exposures also prevented inactivity-induced reductions in BDNF, highlighting potential for preserving neuroplasticity-related signaling during sedentary periods [72]. A recent synthesis emphasized that carefully dosed hypoxia engages HIF-dependent pathways, moderates inflammation, and interacts with monoaminergic systems, offering a rationale for mitigating depressive and anxiety symptoms in vulnerable populations [73].
Nevertheless, safety considerations remain important. Systematic reviews confirm that acute severe hypoxia can transiently impair reaction time and accuracy [74, 75]. For obese postmenopausal women, practical programs typically involve treadmill walking, cycling, or aquatic exercise at simulated altitudes of 2,000–3,000 m, 30–60 min per session, two to three times weekly [66, 67]. Such regimens deliver vascular, cognitive, and mental health benefits at lower absolute workloads, provided sessions are supervised, oxygen saturation is monitored, and exercise intensity and hypoxic dose are individualized based on baseline fitness, comorbidities, and tolerance. At the same time, the available evidence remains less population-specific than for aerobic or CT, and the proposed links between vascular, cognitive, and psychological responses should therefore be interpreted cautiously in obese postmenopausal women. Accordingly, hypoxic exercise should be implemented with caution, requiring individualized prescription and close supervision to ensure safety, particularly in clinical populations.
A summary of the effects of different exercise modalities on vascular, cognitive, and mental health outcomes in obese postmenopausal women is presented in Table 2.
Exercise modalities and their effects on vascular, cognitive, and mental health in obese postmenopausal women.
| Exercise type | Protocol | Vascular outcomes | Cognitive outcomes | Mental health outcomes | Key references | Limitations/Evidence gaps |
|---|---|---|---|---|---|---|
| Aerobic training (AT) | 50–70% VO2max, 3–5 sessions/week, 8–12 weeks | ↑FMD, ↓PWV, ↓CRP, ↓IL-6 | ↑Executive function,↑Memory | ↓Depressive symptoms,↑QoL | [7, 43, 47] | Stronger evidence base than other modalities, but obesity-specific and menopause-specific studies remain limited. |
| Resistance training (RT) | 50–70% 1RM, 2–3 sessions/week, 8–12 weeks | Mixed effects on arterial stiffness, ↑Skeletal muscle perfusion | Potential cognitive support | ↑Self-efficacy,↓Depressive symptoms | [50, 51, 54, 55] | Direct evidence for cognitive outcomes in obese postmenopausal women remains limited. |
| Combined training (CT) | AT + RT, 2–3 sessions/week, 12 weeks | Greatest ↑FMD,↓PWV,↓SBP,↓Inflammation | ↑Executive function,↑Processing speed | ↑Emotional well-being, ↓Anxiety/Depression | [56, 57, 59] | Comparative evidence against other modalities remains limited despite favorable multidomain findings. |
| High-intensity interval training (HIIT) | 85–95% HRmax intervals (30–90 s) + recovery, 8–12 weeks | ↑Endothelial function,↓PWV,↓Inflammation | ↑Executive function,↑Processing speed | ↓Depression/anxiety,↑Psychological well-being | [60–64] | Evidence in obese postmenopausal women is still limited, particularly for cognitive and psychological outcomes. |
| Hypoxic training | AT or CT under normobaric/ hypobaric hypoxia, 2–3 sessions/week | ↑FMD, ↓PWV,↑VEGF,↑Angiogenesis | Potential cognitive support | Potential psychological benefits | [65–67, 69–71, 73–75] | Evidence is derived partly from non-target populations, and population-specific evidence remains limited. |
CRP: C-reactive protein; FMD: flow-mediated dilation; PWV: pulse wave velocity; SBP: systolic blood pressure; QoL: quality of life; VEGF: vascular endothelial growth factor; 1RM: one-repetition maximum; ↑ indicates an increase or improvement; ↓ indicates a decrease or reduction.
Integrative perspective: the vascular–cognitive–mental health framework
The evidence synthesized across exercise modalities underscores a unifying framework in which vascular adaptations mediate the broader cognitive and psychological benefits of physical activity in obese postmenopausal women. The multidimensional benefits of exercise across vascular, cognitive, and psychological domains can be conceptualized through an integrative framework. This relationship is illustrated in Figure 1, which depicts the vascular–cognitive–mental health framework in obese postmenopausal women. Endothelial dysfunction, arterial stiffness, and systemic inflammation constitute the biological substrate linking obesity and estrogen deficiency to impaired brain perfusion, hippocampal neurogenesis, and HPA axis dysregulation [2, 46, 76]. By restoring NO bioavailability, enhancing antioxidant defenses, and reducing inflammatory signaling, exercise-induced vascular improvements provide the mechanistic foundation for neurocognitive resilience and mental health stabilization [32, 34, 36, 37].
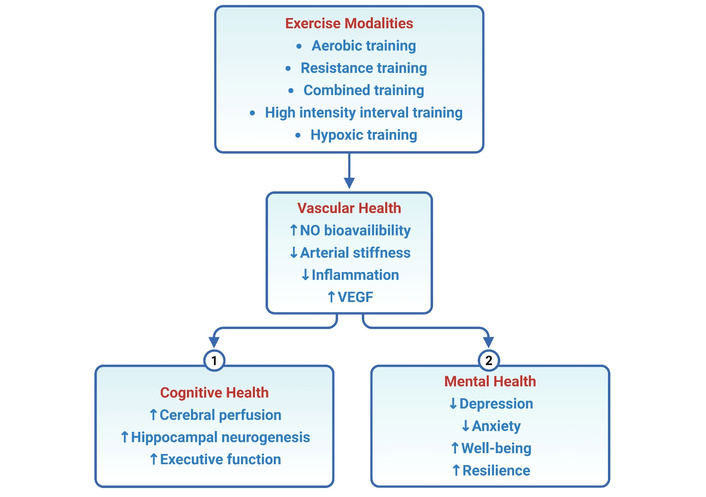
Conceptual model of the vascular–cognitive–mental health framework in obese postmenopausal women. Exercise modalities, including aerobic training (AT), resistance training (RT), combined training (CT), high-intensity interval training (HIIT), and hypoxic training, improve vascular health through enhanced nitric oxide (NO) bioavailability, reduced arterial stiffness, decreased inflammation, and increased angiogenesis via vascular endothelial growth factor (VEGF). These vascular adaptations mediate improved cerebral perfusion, hippocampal neurogenesis, and executive function, supporting cognitive health, while also reducing depression and anxiety and enhancing well-being and resilience to support mental health. In the figure, ↑ indicates an increase or enhancement, and ↓ indicates a decrease or reduction.
Within this framework, different exercise modalities act through complementary vascular pathways that converge on cognitive and psychological outcomes. AT augments endothelial function and cerebral perfusion, thereby supporting hippocampal plasticity and executive performance [21, 22]. Observational data further show impaired endothelial function across menopausal stages, underscoring the clinical relevance of these adaptations [35]. RT may enhance vascular compliance, particularly when performed at low to moderate intensity, and consistently increases skeletal muscle perfusion through angiogenic signaling [50–53]. CT leverages both hemodynamic and musculoskeletal adaptations, producing superior improvements in vascular elasticity, systemic inflammation, and cognitive processing [56, 57, 59]. HIIT maximizes oscillatory shear stress, contributing to improvements in eNOS activity and neurovascular coupling [60, 61], with additional trials showing benefits for depressive symptoms and psychological health [63, 64]. Hypoxic training further engages angiogenic signaling via VEGF and promotes autonomic balance, which together reinforce resilience in estrogen-deficient states [65–67].
Taken together, this integrative perspective highlights vascular health not only as a cardiovascular outcome but also as the central mediator of cognitive and psychological trajectories during the menopausal transition. Tailoring exercise prescriptions to engage these vascular pathways offers the potential to reduce cardiometabolic burden, preserve cognitive function, and stabilize mental health in obese postmenopausal women [77].
This review highlights the potential role of vascular health as a key mechanism linking exercise to cognitive and psychological outcomes in obese women undergoing the menopausal transition. Evidence shows that improvements in endothelial function, arterial elasticity, and inflammatory balance achieved through exercise extend beyond cardiovascular protection to support cerebral blood flow, synaptic plasticity, and neuroendocrine regulation. These multidimensional benefits establish a unifying framework in which vascular adaptations mediate the systemic effects of physical activity.
The conceptual contribution of this work lies in delineating a vascular–cognitive–mental health framework, integrating separate lines of research into a coherent model. This framework does not represent a novel mechanistic pathway, but rather an integrative concept that synthesizes existing evidence linking vascular, cognitive, and psychological domains. Rather than treating vascular, cognitive, and psychological domains independently, this framework emphasizes their interdependence and underscores vascular health as a key mediator through which exercise may influence systemic outcomes. This perspective is particularly important for postmenopausal women, where estrogen deficiency magnifies vascular vulnerability and increases the risks of cognitive and mental health decline.
From a translational standpoint, these insights highlight the value of tailoring exercise prescriptions to clinical and community settings. Practical approaches include community walking groups, supervised resistance programs, and digitally supported home-based interventions, all of which can improve accessibility, adherence, and sustainability. Mental health outcomes should be regarded as co-primary endpoints in exercise trials, given their profound impact on quality of life, functional independence, and sustained engagement in physical activity. Among the available modalities, CT that integrates aerobic and resistance exercise may represent an effective and practical approach in clinical practice, as it simultaneously addresses vascular, musculoskeletal, and psychological domains. In contrast, hypoxic and HIIT interventions, while showing promise, may require careful consideration depending on individual characteristics and current evidence limitations with close medical supervision in postmenopausal women with comorbidities. Prioritizing these tailored approaches may help optimize cardiovascular, cognitive, and mental health outcomes in this vulnerable population.
Future research should explicitly evaluate this integrative model by measuring vascular, cognitive, and psychological outcomes within the same intervention frameworks, with particular emphasis on sex-specific responses and the development of precision exercise strategies tailored to individual vascular, hormonal, and metabolic profiles. Longitudinal and stage-specific studies are needed to clarify how exercise prescriptions can be optimized across different phases of the menopausal continuum, and whether vascular biomarkers such as FMD or PWV can predict neurocognitive and mental health benefits. Incorporating digital monitoring and biomarker-based feedback systems may further advance precision exercise medicine. By moving beyond isolated assessments, such research will refine the evidence base and generate comprehensive strategies to reduce the compounded risks of obesity and menopause.
1RM: one-repetition maximum
AT: aerobic training
BDNF: brain-derived neurotrophic factor
BMI: body mass index
CRP: C-reactive protein
CT: combined training
eNOS: endothelial nitric oxide synthase
FMD: flow-mediated dilation
HIF-1α: hypoxia-inducible factor-1α
HIIT: high-intensity interval training
HPA: hypothalamic–pituitary–adrenal
HRmax: maximal heart rate
IL-6: interleukin-6
NO: nitric oxide
PWV: pulse wave velocity
RT: resistance training
SBP: systolic blood pressure
TNF-α: tumor necrosis factor-α
VEGF: vascular endothelial growth factor
VO2max: maximal oxygen uptake
This study was supported by the KU Research Professor Program of Konkuk University.
JJ: Conceptualization, Methodology, Writing—original draft, Visualization. HYP: Conceptualization, Supervision, Writing—review & editing. Both authors read and approved the submitted version.
The authors declare no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 980
Download: 18
Times Cited: 0
