 Review
Review

Affiliation:
1Department of Biotechnology, Saveetha School of Engineering, Saveetha Institute of Medical and Technical Sciences, Chennai 602105, India
Email: vickramas.sse@saveetha.com
ORCID: https://orcid.org/0000-0003-4319-1575
Affiliation:
1Department of Biotechnology, Saveetha School of Engineering, Saveetha Institute of Medical and Technical Sciences, Chennai 602105, India
ORCID: https://orcid.org/0009-0003-0473-970X
Affiliation:
1Department of Biotechnology, Saveetha School of Engineering, Saveetha Institute of Medical and Technical Sciences, Chennai 602105, India
ORCID: https://orcid.org/0000-0001-9079-7778
Affiliation:
1Department of Biotechnology, Saveetha School of Engineering, Saveetha Institute of Medical and Technical Sciences, Chennai 602105, India
ORCID: https://orcid.org/0009-0006-1204-0423
Affiliation:
1Department of Biotechnology, Saveetha School of Engineering, Saveetha Institute of Medical and Technical Sciences, Chennai 602105, India
ORCID: https://orcid.org/0000-0002-8427-3449
Affiliation:
1Department of Biotechnology, Saveetha School of Engineering, Saveetha Institute of Medical and Technical Sciences, Chennai 602105, India
ORCID: https://orcid.org/0000-0002-5420-8662
Affiliation:
1Department of Biotechnology, Saveetha School of Engineering, Saveetha Institute of Medical and Technical Sciences, Chennai 602105, India
ORCID: https://orcid.org/0000-0002-7863-544X
Affiliation:
2Centre for Research Impact & Outcome, Chitkara College of Pharmacy, Chitkara University, Rajpura 140401, Punjab, India
Email: chopraontheride@gmail.com
ORCID: https://orcid.org/0000-0001-8867-7603
Explor Med. 2026;7:1001408 DOI: https://doi.org/10.37349/emed.2026.1001408
Received: November 21, 2025 Accepted: March 13, 2026 Published: June 03, 2026
Academic Editor: Gennaro Daniele, Phase 1 Program at the Fondazione Policlinico Gemelli, IRCCS, Italy
The increasing survival rates among paediatric and adolescent cancer patients has increased attention on long-term consequences of chemotherapy, particularly male fertility. This review addresses age- and dose-dependent gonadotoxicity and drug type on reproductive potential. It further investigates the damage, including disruption of the hypothalamic-pituitary-gonadal axis and epigenetic alterations that may pose transgenerational risks. A systematic search of PubMed, Scopus, Web of Science, and Google Scholar was conducted for studies from database inception to April 2025. Inclusion criteria included paediatric and adolescent male cancer patients or adult survivors of childhood cancer and reported chemotherapy-related effects on fertility. Preclinical animal models were included to elucidate epigenetic changes. Due to heterogeneity of study designs, a narrative synthesis was performed to categorize findings into hormonal, cellular, and clinical outcomes. Chemotherapy-induced infertility is highly dependent on the developmental stage and specific regimen. Alkylating agents and platinum-based therapies were consistently associated with impaired spermatogenesis, hormonal disruption, and azoospermia or oligospermia. Chemotherapy and cranial irradiation were altered hormonal system that regulates male reproduction and persists epigenetic changes in germ cells. Fertility preservation for postpubertal males is through sperm cryopreservation, while prepubertal boys relied on experimental strategies such as testicular tissue cryopreservation and in vitro spermatogenesis. Chemotherapy induces epigenetic after-effects, including altered DNA methylation patterns that persist even after spermatogenesis recovers. Chemotherapy compromises male fertility through cytotoxic damage and potential long-term genomic instability. The findings highlight that reproductive recovery does not guarantee genomic recovery (epigenetically intact sperm). Consequently, oncofertility care must adapt a reproductive health model that prioritizes early, customized counselling and use of biomarkers to better predict and preserve fertility in young survivors. Although sperm banking remains a standard approach for postpubertal, promising experimental may expand fertility options for prepubertal boys in future.
The rising survival rates among children and adolescents diagnosed with cancer (> 80%) have an increased attention toward the long-term adverse effects particularly infertility associated with cancer and its treatment where 42–66% of patients facing chemotherapy induced infertility [1, 2]. The number of cancer survivors has steadily grown because of earlier cancer identification and advances in cancer therapy and medical care [3]. As a result, it is projected that the overall population will have more cancer survivors. Several studies on male survivors of childhood cancer have shown impaired gonadal function [4]. Semen analysis is currently the most reliable method for estimating male reproductive potential in their reproductive age [5]. Young adult survivors of paediatric cancer often show reluctance in providing semen samples for analysis. Therefore, to determine reproductive function, at least initially, it may be more practical to use reliable markers that reflect gonadal activity in males [6]. Semen cryopreservation is one of the well-established and effective fertility preservation methods for adults [7]. Although sperm banking is advised for all male pubertal patients, it is not often used in paediatric oncology centres, and relatively few adolescent-friendly facilities exist [8]. Therefore, improving the quality of life for cancer survivors has thus become a major public health concern. Therapy-induced toxicities can lead to both late-onset and long-term complications and infertility could be one of them (Figure 1). Moreover, earlier studies suggested that the prepubertal period offers a degree of protection against chemotherapy induced gonadotoxicity based on the assumption that the testes remain in a ‘quiescent’ or inactive developmental state during this time [9]. However, recent studies indicates that testicular tissue is susceptible to damage from oncological treatments across all developmental stages, challenging the notion of inherent resistance during childhood [10].
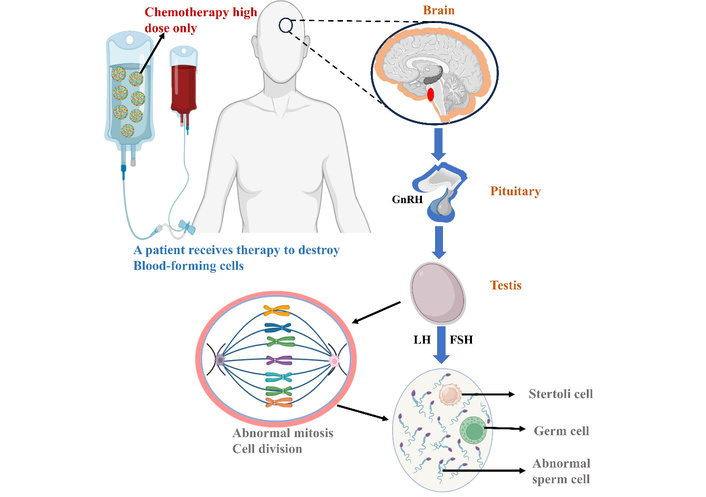
Effect of high-dose chemotherapy on spermatogenesis and the male reproductive hormonal axis. High-dose chemotherapy agents target rapidly dividing cells, including blood-forming cells and germ cells, leading to abnormal mitosis and sperm production. The diagram illustrates the disruption of the communication pathway between the brain and the testis. GnRH: gonadotropin-releasing hormone; LH: luteinizing hormone; FSH: follicle-stimulating hormone.
The idea that the prepubertal testis “dormant” and protected is an oversimplification. Emerging evidence indicates that this developmental stage is a critical window for the establishment of spermatogonial stem cells (SSCs). Damage during this period can irreversibly deplete the foundational stem-cell pool before meiosis begins [11]. Hence, prepubertal testis should be regarded not as “resistant,” but as highly vulnerable, particularly to alkylating agents that affect SSCs. According to patients, fertility is an important consideration in the informed discussion of treatment options. Also, in a survey of cancer survivors, majority of patients prefer to have a family in the future and believe they were not given enough information about their choices of preserving their fertility [12]. They also indicated inadequate counselling regarding the potential adverse effects of oncologic treatments on reproductive health. Male paediatric patients are having a higher risk of developing permanent infertility compared to females, likely due to the greater resistance of ovarian tissue to the gonadotoxic effects of chemotherapy and radiation therapy [13, 14]. The purpose is to combine the most recent data about the long-term effects of chemotherapy on male fertility in three patient groups: (1) prepubertal children (before onset of puberty), (2) adolescents (peripubertal or pubertal individuals), and (3) young adults (postpubertal). Therefore, treatment effects on fertility are discussed in relation to these developmental stages. While existing studies have covered fertility rates and preservation, this review examines the qualitative impact of chemotherapy, specifically, the epigenetic alterations and transgenerational risks that persist even after spermatogenesis recovers.
To provide a comprehensive overview of the long-term effects of paediatric and adolescent chemotherapy on male fertility, a systematic literature search was conducted. Electronic databases, including PubMed, Scopus, Web of Science, and Google Scholar, were queried for studies published from inception up to April 2025. Search terms were used individually and in combination with Boolean operators (“AND/OR”), including: “male fertility,” “gonadotoxicity,” “chemotherapy,” “paediatric oncology,” “adolescent cancer survivors,” “spermatogenesis,” “fertility preservation,” “sperm banking,” “HPG axis,” and “biomarkers of infertility.”
Studies involving paediatric or adolescent male cancer patients (ages 0–19), as well as adult survivors of childhood cancers.
Studies reporting fertility outcomes, gonadotoxicity, sperm parameters, reproductive outcomes (paternity rates), or fertility preservation.
Preclinical animal models were included to elucidate epigenetic changes and hypothalamic-pituitary-gonadal (HPG) axis disruption.
Original research, systematic reviews, meta-analyses, and clinical guidelines.
Full-text articles published in English.
Non-oncological causes of infertility
Studies focusing solely on female fertility
Editorials, conference abstracts without full text
Titles and abstracts were screened for relevance, followed by a full-text review of eligible articles. For each included study, data were extracted based on type of chemotherapy regimen, cumulative dosage, age at treatment, and long-term reproductive outcomes. Due to the heterogeneity of the study designs i.e., ranging from retrospective cohort studies to experimental animal models, a meta-analysis was not performed. Instead, a narrative synthesis was conducted to categorize findings into hormonal, cellular, and clinical outcomes (fertility rates).
The testes are highly sensitive to cytotoxic agents because spermatogenesis depends on rapidly dividing germ cells and tightly regulated endocrine control [15]. Testicular function relies on the precise interplay between Leydig cells and seminiferous tubules to support spermatogenesis, a process highly susceptible to cytotoxic interference. Spermatogenesis is a continuous, highly regulated process of cell proliferation, meiosis, and differentiation by which SSCs develop into mature spermatozoa, occurring from the onset of puberty and persisting into senescence [16]. Radical unilateral orchiectomy remains the conventional treatment for testicular malignancies [17]. A decline in sperm concentration and the development of azoospermia has been reported following orchiectomy. However, the extent of these changes varies across studies and depends on testicular function and disease [18]. Another method that may cause fertility damage is the dissection of retroperitoneal lymph nodes combined with radical orchiectomy [19]. This is because the surrounding sympathetic ganglia, which oversee emission and ejaculation, are injured. Retroperitoneal lymph node dissection, which involves removing all lymph nodes in the retroperitoneal region, eventually leads to anejaculation in almost all cases [20]. A wide broad range of late effects may arise to varying extents due to cytotoxic mechanisms associated with therapeutic interventions. Cardiopulmonary, neurological, psychological, and endocrine complications are among them. In fact, as compared to the general population, survivorship is consistently linked to higher frequency of hospital visits and longer hospital stays. Alkylating agents, such as cyclophosphamide and procarbazine, are particularly damage the germinal epithelium and easily penetrate the blood-testis barrier, targeting cells with high mitotic activity. The extent of this gonadotoxicity is not uniform, it is heavily influenced by the specific drug regimen, cumulative dosage, and patient’s developmental stage [21]. Damage to the developing SSC pool during prepubertal phase can permanently limit future sperm-producing capacity. In adolescents, the rapid growth of testicular tissue renders both germ cells and hormonal regulation vulnerable, whereas in young adults, treatment primarily targets active spermatogenesis, with recovery dependent on the survival of the stem cells.
The harmful effects that therapy may have on the gonads and the subsequent implications for fertility are among the most typical concerns for both young and adult patients. Permanent or temporary infertility may result after oncological chemotherapy, depending on whether single agents or combination regimens were used [22]. The extent of gonadotoxicity is influenced by several factors, including the specific drug, its dosage, frequency of administration, the type of malignancy being treated, and the concurrent use of other medications such as immunosuppressants. Furthermore, while the gonadotoxic profiles of traditional chemotherapies are well-documented, the reproductive impacts of emerging targeted treatments like cytokine-based immunotherapies designed to modulate the tumor microenvironment [23]. To help develop preventive methods, it is crucial to understand the precise processes by which various types of chemotherapeutic drugs directly target and harm the prepubertal testis. Recent clinical data highlight the variability in gonadotoxicity across different drug classes and patient ages. As detailed in Table 1, specific agents exhibit distinct toxicity profiles based on cumulative dosages. For instance, in adolescents and adults treated for Chronic Myeloid Leukemia, Imatinib at doses of 240 mg/m2 has been linked to decreased sperm density and survival rates. Similarly, in colorectal cancer patients, Oxaliplatin and 5-fluorouracil regimens have resulted in subnormal sperm counts. High-dose chemotherapy in Ewing sarcoma and osteosarcoma often results in permanent spermatogenic failure.
Summary of age-dependent gonadotoxic effects of chemotherapy in males across developmental stages.
| Age range/Stage | Tumor type | Anticancer agent | Degree of gonadotoxicity | Ref |
|---|---|---|---|---|
| Adolescents and adults | Chronic myeloid leukemia | Imatinib | Decreased sperm density, count, morphology | [24] |
| Young adults (20–39 years) | Hodgkin lymphoma | Doxorubicin bleomycin vinblastine dacarbazine | Increased sperm anomalies, reduced sperm concentration | [25] |
| Paediatric | Testicular cancer | Ionizing radiation | Testosterone abnormalities | [26] |
| Children and adolescents | Acute lymphoblastic leukemia | Cyclophosphamide | germ cell depletion and risk of azoospermia | [27] |
| Adolescents (15–19 years) and children | Malignant B-cell origin lymphoma | ABVD, BEACOPP, OEPA-COPDAC (Etoposide/Dacarbazine) | High risk; linked to azoospermia and affects spermatogenesis | [28] |
| Children, adolescents and adults (6–39 years) | Osteosarcoma | Ifosfamide | Azoospermia, oligospermia and sometimes results permanent infertility | [29] |
| Children and adolescents (2–25 years) | Ewing sarcoma | Ifosfamide, high-dose chemotherapy | Permanent spermatogenic failure | [30] |
| Paediatric | Solid tumors (e.g., Rhabdomyosarcoma) | Cyclophosphamide | Infertility, impaired spermatogenesis, and Leydig cell dysfunction | [31] |
| Adolescents and adults (17–39 years) | Germ cell tumor | Cisplatin | Severe oligospermia or azoospermia | [32] |
| Children (0–17 years) | Acute leukemia | Irradiation | Gonadal failure, with increased FSH levels | [33] |
Chemotherapy doses are expressed as mg/m2 or g/m2 (cumulative body surface area-based dose). Radiation dose is expressed in Gy, a SI unit of absorbed radiation dose. Gy: Gray (unit of absorbed radiation); Units: mg/m2: milligrams per square meter of body surface area; g/m2: grams per square meter.
Alkylating agents like procarbazine and cyclophosphamide are frequently associated with an increased risk of permanent infertility [33]. Chemotherapy regimens exhibit different levels of gonadotoxicity; for example, mustine, oncovin, procarbazine, and prednisone are more likely to cause azoospermia than regimens such as BEP (bleomycin, etoposide, and cisplatin) for testicular cancer or adriamycin, bleomycin, vinblastine, and dacarbazine for Hodgkin’s disease [34]. For up to two years after the treatment, males who received bleomycin, etoposide, and cisplatin (BEP) for testicular cancer have shown signs of chemotherapy-induced sperm diploidy, which may indicate that the chemotherapy directly contributes to sperm genetic damage [25]. Procarbazine, which is presently considered to be one of the most gonadotoxic alkylating substances, induce severe gonadal damage and long-term sterility by forming covalent bonds that break DNA double strands [35]. Additionally, mice’s seminiferous tubules were nearly devoid of germ cells 30 days after receiving a single 400 mg/kg treatment [36]. This was not a long-lasting impact for two months after treatment; testes weight was fully recovered in parallel with repopulation. The risk of gonadotoxicity varies substantially by developmental stage. In prepubertal children, the testis contains a developing SSC, so injury at this early stage can limit sperm-producing capacity later in life. In adolescents, the testes grow rapidly, which makes both developing germ cells and hormone regulation vulnerable to treatment [37]. In young adults, spermatogenesis is established, and treatment mainly affects actively dividing germ cells; the chance of recovery depends largely on whether SSCs survive and the cumulative dose exposure.
When administering cyclophosphamide alone, dosages of 19 g/m2 are necessary to produce prolonged azoospermia. After completing cyclophosphamide, a follow-up of 26 male patients with azoospermia, 12 individuals resumed spermatogenesis within a period ranging from 15–49 months, with a mean recovery time of 31 months [38]. A preclinical study on prepubertal mice showed that cyclophosphamide exposure triggers rapid transcriptomic reprogramming, including the perturbation of apoptotic and developmental pathways, as early as 16 hours post-treatment [39]. The cumulative dosage of cyclophosphamide was associated with the occurrence of gonadal dysfunction. Busulfan is used in a hematopoietic cell transplant preparation regimen. One dosage of 40 mg/kg was sufficient to damage germ, Sertoli, and Leydig cells in prepubertal rats for up to 10 weeks, after treatment there was a mild recovery [40]. Clinical reports of busulfan in male patients on a cumulative exposure level between < 14 mg/kg and ≥ 16 mg/kg revealed no significant differences in the onset of infertility. Melphalan also functions as an alkylating agent and, when given to juvenile rats, it has been shown to decrease testosterone levels and induce the loss of germ cells. When alkylating agents are used together with platinum-based drugs, such as cisplatin or carboplatin, it has been found that patients had a higher incidence of impaired spermatogenesis, as indicated by elevated follicular-stimulating hormone (FSH) or low inhibin B, compared to those exposed to alkylators alone [41]. According to childhood medulloblastoma cancer survivor male patients, even moderate dose and cumulative doses of cisplatin have been linked to lower livebirth rates [42]. There was no discernible link between cisplatin exposure and infertility in other investigations. Although there were no laboratory studies specifically involving humans, preclinical models demonstrate that cisplatin can decrease germ cells. Also, seminiferous tubules maintained a degenerated appearance with a less severe phenotype over the same recovery period.
An integrated system including the testis, pituitary, and hypothalamus is responsible for maintaining normal spermatogenic processes and regulating the proper release of male hormones. The neuroendocrine activities along the HPG axis play a major role in the endocrine regulation of spermatogenesis [43]. Normal reproductive competence requires the proper development and organization of the HPG axis. Gonadotropin-releasing hormone (GnRH) is a key molecule that controls how the HPG axis functions. Primary or peripheral gonadal failure is most predominantly arisen by gonadal or pelvic irradiation or direct gonadotoxic effects of chemotherapy, especially alkylating drugs. Such interventions have the potential to permanently damage the gonads’ germ cells and somatic support cells, which might result in decreased sex steroids (testosterone), hampered gametogenesis, and either premature gonadal insufficiency or pubertal failure [44]. FSH and luteinizing hormone (LH), two important endocrine signals secreted by the pituitary gland, are controlled by a strong and pulsating release of GnRH from the hypothalamus [45]. When any of these functions are dysregulated, puberty may be delayed or may not present at all, which may lead to infertility, as shown in Figure 2. Reduced FSH and LH production from low GnRH leads to hypogonadotropic hypogonadism, which in turn causes reduced androgen secretion and compromised spermatogenesis [46].
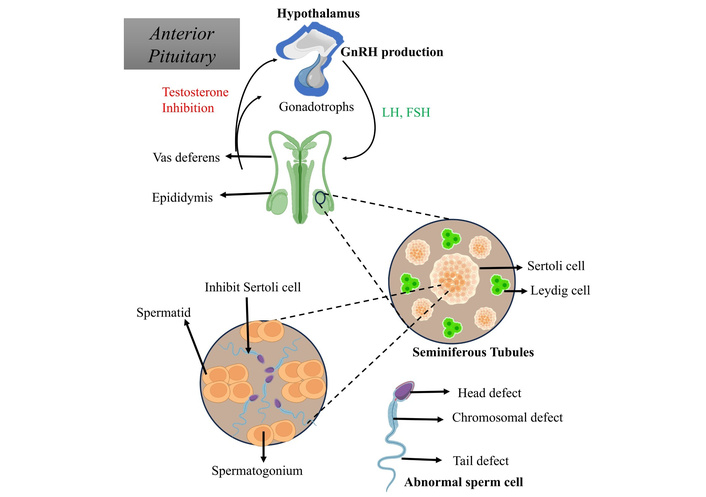
Hormonal and cellular pathways interrupt spermatogenesis in male reproduction. The figure details the feedback loop between the anterior pituitary and the testis. Disruption leads to the inhibition of Sertoli cells and the production of abnormal sperm cells (head, chromosomal, or tail defects).
Numerous variables, including as the patient’s age at therapy onset, sex, cumulative dosage, and kind of chemotherapeutic drugs, radiation dose and field, and time since treatment conclusion, influence the likelihood and degree of HPG axis dysfunction. GnRH secretion by the hypothalamus or LH and FSH secretion by the anterior pituitary might be affected by cranial irradiation, particularly when it targets the hypothalamic or pituitary regions [47]. This condition, known as central (or secondary) hypogonadism, causes the gonads to not be sufficiently stimulated, which impairs spermatogenesis and results in abnormal sex-steroid synthesis (testosterone) [48]. On the other hand, primary hypogonadism, characterized by impaired testicular responsiveness to gonadotropin stimulation due to germ cell and Leydig cell damage, frequently results from direct gonadal injury. This injury is frequently associated with exposure to alkylating agents (e.g., cyclophosphamide, busulfan) or pelvic/testicular irradiation [49]. It is known that survivors of hematopoietic stem cell transplantation with total body irradiation are more vulnerable to primary and central hypogonadism, with a high prevalence of gonadal failure and pubertal arrest observed in a subgroup [50]. Additionally, even while advances in radiotherapy techniques such as proton beam therapy try to reduce collateral damage, there is still a possibility that the HPG axis might be disrupted, when multimodal regimens are employed. Beyond reproductive impairment, the long-term impacts of HPG axis dysfunction include poor linear development, inadequate bone mineral density accumulation, and adverse psychosocial outcomes [51]. Consequently, prolonged surveillance coupled with prompt endocrine intervention constitutes a critical aspect of survivorship care in this patient population, aiming to reduce morbidity and enhance the overall quality of life. Importantly, HPG-axis vulnerability is age-dependent. In prepubertal children, cranial irradiation or chemotherapy may prevent normal pubertal activation of the axis. In adolescents, during the establishment of GnRH pulsatility, treatment may interrupt pubertal progression or result in delayed/secondary hypogonadism [52]. In young adults, the HPG axis is already developed, so damage is more likely to appear as low testosterone levels, increased gonadotropins, and reduced sperm production.
Radiation has been shown to decrease spermatogenesis, alter hormone production, and result in infertility. At 0.1–1.2 grey (Gy), radiation dosages start to negatively impact spermatogenesis, and at 4 Gy the damage is permanent [53]. Permanent azoospermia results from fractionated testicular irradiation at target doses of 20 Gy [54]. This therapy is often administered to individuals who have testicular carcinoma in situ (CIS) or as a follow-up procedure after testis-conserving surgery for a minor testicular cancer. Leydig cells can survive up to 30 Gy of radiation, making them more resilient to damage from radiation. However, it may take up to 9 years after therapy for spermatogenesis to recover [55]. There is still uncertainty about the maximum dosage levels at which persistent azoospermia becomes unavoidable. In leukaemia, less than 20% of individuals who get this therapy have been found to recover their gonadal function. Radioiodine 131I may interfere with spermatogenesis when given to individuals with thyroid cancer in a single standard dosage [56]. However, excessive cumulative dosages may cause permanent damage, thus patients who are expected to need multiple 131I treatments ought to think about semen cryopreservation. There is reason to be concerned about the extent of genetic damage induced to the spermatozoa during the treatment as radiation and the majority of cytotoxic chemotherapies harm genomic material. Even potential genotoxic cancer treatments have been shown to cause relatively few or no detectable mutations in human SSCs, at least according to the current methodologies [57, 58]. This is supported by a large number of research on offspring conceived often a year or more after therapy when the sperm cells would have been produced from living stem cells. The children of male survivors of radiation exposure from the atomic bomb in Japan and the children of survivors of childhood cancer treated with radiation and/or possibly mutagenic chemotherapy are two important studies. Specifically, alkylating agents and radiation may induce mutations in spermatozoa and spermatids, whereas topoisomerase inhibitors can alter spermatocytes, and some nucleoside analogs can alter early spermatocytes and spermatogonia. Chemotherapy and radiation therapy together will cause higher gonad toxicity than either treatment alone [59]. Apart from the effects on sperm concentration, radiation therapy has been shown to increase sperm DNA fragmentation, with these effects potentially lasting for up to two years after treatment [60]. As a result, even if spermatogenesis recovers, it still influences fertilization rates. Higher degrees of spermatocytic damage are caused when the testes receive an increasing dosage of dispersed radiation during radiotherapy for Hodgkin’s disease or retroperitoneal lymph node metastases of testicular cancer [61]. The radiation dose will be reduced by shielding the gonads, but dispersed radiation may still be quite harmful.
In spermatogonia, radiation and alkylating agents can induce single gene mutations as well as chromosomal translocations [62]. As a result, it has become standard practice to advise patients to postpone pregnancy for 3–4 months following treatment to allow for the restoration of healthy sperm [63]. Chromosome abnormalities are 10–15 times more prevalent in fertile patients, and they have been on the rise in infertile patients, accounting for 4.3% of oligozoospermic patients and 20.6% of azoospermic patients [64, 65]. According to new research, epigenetic modifications that do not involve modifications to the DNA sequence itself can be passed down via the male germline in both human and animal models, which may exert potential consequences in the health outcomes of subsequent generations [66]. Epigenetic inheritance mechanisms include DNA methylation, retained histone alterations, and small non-coding RNAs. Among these, the most studied inheritance mechanism is DNA methylation particularly when germ cells are exposed to chemotherapy agents. DNA methyltransferases (DNMTs) regulate DNA methylation patterns, and they may be hindered by substances like 5-azacytidine and 5-aza-2'-deoxycytidine (decitabine), the latter of which is used therapeutically to treat cancer. A longitudinal study of a testicular germ cell tumor patient treated with BEP chemotherapy identified 179 early differentially methylated regions, 43 of which remained epigenetically altered even 24 months post-therapy [67]. Exposure at the spermatid stage seemed to have no discernible effect, but exposure during the spermatocyte stage had milder effects. Moreover, chemotherapeutic regimens not specifically formulated to inhibit DNMTs have nonetheless been shown to induce alterations in sperm DNA methylation patterns when administered continuously throughout the entire spermatogenic cycle. These epigenetic alterations have been correlated with early postnatal mortality in offspring; the precise causal mechanisms underlying the relationship between DNA methylation changes and the observed outcomes have yet to be clearly established. Even though azoospermia is often the most visible clinical concern, a risk exists in survivors retaining sperm production while carrying chemotherapy-induced DNA methylation abnormalities [68]. This ‘Epigenetic Legacy’ challenges the current reliance on standard semen analysis. Survivorship guidelines should differentiate between reproductive recovery (the ability to achieve conception) and genomic recovery (the production of epigenetically intact sperm). Radiation and chemotherapy cause genetic instability in rodents, which may be passed on to offspring and later generations. In some cases, this can lead to reduced growth, learning, and reproductive potential as well as an increased susceptibility to cancer [69]. Instead of genetic transmission the inheritance patterns of these transgenerational abnormalities suggest epigenetic transmission. Evidence from various studies indicates that both spermatogonia and spermatids exhibit susceptibility to the induction of transgenerational effects, although none of these studies have determined if there is a dependency on the stage of germ cells [70]. Chemotherapy-induced damage may significantly affect a patient’s subsequent reproductive result, potentially affecting fertility and impairing the development of sexual traits. SSCs, a kind of male germ cell, and functional supporting somatic cells must continue to survive for long-term fertility. Chemotherapeutic drugs may harm SSCs and may cause genetically aberrant sperm precursors in addition to acute consequences [71]. Although preclinical models provide consistent evidence that chemotherapy and radiation can induce epigenetic alterations in germ cells, the corresponding evidence in humans remains comparatively limited. In the offspring of cancer survivors, most of the available studies are observational, and the associations reported between parental cancer treatment, epigenetic modifications, and health outcomes do not establish definitive germline epigenetic inheritance [72]. Human research in this area is difficult because many other factors can influence outcomes, including parental age, lifestyle, environment, and the direct impact of the original cancer. It is also challenging to separate epigenetic changes that are genuinely inherited from those that arise after birth. For these reasons, while the mechanistic data from preclinical models are strong and biologically credible, current human evidence should be interpreted cautiously and regarded as largely associative rather than confirmatory.
Male gonads tend to be protected from radiation damage. However, there are two exceptions, whole body radiation prior to bone marrow transplantation and in application of irradiation as a therapeutic modality in case of tumor cell involvement in the testis. Testicular irradiation therapy of administered doses ranging from 16–18 Gy for the treatment of testicular CIS is strongly associated with a high incidence of irreversible sterility [73]. Numerous studies have been conducted on post-treatment fertility. Apart from the oncological treatment that the patient has received, his pre-treatment fertility condition appears to be a significant predictor of post-therapy spermatogenic recovery. For example, males with stage 1 seminomas who had just undergone para-aortic irradiation showed a high rate of sperm recovery than in patients treated for testicular germ cell tumor (TGCT) still, no cases of azoospermia were witnessed [74]. In contrast, 55–80% of males who had chemotherapy based on cisplatin were spotted sperm recovery. Chemotherapy based on carboplatin was linked with lower spermatogonial damage [75]. Cancer therapy has the potential to induce genetic mutations in germ cells, which may elevate the risk of developmental abnormalities and paediatric disorders, including congenital malformations [76]. Crucially, there was no documented elevated risk for congenital abnormalities. Also, children of males who had previously had chemotherapy or radiation treatment for cancer did not have an increased incidence of juvenile malignancies, except for some types of hereditary cancers.
A comprehensive assessment of reproductive health in cancer survivors should include a detailed history of cancer treatment. In male patients aged 13 years and older, this assessment should also include a comprehensive sexual history. For survivors of childhood, adolescent, and young adult cancers, exposure to increasing doses of cyclophosphamide, procarbazine, or ifosfamide exceeding 50g/m2 is associated with a lower probability of achieving future paternity, though current supporting data is limited in quality [77]. Despite their limited participation in formal studies, several substances often used in conditioning regimens for hematopoietic stem cell transplants, including busulfan, melphalan, fludarabine, and ifosfamide, have also been implicated based on expert consent. A dose-dependent association between exposure to alkylating agents and paternity outcomes was observed in a childhood cancer survivor study [78]. Male survivors who were treated with cyclophosphamide, procarbazine, ifosfamide, or cisplatin exhibited significantly lower rates of fatherhood compared to their sibling controls [79]. However, individual reproductive outcomes are not always predicted by cumulative medication dosage. The St. Jude Lifetime Cohort Study found that sperm concentration and cyclophosphamide equivalent dosage were negatively correlated [80]. However, since some patients showed total germ cell loss even at low doses, it was difficult to determine a precise threshold for azoospermia. These findings strengthen the idea that all male survivors exposed to alkylating agents should be considered at risk for altered spermatogenesis, regardless of the severity of treatment, and highlight the significant interindividual variations in gonadal vulnerability. The use of serum inhibin B and FSH as surrogate indicators for azoospermia is debatable. In limited cohorts, several studies showed a direct relationship between sperm concentration and inhibin B level [81]. It was found that inhibin B had a 91% sensitivity and 90% specificity for detecting azoospermia, but in a study of 275 male survivors of childhood or teenage cancer, the positive predictive value was only 66%. Inhibin B’s specificity for detecting azoospermia was 45.0%, and its positive predictive value was 52.1% [82]. FSH had a positive predictive value of 65.1% and a specificity of 74.1%. Therefore, neither inhibin B nor FSH is a satisfactory substitute for semen analysis.
Sperm molecular components may serve as key indicators of reproductive damage. This is particularly crucial for long-term exposures such as those that occur during chemotherapy regimens in which cytotoxic medications are often administered for months rather than days [83]. The mature sperm in the ejaculate mimic the testicular conditions throughout the human spermatogenesis stage. The simplest way to measure this could be to measure alterations in mRNA [84]. Glutathione S-transferase and aldehyde dehydrogenase transcripts were found to be elevated in round spermatids in a recent study conducted on rats to examine the effects of BEP chemotherapy on drug-metabolizing enzymes [85]. These results imply that phase II metabolizing enzymes, including the glutathione S-transferase and aldehyde dehydrogenases, might be predictive biomarkers for chemotherapy-induced testicular toxicity. A number of techniques have been developed to quantify the damage to sperm DNA. The frequently used assays are the Sperm Chromatin Structure Assay (SCSA), the Terminal Deoxynucleotidyl Transferase dUTP Nick End Labeling (TUNEL), and the Sperm Chromatin Dispersion Test (SCD) [86]. Because SCSA depends on flow cytometry, it requires expensive equipment and central laboratory analysis. TUNEL and SCD, on the other hand, are easier for in-house implementation because of their simpler instrumentation needs and comparatively lower cost. In research, SCD and TUNEL in males were compared to unexplained infertility [87]. Based on chromatin structural susceptibility, SCD works via a two-step process that includes regulated DNA denaturation and protamine depletion, whereas TUNEL uses tagged nucleotides at damage regions to directly measure single- and double-stranded DNA breaks. Despite this, SCD proved to be more user-friendly, sensitive, and rapid than TUNEL. The United States Environmental Protection Agency has investigated SP22, a sperm-specific protein that declines in abundance following exposure to toxicants affecting both the epididymis and the testes. Recent human clinical updates shows that while established as a fertility biomarker across mammalian species, its expression pattern varies significantly between fertile and infertile cohorts [88]. Young males (20 to 34 years old) are most likely to develop TGCTs. Chemotherapy based on cisplatin is effective in treating about 90% of TGCTs [89]. On the other hand, this treatment increases the risk of developing secondary cancers. Several novel biomarkers, including CIS or Intratubular Germ Cell Neoplasia that represent innovative molecular targeted therapies, have been discovered to effectively distinguish between TGCT subtypes. A comprehensive classification of these markers, highlighting the differential expression between seminomas and non-seminomas. While OCT3/4 is a well-established transcription factor expressed in CIS, seminoma, and embryonal carcinoma, it is notably absent in yolk sac tumors and choriocarcinoma. Meanwhile, SOX17 offers a distinct profile, being expressed in CIS and seminoma but variable in yolk sac tumors, aiding in differential diagnosis. Other markers provide insight into chromatin structure and cell cycle regulation. For example, chromatin-associated proteins like HMGA1 are expressed across CIS, seminoma, and embryonal carcinoma, whereas HMGA2 is absent in seminoma, making it a specific marker for embryonal carcinoma and yolk sac tumors. About 40% of testicular mRNAs are carried by sperm cells, which makes the sperm transcriptome a useful, non-invasive proxy for tracking gene expression during spermatogenesis [90, 91]. A range of mRNA transcripts, such as motility-related mRNAs that exhibit reduced abundance in males with disrupted sperm motility, have been recognized as potential biomarkers of male fertility [92]. Infertile males have an unusual amount of protamine mRNAs, which are essential for chromatin packing. The anti-apoptotic marker Bcl-2 mRNA is upregulated in infertile individuals’ sperm [93]. Sperm RNA is positioned as a promising molecular biomarker for fertility assessment because these RNAs can either be retained passively or functionally contribute to processes like chromatin remodelling, gene imprinting, and early embryogenesis. Spermatogenic integrity will reflect in the epigenetic biomarkers of sperm DNA methylation patterns. Germline DNA dynamically reprogrammes during spermatogenesis, and the functioning of the testicles will be associated with abnormal methylation patterns. For instance, infertile men have abnormal methylation in both imprinted and non-imprinted genes (H19, IGF2) [94]. Extensive research in adult rodent models has explored toxicant exposure effects on sperm DNA methylation, including detailed analyses of epigenetic alterations following chemotherapy and tamoxifen-induced changes in the methylation patterns of imprinted genes. The tumor biomarkers listed in Table 2 (e.g., OCT3/4, c-Kit, SOX17, NANOG) are not only diagnostic markers for TGCT, but they also serve for long-term male fertility prognosis. These markers identify neoplastic or premalignant germ cells that frequently require gonadotoxic treatments such as radiotherapy or platinum-based chemotherapy. As a result, the presence of such biomarker-positive lesions is linked with the intensity of treatment exposure and spermatogenic loss. Furthermore, biomarkers such as OCT3/4 and c-Kit are directly involved in germ cell self-renewal and differentiation pathways; persistent expression after therapy may indicate impaired spermatogonial stem-cell recovery and, consequently, reduced fertility restoration potential [95]. A shift is needed from isolated fertility markers to a multimodal assessment model. Instead of relying on FSH alone, Inhibin B, a direct hormone product secreted by the Sertoli cells inside the testes. It acts as a direct molecular proxy for how healthy the seminiferous tubules which act as a “non-invasive biopsy” of testicular function [96]. Such an approach enables clearer differentiation between maturation arrest and Sertoli-cell-only patterns.
Tumor biomarkers for predicting fertility and recovery in testicular germ cell tumors.
| Biomarker | Classification | CIS | Seminoma | Embryonal carcinoma | Teratoma | Yolk sac tumor | Choriocarcinoma | Ref |
|---|---|---|---|---|---|---|---|---|
| OCT3/4 | Transcription factor | + | + | + | - | - | - | [97] |
| SOX2 | Transcription factor | - | - | + | - | - | - | [98] |
| SOX17 | Transcription factor | + | + | - | +/- | +/- | - | [99] |
| HMGA1 | Chromatin associated protein | + | + | + | - | - | N.O. | [100] |
| HMGA2 | Chromatin associated protein | - | - | + | - | + | N.O. | [101] |
| PATZ1 | Transcriptional repressor | N.O. | + | + | + | + | - | [102] |
| GPR30 | G protein-coupled estrogen receptor | + | + | + | +/- | + | - | [103] |
| RNF4 | E3 ubiquitin ligase | - | - | - | - | - | N.O. | [104] |
| NEK2 | Serine/threonine kinase | + | + | +/- | - | - | N.O. | [105] |
| Aurora B | Serine/threonine kinase | + | + | + | - | - | - | [106] |
| NANOG | Transcription factor | + | + | + | - | - | +/- | [107] |
| LIN28 | RNA binding protein | + | + | + | - | + | +/- | [108] |
| c-Kit (CD117) | Tyrosine kinase receptor | + | + | - | - | - | - | [109] |
| PLAP | Alkaline phosphatase isoenzyme | + | + | + | +/- | +/- | +/- | [110] |
+ = expressed; - = not expressed; +/- = variable expression; N.O. = not observed.
Current American Society of Clinical Oncology recommends that adolescents who are able to provide a semen sample right before treatment should be provided with sperm cryopreservation as the standard established technique of fertility preservation [111]. Male patients with a recent cancer diagnosis should be counselled to provide a semen sample for cryopreservation via masturbation to preserve future fertility potential. In pubertal boys who are unable to provide a semen sample through masturbation due to religious constraints or developmental limitations, alternative methods, such as penile vibratory stimulation or intraoperative rectal electroejaculation, may be employed that can be available in specialized clinical settings [112]. It is also important to recognize that spermatogenic maturation does not always correspond directly with the degree of pubertal development, as mature spermatozoa may be present during earlier developmental stages of puberty. This observation could broaden fertility options in prepubertal and peripubertal individuals. Even though cryopreservation of sperm is considered a standard method, some other methods are also widely used in fertility preservation among males in various age groups. Fertility preservation also differs by developmental stage. Prepubertal boys are unable to produce ejaculated sperm; therefore, sperm banking is not feasible, and only experimental strategies, such as testicular tissue cryopreservation are available [113]. Adolescents may already have mature sperm in the ejaculate, depending on pubertal stage. Sperm banking is feasible and may require assisted ejaculation methods when masturbation is not possible. In young adults, ejaculated sperm cryopreservation remains the standard approach, with TESE (testicular sperm extraction) or microdissection testicular sperm extraction (micro-TESE) used in azoospermic patients following treatment. When sperm cryopreservation and TESE are standard clinical practices, the approach must be tailored to the patient’s physical capabilities and developmental stage. Established methods for post-pubertal males include standard sperm cryopreservation and surgical extraction (TESE), being particularly useful for azoospermic patients despite being labor-intensive, as shown in Table 3. However, for early or pubertal boys unable to ejaculate voluntarily, assisted methods are available. Penile vibratory stimulation offers a non-invasive, simple alternative that does not require anaesthesia, whereas Electroejaculation utilizes rectal probe stimulation and is effective but necessitates anaesthesia.
Fertility preservation/restoration approaches for male cancer patients.
| Approach | Patients | Procedure | Current observations | Advantages | Considerations | Ref |
|---|---|---|---|---|---|---|
| Sperm cryopreservation | Post-pubertal males | Collection and freezing of ejaculated semen | Standard practice | Highly effective | Not suitable for pre-pubertal boys | [114] |
| TESE | Post-pubertal males | Surgical extraction of sperm cells from testicular tissue | Standard practice | Useful for azoospermic patients | Processing TESE specimens is highly labour-intensive | [115] |
| Testicular tissue cryopreservation | Pre-pubertal or Adults | Preservation of SSCs inside the tissue | Experimental | For prepubertal boys who have not yet initiated spermache | No live births have been reported | [116] |
| Electroejaculation | Early or pubertal boys | Uses electrical stimulation via a rectal probe to induce ejaculation | Available | Effective for young boys unable to ejaculate voluntarily | Requires anaesthesia | [117] |
| Penile vibratory stimulation | Early or pubertal boys | External vibratory stimulation to produce ejaculation | Available | simple in use, non-invasive, does not require anaesthesia | Adjunct methods if ejaculate is incomplete | [118] |
| Induced pluripotent stem cells | Adults | Reprogramming adult body cells into pluripotent stem cells | Experimental | can become any cell type, including germ cells | Not yet applicable in humans | [119] |
| Testicular Sperm Aspiration | Adults | To harvest sperm a needle is inserted into the testicle to aspirate testicular tissue | Clinical practice | Cost effective | May retrieve immature sperm | [120] |
| Micro TESE | Adults | Uses a microscopy to precisely extract testicular tissues exhibiting highest likelihood of spermatogenesis | Clinical practice | Higher success rates in difficult cases | More expensive | [121] |
| Hormonal protection strategies | Post-pubertal and adults | Administration of GnRHa, temporarily suppress gonadotropin secretion to reduce testicular activity | Preclinical level | Suitable for hormone sensitive cancers | Apart from rat studies, showing conflicting outcomes; still under investigation | [122] |
Preclinical studies are important to specifically determine the extent and underlying mechanisms of testicular damage caused by chemotherapy drugs during the prepubertal stage. Being aware of the exact mechanisms by which chemotherapy drugs affect the prepubertal testis can be valuable in developing protective or preventive measures. Sperm banking, despite being a relatively low-cost and simple procedure, remains significantly underutilized in industrialized nations, including those countries with universal healthcare systems that cover its cost [123]. However, in a recent Swedish registry-based cohort, 54% of men have remembered preserving semen, and 68% of men remembered getting information about sperm banking [124]. In cancer treatment settings, the most prominent challenge is still failing to provide male patients with timely information. According to the oncologist’s suggestion, parents should be engaged in their children’s education and counselling as part of the decision-making process [125]. Sperm banking is still a simple yet effective way of preserving fertility, even though banked semen is used at comparatively low rates. In a recent study involving men treated for Hodgkin lymphoma, the use of semen cryopreservation was associated with a twofold increase in fatherhood [37]. Notably, 20% of offspring were conceived using cryopreserved semen. During chemotherapy, hormonal suppression is a strategy for male fertility preservation to mitigate chemotherapy-induced gonadotoxicity by transiently inhibiting germ cell proliferation intended to promote spermatogenesis for the preservation of male fertility [126]. This method lowers intratesticular testosterone levels by inhibiting pituitary gonadotropins (LH/FSH). This is based on a hypothesis that active generation of germ cells leads to enhanced resilience against chemotherapy-induced cytotoxicity. The growth of germ cells can also be inhibited by further lowering intratesticular testosterone. Hormonal suppression during chemotherapy in rats promotes spermatogenesis to rebound from surviving stem cells by reversing a barrier in spermatogonial differentiation [127]. Post-chemotherapy in humans showed a failure for protection or restoration of spermatogenesis in 7 of 8 clinical trials [128]. Thus, therapeutic outcomes have been mostly inconsistent, with the observation that human models have had less success than animal models. Hormonal suppression is not clinically validated to be an effective method for protecting male fertility after chemotherapy. However, sperm cryopreservation is still considered the gold standard.
Semen cryopreservation prior to the initiation of chemotherapy or radiation treatment is an effective way of preserving male and postpubescent fertility. For patients who have not had their sperm cryopreserved, the recent success of TESE, together with intracytoplasmic sperm injection (ICSI) for nonobstructive azoospermia, suggests some technologies that offer a new therapeutic alternative. Sperm retrieval rates ranged from 42 to 47% across the trials [129]. Pregnancy and live birth outcomes following TESE–ICSI vary depending on the study population. For instance, one study reported a clinical pregnancy rate of 45.8% (95% CI: 39.1–52.5%) and live birth rates of 34.1% per embryo transfer and 44.5% per cycle [130]. TESE remains a viable option for patients who have not done their cryopreservation. There are currently no feasible options for ensuring future fertility in young males whose spermarche has not yet begun. Only experimental methods now provide promise for ART procedures in the future [131]. SSCs, which may be isolated from testicular tissue prior to cancer therapy, may be used in potential new fertility preservation methods (Figure 3) [132].
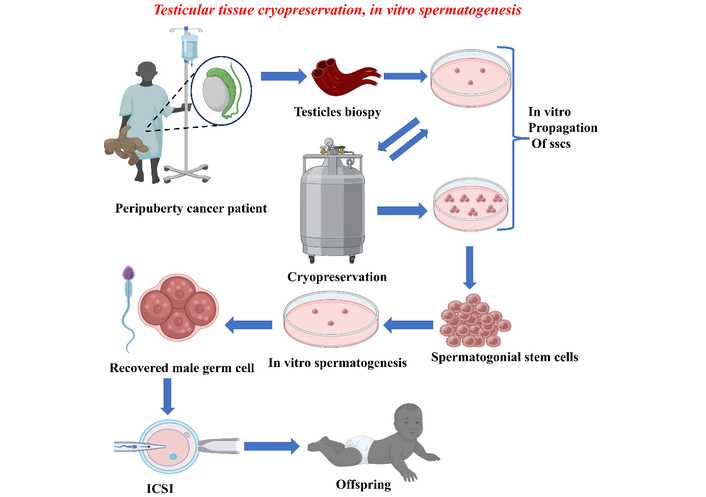
In vitro spermatogenesis and testicular tissue cryopreservation for fertility preservation. The workflow illustrates the fertility preservation for a peripubertal cancer patient. A testicular biopsy is performed to obtain tissue containing spermatogonial stem cells (SSCs) that undergo cryopreservation. Alternatively, SSCs can be isolated and cultured in vitro. These cells then undergo in vitro spermatogenesis to differentiate into mature male germ cells. Then, recovered sperm cells are used in ICSI to fertilize an egg.
Spermatogenesis does not take place in prepuberty, and so spermatozoa cannot be cryopreserved. Some oncofertility programs harvest and freeze testicular stem cells in prepubertal boys who are experiencing drug-induced germ-cell loss to maintain the fertility of childhood cancer survivors [133]. This strategy is based on early research in mice by Brinster and colleagues, who demonstrated that testicular stem cells may be used to restore spermatogenesis by transplanting them into seminiferous tubules which lacking germ cells [134]. This technique was recently used to produce spermatozoa that could fertilize oocytes in recipient macaques who had had facing chemotherapy before to puberty and in adulthood. In order to cryopreserve testicular stem cells for a prepubertal patient undergoing sterilizing chemotherapy could opt to get a testicular biopsy as a preventative measure. The stem cells that thawed from cryostorage can be reintegrated into the testicular tissue after cancer treatment in the hope of restoring spermatogenesis. Studies involving both mice and humans have demonstrated that testicular tissue containing SSCs can be cryopreserved using cryoprotective agents such as dimethylsulfoxide and sucrose [135]. This preservation can be achieved through either a slow, uncontrolled freezing protocol or via an ultrarapid vitrification method. Since these simple processes do not require expensive biofreezers, testicular tissue may be collected and cryopreserved at a procurement point that is separate from the banking and transplanting sites. Cryopreserving testicular tissue offers the possibility of future fertility restoration, either through microinjection of dissociated testicular cells into the seminiferous tubules or by grafting the frozen-thawed tissue directly into the testis [136]. Currently, this treatment is not very effective even in animal models. However, in vitro growth of the stem cells either before to freezing or upon thawing may enhance the procedure’s success rate in humans [137]. A testicular biopsy in children with tiny testes may reduce future spermatogenesis following recovery from cancer treatment, which may limit testicular germ cell transplantation to children who have a high chance (> 80%) of becoming sterile [138]. Due to the investigational status of both testicular germline stem cell storage and reimplant the prophylactic approach remains a subject of controversy. However, a new survey indicates that parents of boys with childhood cancer already embrace this approach.
National organizations like American Society of Clinical Oncology provide valuable assistance, but the cancer therapies and medications are always evolving. Despite this progress, there is still a lack of knowledge on certain important issues that patients frequently have, such as how long to take contraception following treatment or long-term effects of cancer treatments may have on the health of their future offspring, regardless of whether they were treated as adults or children. Nonetheless, the major medical associations in the USA and Europe: American Society of Clinical Oncology and the European Society for Medical Oncology, have generally consistent guidelines. For example, an ideal way to possibly maintain the fertility of men (and boys who produce sperm in the ejaculate) during chemotherapy or radiation treatment is to save semen samples [139, 140]. Therefore, all patients must be informed about cancer therapy effects on spermatogenesis and the possibility of sperm banking. The American Urological Association and the American Society for Reproductive Medicine jointly released 2024 guidelines that stress the significance of proactive fertility management in male patients receiving gonadotoxic cancer treatments [141]. Before treatment, clinicians are encouraged to discuss with patients the possible negative effects of these therapies on spermatogenesis. Prior to therapy, sperm cryopreservation through the collection of multiple specimens is highly advised to mitigate long-term fertility loss [142]. Due to the possibility of sperm genetic damage, patients are also recommended not to proceed conception for at least a year after chemotherapy or radiation treatment. The guidelines also address post-treatment follow-up, suggesting semen analysis to evaluate spermatogenesis recovery at least 12 months, and ideally 24 months, following therapy [143]. Micro-TESE remained as a fertility restoration option for those who continue to be azoospermic. A meta-analysis that included many European trials still concluded that sperm cryopreservation is the feasible and effective way of retaining fertility in adult male cancer patients. In contrast, spermatogenesis recovered in 12 months for those who received ≤ 2 cycles of bleomycin, etoposide, and cisplatin (BEP) in a multicentre review of 129 testicular cancer patients, but recovery took 24 months for those who received 3–4 rounds [144]. Despite these setbacks, azoospermic males were able to obtain a 27% live birth rate using ICSI and TESE [145]. The idea that prepubertal testes are resistant to chemotherapy was contested in a pilot study conducted by McGill University Health Centre and Institut National de la Recherche Scientifique in cooperation with oncologists and fertility specialists, and the study assessed 13 paediatric leukaemia/lymphoma survivors. Regardless of puberty status, sperm analysis showed that 85% of them had severe oligospermia or azoospermia, indicating a universal risk of infertility. The cohorts showed increased sperm DNA fragmentation, indicating that alkylating drugs such as cyclophosphamide damage genomic integrity at any developmental stage [146]. Such findings highlight the need to preserve fertility at an early age, especially in young males. These varied findings underscore the complex and context-dependent effects of chemotherapy on male fertility which are influenced by the specific cancer type and treatment regimen. Nonetheless, they collectively reinforce the global importance of implementing fertility preservation strategies within oncology care.
Long-term studies show that a significant number of male cancer survivors, between 15% and 46% continues to experience infertility. As more young people and adolescents are commencing long-term therapies, it becomes even more important for clinicians to have regular, open conversations about fertility and future family plans as part of routine care. Failure to engage in such early conversations may compromise both long-term health and reproductive health. The international oncology centres portray the considerable risk of male infertility that comes with post-chemotherapy for various cancer types and treatment approaches. Fertility preservation treatments, notably sperm banking, provide an effective way for men to protect their reproductive potential before going through chemotherapy. Researchers are becoming more engaged in understanding the long-term effects of cancer and its treatments because of the increased number of young cancer survivors and the tendency to delay pregnancy until later in life. Male oncofertility must transit from ‘survival-first’ to a ‘precision reproductive health’. A model that goes beyond freezing sperm to include the long-term surveillance of its genetic integrity. Testicular damage resulting from radiotherapy exhibits a clear dose-dependent relationship, wherein the onset, potential for reversibility, and duration of recovery of spermatogenesis are all correlated with the testicular dose of irradiation. The ongoing research and advancements in assisted reproductive technologies provide hope for fertility preservation and restoration among cancer survivors affected by such treatment-related infertility. To address this crucial component of long-term survivability, it is consistently advised to have thorough and early conversations regarding fertility risks and preservation options. This emphasizes the importance of oncofertility to include in standard cancer treatment.
DNMTs: DNA methyltransferases
FSH: follicular stimulating hormone
GnRH: gonadotropin-releasing hormone
Gy: gray
HPG: hypothalamic-pituitary-gonadal
ICSI: intracytoplasmic sperm injection
LH: luteinizing hormone
SCD: sperm chromatin dispersion test
SCSA: sperm chromatin structure assay
SSCs: spermatogonial stem cells
TESE: testicular sperm extraction
TGCT: testicular germ cell tumor
TUNEL: terminal deoxynucleotidyl transferase dUTP nick end labeling
VAS: Conceptualization, Methodology, Writing—original draft. PC: Conceptualization, Formal analysis, Writing—original draft. BSB: Data extraction, Writing—review & editing. BS: Visualization, Writing—review & editing. MMCM: Investigation, Resources. SA: Visualization, Validation. JRD: Project administration, Formal analysis. HC: Project administration, Investigation. All authors read and approved the final manuscript.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 1236
Download: 12
Times Cited: 0
