Case Report
Case Report

Affiliation:
Division of Cardiac Surgery, Department of Surgery, Dentistry, Paediatrics and Gynaecology, University of Verona, 37126 Verona, Italy
†These authors share the first authorship.
ORCID: https://orcid.org/0009-0003-2854-2784
Affiliation:
Division of Cardiac Surgery, Department of Surgery, Dentistry, Paediatrics and Gynaecology, University of Verona, 37126 Verona, Italy
†These authors share the first authorship.
Email: alessandra.francica@univr.it
ORCID: https://orcid.org/0000-0001-8674-3179
Affiliation:
Division of Cardiac Surgery, Department of Surgery, Dentistry, Paediatrics and Gynaecology, University of Verona, 37126 Verona, Italy
ORCID: https://orcid.org/0000-0003-1984-6172
Affiliation:
Division of Cardiac Surgery, Department of Surgery, Dentistry, Paediatrics and Gynaecology, University of Verona, 37126 Verona, Italy
ORCID: https://orcid.org/0000-0003-0931-018X
Explor Med. 2026;7:1001407 DOI: https://doi.org/10.37349/emed.2026.1001407
Received: November 24, 2025 Accepted: April 16, 2026 Published: May 28, 2026
Academic Editor: Carlos M. Ferrario, Wake Forest School of Medicine, USA
Tricuspid valve endocarditis has potential associations with various conditions, but it is commonly related to intravenous drug abuse. Often, its eradication can become very challenging due to high post-operative mortality and high rate of recurrence due to persistence of drug abuse habits. The bidirectional Glenn shunt (BGS), typically employed in congenital heart surgery, combined with tricuspid valvectomy, has occasionally been used for recurrent endocarditis. Herein, we present a 31-year-old woman with drug addiction scheduled for her fourth reintervention due to the early degeneration and infection of a previous pulmonary homograft used for recurring tricuspid valve endocarditis. The final surgical strategy was valvectomy and BGS, aimed at eliminating all potential sources of infection and providing more time for the patient to overcome drug addiction, enabling further treatment if necessary.
A 31-year-old woman with a history of three previous tricuspid valve procedures due to intravenous drug abuse was referred to our Unit for the fourth time because of recurring endocarditis. Her surgical journey began at age 27 with tricuspid valve repair for methicillin-resistant Staphylococcus aureus endocarditis. Two months later, she required tricuspid valve replacement with a bioprosthetic valve due to early recurrence of Staphylococcus aureus endocarditis and concomitant Candida albicans infection. A year later, she was diagnosed with a relapse of bioprosthetic valve endocarditis, leading to rapid stenotic degeneration. Given her young age, long history of intravenous drug addiction, diminutive body surface area (1.48 m2), and small, fibrotic valve annulus, she underwent prosthesis replacement using a pulmonary homograft with a previously unreported top-down technique [1]. Two years later, she was referred back to our Centre due to the third recurrence of endocarditis leading to homograft degeneration (Figure 1).
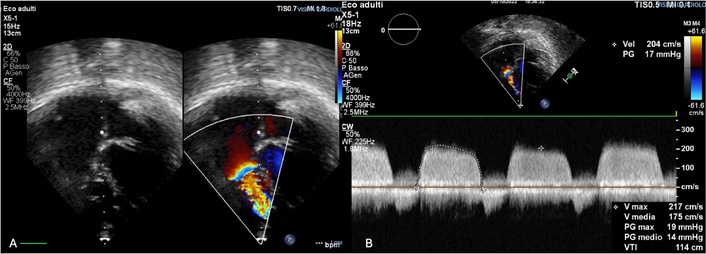
Echocardiographic evidence of homograft degeneration. (A) Homograft sclerotic degeneration at preoperative echocardiography. (B) Echo-color-Doppler assessment of trans-valvular flow.
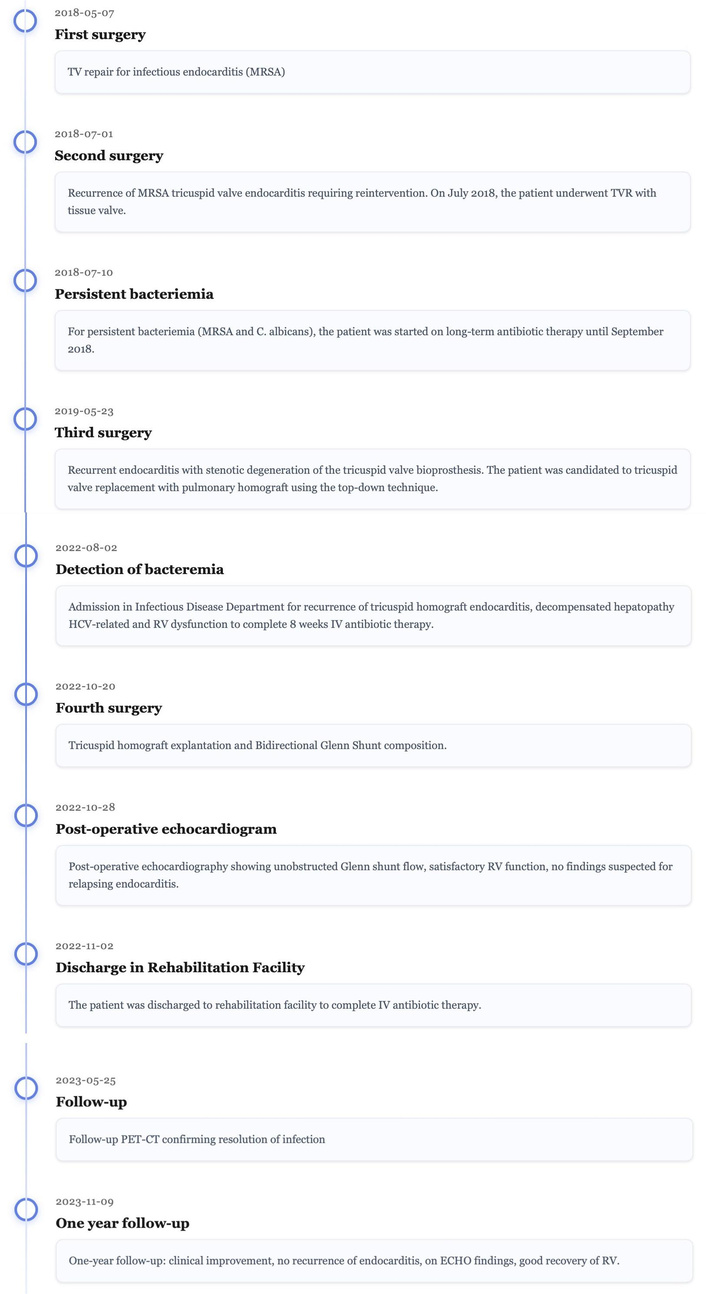
Figure 2 provides a timeline summarizing the patient’s treatment progression.
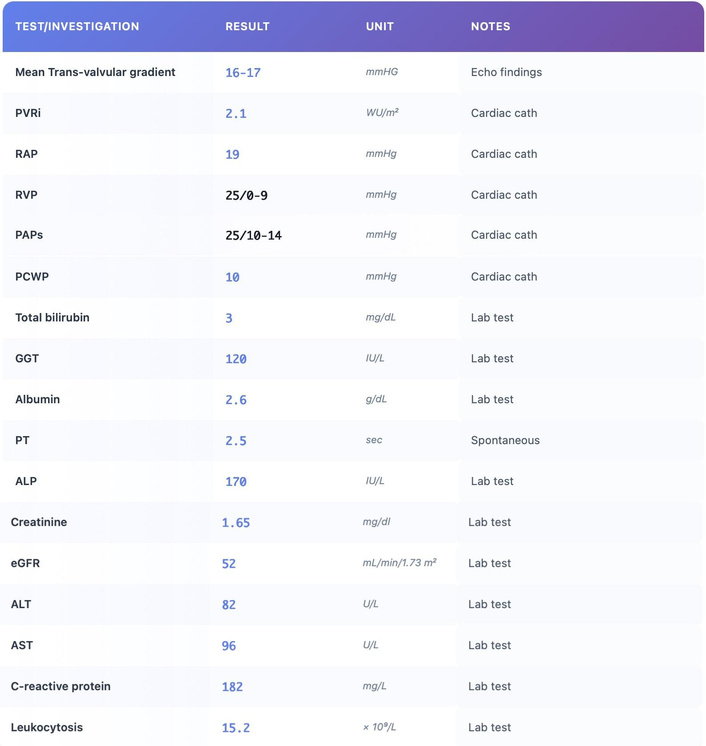
The patient presented with symptoms of right-sided heart failure, such as poor exercise tolerance, shortness of breath, and progressive impairment of renal and liver function (see Diagnostics section). According to progressive liver dysfunction, she displayed recurrent ascites requiring periodic evacuation. Her overall haemodynamic status was deemed as NYHA class III. Blood cultures were tested positive for Staphylococcus aureus. The PET-CT scan showed increased uptake around the tricuspid valve annulus of the homograft, with multiple bilateral pulmonary embolizations. The echocardiogram confirmed the deterioration of the previously implanted pulmonary homograft, with a mean transvalvular gradient of 16–17 mmHg (Movie S1). Considering her recurrent endocarditis, history of drug abuse, and unsuccessful prior surgeries, she was scheduled for homograft explanation and bidirectional Glenn shunt (BGS) to eliminate potential sources of infection in the right-sided heart. For this purpose, preoperative right cardiac catheterization was performed, confirming patient’s eligibility for Glenn circulation (PVRi 2.1 WU/m2, RAP 19 mmHg, RVP 25/0–9 mmHg, PAP 25/10–14 mmHg, PCWP 10 mmHg). The therapeutic strategy was discussed during a dedicated multidisciplinary endocarditis meeting involving cardiac surgeons, cardiologists, infectious-disease specialists, cardiac anesthesiologists, hepatologists, and addiction-medicine consultants. Arguments favoring a combined valvectomy and BGS included extreme annular destruction and hostile operative field, high risk of reinfection with any new prosthesis, preserved pulmonary vascular resistance, severe right ventricular volume overload and the patient’s willingness to enter a structured rehabilitation program. Medical therapy alone was considered insufficient in view of mechanical obstruction and ongoing embolization. Isolated tricuspid valvectomy was felt to carry unacceptable risk of refractory right-heart failure. The Glenn shunt was therefore selected to unload the right ventricle while maintaining forward pulmonary flow. The fourth median sternotomy was performed uneventfully. After starting CPB, an initial attempt to remove the pulmonary homograft on the beating heart was made. However, the heavily calcified remodeling of the homograft and the small right ventricular cavity made the procedure very challenging, thus requiring excision during a period of cardioplegic arrest. Upon initial inspection, the homograft, originally 27 mm [1], was found to accommodate only a 12 mm Hegar device. After successful homograft excision, the tricuspid annulus eventually measured 20 mm. Following the completion of annular debridement and right atriorrhaphy, the aorta cross-clamping was released, leading to the prompt resumption of sinus rhythm. Subsequently, BGS between the superior vena cava and the right pulmonary artery was completed after ligation of the azygos vein (Movie S2). Post-operative echocardiography showed unobstructed BGS flow with preserved left ventricular contractility and mildly reduced right ventricular function. The early post-operative period was complicated by need for surgical revision due to pericardial effusion and recurrent bilateral pleural effusion, likely due to associated chronic liver disease. Following optimized medical treatment, the patient was discharged on the thirteenth postoperative day on eight-week antibiotic therapy. At one-year follow-up, the patient had overcome her drug addiction. Physical examination showed optimal health, with only occasional shortness of breath during strenuous exercise (NYHA class II). There were no clinical or laboratory signs of recurrent endocarditis. Latest echocardiogram revealed preserved left ventricular function, slightly reduced right ventricular function, and a satisfactory bidirectional cavo-pulmonary shunt flow. A PET-CT scan confirmed complete resolution of the infection in the right-sided heart (Figure 1). At one-year follow-up, she remained abstinent from drug use and was in NYHA class II. Six-minute walk distance was 480 m, and cardiopulmonary exercise testing showed a peak VO2 of 19.6 mL/kg/min (68% predicted). Right heart catheterization at one year was not performed because the patient declined to undergo the procedure. Liver tests improved substantially (bilirubin 1.2 mg/dL, INR 1.2). PET-CT showed complete resolution of infection.
Figure 3 provides diagnostic results of the patient.
The patient reported significant physical and psychological improvement following surgery, particularly in terms of exercise tolerance and quality of life. She described a marked reduction in peripheral edema and fatigue and expressed relief at being free from recurrent infections. The patient acknowledged the severity of her previous condition and emphasized that the surgical intervention represented a turning point in her commitment to substance-abstinence and rehabilitation.
Relapsing right-sided endocarditis in drug-addicted patients remains a formidable challenge. While valve repair is preferable, extensive destruction often precludes reconstruction. Homografts may reduce reinfection risk, but their durability in the tricuspid position is uncertain. Previous studies have reported a 100% mortality rate in these patients due to the inability to control the endocarditis [2]. While the use of aortic homografts in aortic valve endocarditis has shown low risk of recurring infection and good long-term survival [3], mitral and pulmonary homograft tissues have rarely been used in tricuspid valve endocarditis. Whether recurrent infection in the present case was prompted by accelerated tissue degeneration, or the opposite, is matter of speculation. For drug addicts with intractable right-sided endocarditis, Arbulu et al. [2] proposed tricuspid valvectomy or pulmonary valvectomy. However, early postoperative refractory right-sided heart failure and mortality remained high. In this scenario, combining valvectomy with BGS, which unloads the right ventricle from superior vena caval flow, may mitigate early right heart failure while allowing for infection control. To the best of our knowledge, only four cases of Glenn procedure for relapsing endocarditis in drug addicts were previously reported [4, 5]. In these series, three patients eventually required tricuspid prosthesis implantation after 4–5 years of follow-up, due to late onset of right heart failure, without recurrence of infection. The fourth patient was lost to follow-up. Therefore, the BGS strategy allowed most patients to buy time to fully overcome drug addiction.
In the setting of recurrent right-sided infective endocarditis, echocardiographic evaluation represents a pivotal step, not only for confirming the diagnosis but also for guiding clinical management and risk stratification. The identification, characterization, and monitoring of intracardiac masses—particularly vegetations—are essential, given their direct implications for embolic risk and therapeutic decision-making.
In this context, recent advances in echocardiographic techniques suggest that Tissue Doppler Imaging (TDI), including both color TDI and pulsed-wave (PW) TDI modalities, may provide incremental diagnostic and prognostic value in patients with pathological right heart masses. Color TDI has been shown to enhance the visualization of intracardiac masses by improving the delineation of their motion patterns relative to adjacent myocardial structures, thereby facilitating a more accurate morphological and functional assessment. This approach may be particularly useful in differentiating highly mobile vegetations or thrombotic material from surrounding tissues within the anatomically complex right-sided chambers. Complementarily, PW-TDI enables a quantitative assessment of mass mobility through the measurement of peak antegrade velocity. This parameter has been proposed as a surrogate marker of embolic potential, with higher velocities reflecting increased mobility and, consequently, a potentially higher risk of embolization [6].
The combined use of qualitative (color TDI) and quantitative (PW-TDI) approaches may therefore enhance the overall diagnostic yield of echocardiography, allowing for a more comprehensive characterization of right heart masses. In patients with recurrent endocarditis, where accurate lesion assessment and embolic risk evaluation are of paramount importance, the integration of these advanced techniques into routine echocardiographic practice should be considered, as they may provide clinically meaningful adjunctive information beyond conventional imaging [7].
From a long-term perspective, in this patient, the Glenn shunt should not be regarded as a definitive (destination) therapy, but rather as a strategic and staged approach. The decision to perform a Glenn procedure was primarily driven by the need to achieve optimal source control of the right-sided infection. This was accomplished through a combined strategy of complete removal of prosthetic material and targeted antibiotic therapy, in the context of persistent bacteremia and ongoing metabolic activity on imaging studies suggestive of uncontrolled infection. In this setting, the Glenn shunt allowed effective exclusion and decompression of the right heart, thereby facilitating complete surgical and microbiological eradication of the infected site.
Conversion to a Fontan-type circulation was considered as a potential future option in the event of progressive right ventricular deterioration. However, this scenario did not materialize, as the patient has remained clinically stable, asymptomatic, and in good overall hemodynamic condition during follow-up. Consequently, no indication for Fontan completion has emerged to date.
Similarly, heart transplantation represents a viable therapeutic option in the case of subsequent clinical deterioration, provided that standard eligibility criteria are met, including sustained infection control and appropriate patient selection. Notably, one of the advantages of the current strategy is that it preserves the possibility for longitudinal reassessment. Should complete infection eradication be achieved and the patient develop hemodynamic intolerance to the current circulation, further surgical options—including implantation of a new prosthetic valve—may be reconsidered within a controlled and infection-free setting.
The present experience highlights that a multidisciplinary approach in such extreme and complicate case, involving all specialistic members of endocarditis team, is of paramount importance to address the patient to the most appropriate therapeutic strategy. Only throughtout a multidisciplinary assessment is it possible to get a comprehensive understanding of the physiopathology, milestone in the establishment of treatment plan.
The strategy of valvectomy combined with BGS, as previously proposed by Huang et al. [4], offers an opportunity for sterilization and potential drug habit change. Contrary to prior observations [5], the pathophysiology established did not lead to right heart failure, albeit at a shorter follow-up, possibly due to the younger age at surgery and smaller patient size in the present case.
BGS: bidirectional Glenn shunt
PW: pulsed-wave
TDI: Tissue Doppler Imaging
The supplementary movies for this article are available at: https://www.explorationpub.com/uploads/Article/file/1001407_sup_1.pdf.
VB: Writing—original draft, Writing—review & editing, Investigation. AF: Supervision. SH: Resources. GBL: Project administration. All authors read and approved the submitted version.
The authors declare that they have no conflict of interest.
Ethical approval was not required for this case report.
The consent was obtained from the patient.
Written informed consent for publication was obtained from the patient.
All relevant data are within the manuscript and its Supporting Information files.
This research received no external funding.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 527
Download: 14
Times Cited: 0