 Systematic Review
Systematic Review

Affiliation:
1College of Nursing, Wayne State University, Detroit, MI 48202, USA
Email: av6363@wayne.edu
ORCID: https://orcid.org/0000-0002-9899-1759
Affiliation:
2Department of Medical Laboratory Science, Eugene Applebaum College of Pharmacy and Health Sciences, Wayne State University, Detroit, MI 48201, USA
ORCID: https://orcid.org/0009-0005-1368-2586
Affiliation:
3Albert Einstein College of Medicine, Bronx, NY 10461, USA
ORCID: https://orcid.org/0000-0001-9742-6611
Affiliation:
1College of Nursing, Wayne State University, Detroit, MI 48202, USA
ORCID: https://orcid.org/0000-0003-1535-2597
Affiliation:
4Department of Oncology, School of Medicine, Wayne State University, Detroit, MI 48201, USA
ORCID: https://orcid.org/0000-0003-3586-1225
Affiliation:
5Comprehensive Sickle Cell Center, Children’s Hospital of Michigan, Detroit, MI 48201, USA
ORCID: https://orcid.org/0000-0003-1862-6469
Affiliation:
1College of Nursing, Wayne State University, Detroit, MI 48202, USA
ORCID: https://orcid.org/0000-0002-1356-6885
Explor Med. 2026;7:1001400 DOI: https://doi.org/10.37349/emed.2026.1001400
Received: August 29, 2025 Accepted: March 16, 2026 Published: April 20, 2026
Academic Editor: Attila Nemes, University of Szeged, Hungary
Background: Sickle cell disease (SCD) is a group of heritable conditions with significant morbidity, burden of disease management and healthcare delivery issues. Medical mistrust (MM) is a psychological outcome of healthcare delivery issues. The purpose of this review was to assess the concept of MM in the literature on SCD, summarize the findings and gaps, and was guided by three questions: 1) How has MM been measured and/or described in patients with SCD? 2) What factors have been described in the literature that predispose patients with SCD to develop MM? 3) What consequences or outcomes have been described because of MM in patients with SCD?
Methods: The methodological framework of Arksey and O’Malley was used to review articles from PubMed, Scopus, Web of Science, CINAHL, PsycInfo, and EMBASE. Inclusion criteria were quantitative, qualitative, and mixed methods peer-reviewed studies published in English between 1994 and 2025; articles focused on patients with SCD and those that described concepts found in the existing MM instruments.
Results: Forty-two studies were included; 26 were strictly qualitative, 11 were mixed methods, and 5 were strictly quantitative. No study used an existing MM measure; yet concepts from MM measures were described: group disparities and suspicion. Negative healthcare staff communication, poor pain control, transition of care, and lack of provider transparency predisposed patients toward MM. Outcomes of MM included avoidance of care, nonadherence, psychological distress, and maladaptive coping.
Discussion: This review highlights the predictors and outcomes of MM in patients with SCD and identifies the notable gaps in the state of the SCD MM literature. More studies are needed to assess the development and consequences of MM in patients with SCD. The findings highlight the experiences of patients with SCD and offer researchers insights into possible interventions to decrease MM and improve outcomes.
Sickle cell disease (SCD) is a group of heritable hematologic conditions stemming from mutations in the hemoglobin subunit beta gene (HBB). Hemoglobin comprised of mutant beta-globin polymerizes the cells which induces red blood cell (RBC) stiffness and less deformability, contributing to vessel occlusion and tissue ischemia [1, 2]. These RBCs then adhere to the endothelium and blood components, adding to vessel occlusion and repeated cycles of inflammation [3]. Polymerization also causes hemolysis through fragility of the RBCs and oxidative stress [4, 5]. These processes contribute to significant morbidity in patients with SCD, including pain crises, acute chest syndrome, stroke or silent infarction, pulmonary hypertension, kidney disease, avascular necrosis, and functional asplenia with risk for infection [6, 7]. Approximately 100,000 people live with SCD in the United States (US), a small fraction of the estimated 7.74 million affected globally [8, 9]. Despite being considered a rare disease in the US, the adverse health outcomes attributed to SCD lead to frequent utilization of healthcare services. A previous study found that individuals with SCD in the US average 2.59 care encounters per year, with an average of 1.52 of these encounters resulting in hospitalization [10]. Of the hospital admissions in this study, the rehospitalization rates within 14 and 30 days were 28.4% and 41.1%, respectively [10]. Insufficient disease management, whether through inconsistent medication, lack of a primary care physician (PCP), or missed outpatient appointments, raises the risk of vaso-occlusive events, hospitalization, and rehospitalization [11–15]. This greater need for healthcare involves increased costs. In addition to the high morbidity faced by those with SCD, which includes a 20-year reduction in lifespan on average, the total mortality burden was estimated to be 376,000 people globally [8]. Speller and colleagues [9], despite limiting their sample to SCD patients with Medicaid insurance, noted these patients, despite having a rare disease, accounted for double the average annual spending relative to others with public insurance in the US. In an earlier study by Brousseau and colleagues [10], researchers found significant differences in acute hospitalization rates between public and privately insured individuals. Most notably, adults with public insurance experienced twice as many acute care encounters [10]. To alleviate widespread morbidity, mortality, and costs from SCD, healthcare services must be effective and accessible.
With the disproportionate burden of SCD, improved disease management strategies and health system interventions are needed to enhance health outcomes in patients with SCD. One aspect of healthcare delivery that hinders disease management is medical mistrust (MM). MM is a multifaceted concept that has been broadly defined as a “lack of confidence in healthcare providers (HCPs), institutions, and systems” [16], and is not synonymous with distrust, which is an attitude based on the belief that one’s trust has been diminished or violated [16]. MM is rooted in historical events, cultural identity, and lived experiences; it encompasses the social dynamics of how patients interact with healthcare entities [16, 17]. Marginalized patients, such as people of color, LGBTQ populations, and older adults, often develop heightened levels of MM due to their encounters with healthcare discrimination and systemic inequities [18–22]. The cognitive and behavioral attributes of MM include suspicion toward the motives and practices of healthcare professionals. These attributes contribute to concerns about receiving substandard or harmful treatment and lead to underutilization of medical services [16–23]. To assess levels of MM, researchers have developed reliable and validated tools. The two most used tools are the MM Index (MMI) [23] and the Group-Based MM Scale (GBMMS) [24]. These tools quantify patients’ perceptions of the healthcare system. Decades of research using these tools [23, 24] have found that MM influences health behaviors, engagement with medical services, and interactions with providers. Previous studies have shown that those with higher levels of MM were less likely to complete health-maintenance behaviors, i.e., participating in primary screenings and adhering to treatment regimens [24–31]. Avoidance of healthcare services results in adverse health outcomes [29]. Despite the obvious overlap between patients with SCD and marginalized populations, research evaluating MM in this context is underdeveloped and represents a long-standing gap in knowledge.
The goal of this systematic review was to assess the extent and nature of the MM research available within the realm of SCD studies in order to summarize the findings and identify gaps in the literature. SCD positions most patients at the intersection of race and chronic illness, where MM is often encountered [24]. Therefore, this review will consider studies that examine patients’ perceptions of the influence of race/ethnicity on the medical care they receive. Studies that either qualitatively or quantitatively describe potential predictors of MM in patients with SCD will be considered. Based on this context, the following research questions were formulated to guide this systematic review:
R1: How has MM been measured and/or described in patients with SCD?
R2: What factors have been described in the literature that predispose patients with SCD to develop MM?
R3: What consequences or outcomes have been described as a result of patients with SCD developing MM?
This systematic review is based on the methodological framework of Arksey and O’Malley [32]. The approach was selected because MM in patients with SCD is an under-researched topic, and Arksey and O’Malley’s framework allows for maintenance of a broad scope for research questions. This allows researchers to be able to summarize the extent, range, and nature of activities related to the research question [32]. This review will include primary, quantitative, qualitative, and mixed methods peer-reviewed studies that meet the inclusion criteria. Studies had to focus on the patient with SCD and not on a HCP, caregiver, or family member. The studies were limited to only English language, data-based empirical research articles. Studies had to describe concepts found in the group-based MM instrument [24] [e.g., suspicion of the health care system (items 3, 4, 5, 6, 7, 9); group disparities in health care (items 8, 10, 11) and lack of support from health care (items 1, 2, 12)] [24]. Literature reviews, opinion texts, editorials, conference proceedings, dissertations, and studies about mistrust of research and genetic testing in SCD were excluded.
Article search strategies were developed in coordination with a research librarian specializing in systematic reviews. Using search terms “sickle cell anemia,” “sickle cell disease,” “trust,” “mistrust,” “distrust,” “stigma,” “racism,” “disparity,” “healthcare inequality,” “health disparities,” “physician-patient relations,” “nurse-patient relations,” “physician-patient communications,” and “discrimination” across six electronic databases (CINAHL, EMBASE, Scopus, PubMed, Psycinfo, and Web of Science) yielded 527 articles from 1994 to 2025. After removing duplicates, 402 articles remained. These titles and abstracts were then independently screened by three members of the systematic review team for relevance (MS, MF, NS), resulting in 321 remaining articles for full-text screening. During the full-test screening stage, two team members (MS, MF) independently conducted full-text screening of studies for fulfillment of the inclusion criteria.
Amongst the data-based articles that were ultimately selected for inclusion, two team members (MF, NS) screened their reference lists for potentially relevant articles based on titles, resulting in 38 new articles, added to the 321 full-text articles which needed full screening. Full-text screening of these 359 articles was conducted independently by two team members (MS, MF). Two reviewers (MS, MF) extracted relevant data using an Excel template designed for this review. The following information was collected: study settings, participant characteristics, objectives, any framework used, methodology, study design, recruitment, data collection methods, and findings specific to MM. The data extraction template was pre-tested on five eligible studies and refined. Themes, interpretations, and quotations were extracted from qualitative studies, while numbers and interpretations were extracted from quantitative findings. Both reviewers extracted relevant data, which was then double checked by the other reviewer (MS, MF). Any disagreement was resolved through discussion, and when required, by involving a third reviewer (RB). An iterative narrative synthesis approach to analysis was then conducted. The authors developed a synthesis of findings from included studies, explored relationships in the data, and discussed the emerging themes and concepts. These detailed findings from each article, including excerpts of patient statements, are listed in the in-text tables and in Table S1.
A final body of 42 original peer-reviewed articles was included in this systematic review. Figure 1 illustrates the flow of study screening and inclusion/exclusion. This systematic review was registered on Open Science Framework, maintained by the Center for Open Science (https://osf.io/).
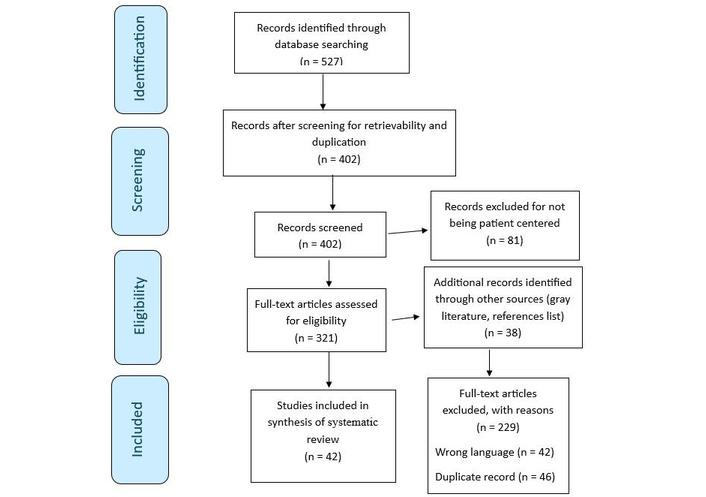
Literature search Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram and database search indicators. Adapted from “PRISMA” (http://www.prisma-statement.org/). Accessed July 1, 2025. © 2024–2026 the PRISMA Executive. Distributed under a Creative Commons CC BY 4.0 license.
Based on the systematic review framework [32], this review compiled study characteristics and findings on the topic of MM in patients with SCD. Table S1 provides a comprehensive presentation of the 42 included studies. Thirty-nine studies used cross-sectional designs, with only three studies utilizing a longitudinal design [33–35]. Five studies used strictly quantitative methodology, 26 studies were strictly qualitative, and eleven studies used mixed methods analyses. Table S1 also provides information on recruitment sites, a description of participants, frameworks, and tools utilized in each study, and a description of each study’s findings relevant to MM.
Overlap in recruitment strategies and settings was noted across studies. Four studies recruited from inpatient settings [36–39], 25 studies recruited from outpatient hematology clinics, and two studies recruited participants from the emergency department (ED) [40, 41]. Three studies recruited participants from market research company participant panels [42–44]. Ten studies recruited participants from community centers or national/local SCD advocacy foundations or groups, and two studies recruited participants from national SCD conferences [45, 46].
Seven of the 42 studies had higher male participant ratios than female participants [37, 44, 47–51]. Over half (n = 21) of the studies included older adult participants (above age 50 years old) with SCD, and only 13 studies examined pediatric patients (< 18 years of age) with SCD [34, 35, 38, 39, 42, 48, 49, 51–56]. Twenty-one (50%) studies specified the sickle cell genotype of participants, with the predominant form of sickle cell across these studies being hemoglobin SS. Notably, none of these studies differentiated their study findings or outcomes based on participant genotype.
Three studies included participants as dyads [42, 51, 52]. Nelson and Hackman [52] collected data on “patient and family” dyads with no further specification given as to the type of family member. Durgam and associates [42] collected data on adolescent patients and caregiver dyads, with no further specification about the caregiver. Lastly, Hauser and colleagues [51] provided specifics about dyads. All the dyads were adolescent and primary caretaker (17 parents, 4 grandparents, and 1 aunt) [51]. The only commonality discussed across the three articles was a description of the caregivers as being predominantly black and female [42, 51, 52].
Seventeen studies included participants with self-reported ethnicities that were non-Black or African American, with five of these studies reporting Hispanic participants [39, 48, 57–59], one study reporting an Asian participant [43], and three studies reporting White participants [43, 54, 59]. The remainder of the study participants self-identified as “other race” [39, 46–48, 51, 54, 58–60]. The majority of studies were conducted in the US, with eight studies conducted in England [34–37, 56, 61–63]. One study was conducted in Canada [42] and one in Brazil [47].
Research question 1: How has MM been measured and/or described in patients with SCD?
Only six articles used quantitative methodologies (Table 1). Sample sizes in these studies ranged from 20 to 556 participants [33, 39, 43, 52, 60, 64]. Only two quantitative studies [39, 52] included adolescents with SCD. None of these studies with quantitative methodology utilized a theoretical framework. No study utilized a psychometrically validated measure of MM, such as the GBMMS or the MMI or examined MM as either a discrete study variable or as a primary study aim. The instruments that were utilized included the Adult Sickle Cell Quality of Life Measurement Information System (ASCQ-ME) [65], the discrimination subscale of the interpersonal processes of care (IPC) survey [66], Perceptions of Racism in Children and Youth (PRaCY) Tool [67], the national Behavioral Risk Factor Surveillance System (BRFSS) dataset, and the Sickle Cell Transfer Questionnaire [68]. Table 1 summarizes the findings of studies that used quantitative methodologies. With the GBMMS [24] as a guide, most of these studies focused on the GBMMS sub-concept of group disparities in health care, i.e., discrimination based on race or drug seeking.
Quantitative study results.
| Author, year | Instrument used | Participants (n) | Study results |
|---|---|---|---|
| Rizio et al., 2020 [43] | Adult Sickle Cell Quality of Life Measurement Information System (ASCQ-ME), Work Productivity and Activity Impairment-Specific Health Problem (WPAI-SHP) | 303 | 101 patients reported that “difficulty trusting healthcare providers” and 120 patients reported that “discrimination or stigmatization by healthcare professionals” were barriers to receiving healthcare. |
| Evensen et al., 2016 [64] | ASCQ-ME: Quality of Care | 556 | Poor provider communication behaviors of not listening to patients, not spending enough time with patients, and not treating them with respect (60% of participants).Emergency department (ED) nurses and doctors did not believe their pain scores.Experiences of being treated badly in the ED by healthcare staff contributed to current decisions to delay seeking care during acute vaso-occlusive pain crises (83% of participants). |
| Mathur et al., 2016 [60] | Discrimination subscale of interpersonal processes of care (IPC) survey | 71 | 38% (n = 27) reported some experience with discrimination in health settings; of these 27 individuals, 21 reported doctors paid less attention to them due to race; 22 reported they felt discriminated against by doctors because of race or ethnicity. |
| McGill et al., 2023 [33] | Discrimination subscale of IPC survey2-item subscale:“How often did doctors pay less attention to you because of your race or ethnicity?”“How often did you feel discriminated against by doctors because of your race or ethnicity?” | 68 | Racism-based discrimination negatively impacted pain scores (average daily pain score, baseline pain score) with statistical significance.Racism-based discrimination also significantly negatively impacted depression and severity of insomnia in patients. |
| Wakefield et al., 2017 [39] | Perceptions of Racism in Children and Youth (PRaCY) measure | 20 | Four youth with sickle cell disease (SCD) reported incidents of racial bias in medical settings. |
| Nelson and Hackman, 2013 [52] | Behavioral Risk Factor Surveillance System (BRFSS) 2008 and Sickle Cell Transfer Questionnaire | 112 | 50% of patients and families felt that race affected the quality of health care, with equal distribution between outpatient and inpatient settings. |
Thirty-six articles employed qualitative methodologies (eleven of which utilized mixed methods). Sample sizes in these qualitative studies ranged from seven to 95 participants. Fourteen studies explicitly described the use of a qualitative framework, theory or design. The qualitative frameworks/theories utilized included hermeneutics [69], phenomenonology [55, 56, 59, 61], van Manen’s Thematic analysis [69], ethnography [70], The Sociological Theory of Stigma [47], grounded theory [34, 35, 71], Ecological Framework for Palliative Care of SCD [72], Leininger Culture Care Theory [72], critical race theory [59], Theory of Self Care Management for SCD [40], and a new paradigm research design from Reason & Rowan 1981 and Webb’s 1991 feminist methodology [36]. Table 2 summarizes the findings of the qualitative studies.
Summary of qualitative predictors of medical mistrust.
| Theme | Description | Sample quote | Contributing studies |
|---|---|---|---|
| Healthcare providers (HCPs) mistrust and stigmatize the patients | When HCPs mistrust patients and display that mistrust, patients develop mistrust of providers.This mistrust includes being labeled a “drug addict” being judged by nurses and even hospital security staff. | “They get suspicious because they can’t believe you can be better in two days”The nurse turned around to me and said, “…we’re scared that you’re gonna get hooked on it and we don’t wanna see you down on the street hustling drugs”“They think we’re like two-hour junkies you know, as soon as the time is up, we want a fix”“There was a nurse who told me sickle cell was not a disease”“They’ll say, well you don’t look like you have sickle cell. How am I supposed to look?” | Alleyne et al., 1994 [36]Masese et al., 2021 [49]Ezenwa et al., 2016 [57]Williams-Gray and Senreich, 2015 [59]Maxwell et al., 1999 [63]Wickersham et al., 2022 [72] |
| Lack of emergency department (ED) physician knowledge about sickle cell disease (SCD) | Patient believes that ED physicians either do not know what sickle cell is, or do not fully understand it, leading to patients not being treated correctly in the ED. | “ED doctors should consult the SCD team but they do not, because I am a doctor and I know how to treat you”“My (hematology) doctor wrote that protocol…of course they (ED physicians) are not familiar with the dosage you’re on, things of that sort…there are specific protocols but they’ll ignore it”“Every time I enter the ED, I wonder if it will be the last time. Will they take my life seriously?”“One doctor asked me (about sickle cell), ‘wait what is that exactly?’” | Collins et al., 2022 [34]Young et al., 2020 [44]Sinha et al., 2019 [45]Crego et al., 2021 [48]Campbell et al., 2010 [55]Wickersham et al., 2022 [72] |
| Inadequate pain control during a pain crisis | HCPs (doctors and nurses) dismiss patients’ self-reported pain levels, making assumptions about their pain level, thus downrating their pain score and providing inadequate analgesia, and forcing patients to wait a long time for pain medication. | “They make us wait a long time for pain medicine”“I was screaming for painkillers and the nurse said I was pretending”“The nurse decided to cut down the dose without the doctor’s permission. When I saw the chart, I saw she was giving half the dose”“Pain is what the patient says it is, unless you have sickle cell, then it’s what the doctor says it is” | Collins et al., 2022 [34]Durgam et al., 2023 [42]Coleman et al., 2016 [61]Elander et al., 2004 [62]Maxwell et al., 1999 [63]Wickersham et al., 2022 [72] |
| Patient believes that HCPs racial biases impact treatment and care | Patients’ perception that HCPs harbor racially-motivated, implicit biases that impact their treatment. | “A white patient wouldn’t be treated like this”“Racial bias impacts how fast you get treatment”“This doctor saw everybody else, all the white people, before he saw me”“My race does influence my experience with SCD because blacks are viewed in a negative light”“My experience with sickle cell has been that I don’t want to go to a hospital. I think they’re insulting. I think that because of my skin color, they think I’m an idiot. I think it’s racism; pure simple racism” | Wakefield et al., 2018 [38]Durgam et al., 2023 [42]Carvalho et al., 2021 [47]Treadwell et al., 2020 [54]Wickersham et al., 2022 [72]Cole et al., 2007 [76] |
| Poor transition of care from pediatric specialty care to adult medical care | Patient descriptions of the negative aspects during the transition of care in the emerging adulthood period. | “Even though I’m 24…I’m still with my pediatric hematologist because she does sickle cell and sickle cell only. She doesn’t want me going to a hematologist and oncologist who does both”“I worry that I will have a doctor that doesn’t know SCD. Some doctors don’t know how to treat SCD and they act like they do” | Hauser et al., 1999 [51]Phillips et al., 2022 [53]Treadwell et al., 2020 [54]Williams-Gray and Senreich, 2015 [59]Wickersham et al., 2022 [72]Bemrich-Stolz et al., 2015 [74] |
| Characteristics of HCPs that lead to development of medical mistrust | HCPs displaying ableism and phobia of giving opioids.Provider bias about disability.Differences in prescribing pain meds.Racial cultural stereotypes. | “Participants suspected that the ED staff were reserving hydromorphone for patients without SCD. For example, ED staff advised they did not have hydromorphone; however, when the patient was hospitalized, hydromorphone was available”“Because so many people go to the ER, they do your labs, and if there’s hemoglobin like [mine] used to be an eight or so. And that’s like, ‘Oh, yeah. Hemoglobin is at eight. You can’t possibly be in a crisis.’ I go to (place) every six weeks to get the transfusions, so of course, my hemoglobin’s gonna be high: That doesn’t mean I’m not in a crisis...” | Collins et al., 2022 [34]Renedo et al., 2019 [35]Alleyne et al., 1994 [36]Durgam et al., 2023 [42]Sinha et al., 2019 [45]Carvalho et al., 2021 [47]Crego et al., 2021 [48]Masese et al., 2021 [49]Campbell et al., 2010 [55]Royal et al., 2011 [58]Williams-Gray and Senreich, 2015 [59]Maxwell et al., 1999 [63]Adegbola et al., 2012 [69]Weisberg et al., 2013 [71]Bemrich-Stolz et al., 2015 [74]Brown et al., 2015 [75]Cole et al., 2007 [76] |
| Adolescent specific predictors of medical mistrust | Adolescent patient descriptors of what makes them mistrust HCPs—being excluded from shared decision making and fear of transitioning to adult care. | “When you’re a pediatric sickle cell patient, you have the doctors there every step of the way, but not with adult sickle cell…I know when I first transitioned I never felt more alone in my life. And adult care providers are a lot more blunt and cold, like ‘I don’t know, I’m not really educated in sickle cell.’” | Collins et al., 2022 [34]Renedo et al., 2019 [35]Wakefield et al., 2018 [38]Durgam et al., 2023 [42]Crego et al., 2021 [48]Masese et al., 2021 [49]Hauser et al., 1999 [51]Phillips et al., 2022 [53]Treadwell et al., 2020 [54]Campbell et al., 2010 [55]Thomas et al., 2002 [56] |
Most studies utilizing qualitative methodologies employed a semi-structured interview guide that was administered individually, with eight studies administering focus groups [44, 49, 51, 56, 59, 63, 70, 73]. One study utilized an open-ended, fill-in-the-blank written section for qualitative data collection [57], and one study had participants use digital technology, specifically the Photovoice program to provide qualitative data [44]. Further description of these studies can be found in Table S1.
Research question 2: What factors have been described in the literature that predispose patients with SCD to develop MM?
To answer research question 2, themes were extracted from the 42 studies that met inclusion criteria to predict the development of MM in patients with SCD by two authors (MS, MF). The aggregated themes included HCP/staff behaviors and characteristics, inadequate pain control, poor transition of care from pediatric to adult medical care, lack of HCP transparency about medical treatments, and adolescents’ specific predictors of MM. Table 2 summarizes the predictors of MM with illustrative quotes.
The first theme of MM predictors was related to HCP-specific behaviors and characteristics. Many of the qualitative studies in this review examined patients’ experiences of being mistrusted by hospital staff and HCPs in EDs and acute care hospitals. Many examples of healthcare professionals, namely physicians and nurses, mistrusting the patient and his/her intentions were described as voiced concerns and behaviors by HCPs, with these HCP behaviors directly leading to the patient mistrusting the physicians and nurses in turn.
Specific to physicians, a common finding across studies was the patients’ perception of non-hematology physicians being opioid-phobic regarding prescribing opioids for their pain in both inpatient and outpatient settings. Non-SCD specialty providers, ranging from ED physicians and PCPs, were commonly reported as ignoring patients’ standing pain treatment protocols. This behavior, combined with a lack of interdisciplinary care coordination and refusal to consult their hematologist during a pain crisis, led to the development of MM of ED and PCP providers among patients with SCD.
Almost all of the studies examining patients’ perception of non-hematology physicians reported the patients’ predominant belief that these physicians lacked any knowledge of SCD. The patients described themselves as not trusting these physicians (e.g., ED and PCP) for their care.
Many studies reported qualitative findings about patients feeling stigmatized by HCPs who labeled them as “drug addicts”. Patients reported the belief that even asking for pain medication during an acute pain crisis could lead to the development of HCPs’ mistrust or stigmatization of a patient with SCD. Another common finding across studies was patients’ perception of HCPs endorsing racial bias and discrimination by dismissing them, discounting their concerns, and delaying their care [34–36, 39, 42, 45, 47–49, 52, 55, 58–60, 69, 71, 74–77].
One major predictor of the development of MM in patients with SCD was poor pain management during a crisis. The poor pain management was described as 1) long wait times to receive pain medicine, 2) receipt of inadequate doses of analgesia and being told to wait hours for another dose, and 3) being ignored by HCPs when asking directly for pain medicine. Another common theme related to pain control was the belief that HCPs were intentionally withholding pain medicine [34, 36, 42, 61–63, 69, 70, 72].
Among studies that examined both adults and adolescents with SCD, the transition of care from pediatric hematology sites to adult hematology sites led to patients developing mistrust of their new adult HCP. The participants described adult medicine providers labeling them as drug-seeking. The patients described providers who were not hematologists specialized in sickle cell care, but rather they were taking care of a variety of hematological disorders without specializing in SCD. The patients also perceived that adult providers were less compassionate, respectful, and supportive of their needs than their pediatric providers, and they feared being transitioned to someone with limited knowledge of SCD [51, 53, 54, 59, 71, 72, 74].
Another theme was the patients’ concern about the side effects of medications and HCPs’ lack of transparency about the side effects. Another related finding was patients reporting mistrust of HCPs due to limited transparency about the full scope of treatment options or pushing specific treatment options despite the patients’ refusal. Patients also reported a belief that HCPs may not be clinically up to date about all the available treatment options [46, 49, 78]. Another expressed theme was a system level inability to find specialized care or knowledge sickle cell providers. Patients often lacked the option to choose a SCD provider they liked, and they had to accept care from whoever was available. In many locations, no SCD provider or clinic existed [41, 43, 51, 53].
Common themes across the adolescent-focused studies were perceptions of feeling invisible and excluded from the shared decision-making process. Adolescents reported their frustration with HCPs speaking only to caregivers, which led to mistrustful feelings. Similar to the adult participants/patients, adolescents feared the transition from pediatric to adult healthcare. These fears were also based on concerns about being treated incorrectly due to the HCPs’ lack of knowledge about SCD [34, 35, 38, 39, 42, 48, 49, 52–56].
Research question 3: What consequences or outcomes have been described as a result of patients with SCD developing MM?
To answer research question 3, four common themes about the consequences or outcomes of the development of MM in patients with SCD were extracted from the 42 included studies. These themes included: 1) impact on patient behaviors, 2) impact on treatment adherence, 3) impact on patient psychological outcomes, and 4) the development of maladaptive coping strategies. Table 3 represents the outcomes and consequences of patients with SCD developing MM, with illustrative quotes.
Summary of consequences/outcomes of medical mistrust development.
| Theme | Description | Sample quote | Contributing studies |
|---|---|---|---|
| Impact on patient medication and treatment plan adherence | Concerns about medication side effectsConcern that providers are not being transparent about medications and all treatmentsConcern about the persistence of doctors in trying to prescribe certain therapies hydroxyurea (HU) | “HCPs are not up to date on the latest treatments”“I’m pretty much like, why is she still talking about this? I tell her no every time, will she give up? But she doesn’t. She asks me every time”“I wasn’t interested in taking more drugs and a drug (HU) with toxic effects”“my nurse had on gloves and I asked why she has on gloves and she said that HU is chemotherapy, to which I thought, I’m on chemo?” | Sinha et al., 2018 [46]Masese et al., 2021 [49]Weisberg et al., 2013 [71]Jabour et al., 2019 [77] |
| Impact on patient psychological outcomes | Fear of being given poor or inadequate treatmentAngerFatalismAnxietyHelplessnessFrustration: about lack of care options, about being dismissed, about being stereotypedBeing made to feel invisibleDevelopment of medical trauma | “You see, our society accepts and treats cancer patients differently. They can’t see that sickle cell disease is something you’re born with. I’d say their pain is less than ours. However, they get better treatment, better pain management than sickle cell patients”“It bothers me quite a bit because I’m not getting the treatment that I need because of fear of giving a sickle cell patient drugs that are addicting”“There is no SCD clinic in my hometown, and limited (care) options because of Medicaid”“When you (health care providers) look at me and say that I am an addict for getting a medicine that is going to make me feel better in a disease I have no control over whatsoever, then I know right then and there you are categorizing me. You are looking down on me. You have nothing good to think about me. So, it makes me very angry. It really does”“... it makes me feel like, you know, my life is worth nothing to them. You could drop down dead, they wouldn’t care you know, another bed for somebody else”“I was stressed and thinking of killing myself” | Collins et al., 2022 [34]Harris et al., 1998 [37]Smith et al., 2017 [41]Oyedeji et al., 2025 [50]Hauser et al., 1999 [51]Phillips et al., 2022 [53]Campbell et al., 2010 [55]Thomas et al., 2002 [56]Elander et al., 2004 [62]Strickland et al., 2001 [73] |
| Impact on patient behaviors | Avoidance of care or care siteDelaying care (waiting to go to emergency room)Changing their appearance to be taken seriously and not be labeled a “drug addict” | “I try to avoid the ED as much as possible”“I don’t like going to the ED…they act like I’m a junkie or something because I ask for pain medication”“Even now when I go back to the hospital, I don’t fully trust them. I try to avoid the hospital as much as I can”“When you have sickle cell disease, you have to look a certain way...if you look shabby then you’re a drug user”“This nurse is very insensitive; she has insulted me on several occasions and made me cry. This has caused unnecessary stress during my crisis [...] (this has made me feel) [...] uncomfortable [...] I no longer use the center” | Collins et al., 2022 [34]Young et al., 2020 [44]Sinha et al., 2018 [46]Masese et al., 2021 [49]Treadwell et al., 2020 [54]Maxwell et al., 1999 [63]Weisberg et al., 2013 [71]Jabour et al., 2019 [77]Matthie et al., 2016 [78] |
| Maladaptive coping strategies | Patient description of maladaptive coping strategies to deal with inadequate care from healthcare providers: managing pain on their ownTurning to illicit substance use as copingNondisclosure habit to providersSelf-discharge from inpatient stays | “I was convinced that the nurse was trying to kill me. I was in a great deal of pain and discharged myself, phoned up my friend to come and get me”“They gave me some tablets every 3 or 4 hours. It doesn’t work like that. So I asked her in the next bed (another SCD patient) if she had something to spare. She brought some tablets from home” | Sinha et al., 2019 [45]Elander et al., 2004 [62]Maxwell et al., 1999 [63]Wickersham et al., 2022 [72] |
A dominant theme across studies was the avoidance of non-specialty (non-hematology) care. One non-specialty area that was commonly discussed was the avoidance of EDs [34, 41, 42, 44, 54, 78]. Patients described managing their pain during an acute sickling crisis to avoid going to the ED until the pain became unbearable. Patients described wanting to control the pain crises for as long as they could at home and hoping that the pain would resolve on its own to avoid being undertreated for pain, judged for wanting pain medication, and racially profiled [34, 44]. Another subtheme related to avoidance of non-specialty care was the avoidance of PCPs because of their lack of SCD knowledge and instead utilizing their hematologist as their PCP [35, 49, 51, 75].
Another outcome health behavior discussed was patients’ practice of changing their external appearance to appear cleaner and neater so that they would not be treated like a “drug addict” for looking “shabby,” despite their level of pain [42, 44]. A common behavior described by patients was avoiding the display of their personal pain coping strategies (such as singing, listening to music, laughing) in view of HCPs to control the HCPs’ perception about their subjective pain score and thereby receiving inadequate analgesia [34, 56, 62].
The lack of provider transparency about treatment plans and options, as well as side effects of medications, was described as leading to patients mistrusting the treatments and negatively impacting treatment adherence. One specific outcome commonly described was the decreased adherence to medications, specifically to hydroxyurea (HU) [34, 44, 46, 49, 54, 63, 71, 72, 77, 78]. Studies described participants’ skepticism about efficacy of HU and concerns about its side effects despite HCPs’ attempts to allay their concerns. Some participants even described how daily HU use and frequent routine blood transfusions [72] kept their hemoglobin high, with the consequence that the normal hemoglobin level led to ED providers mistrusting them during crisis visits and dismissing them. As a result, patients report not receiving pain medication in the ED, and being told, “oh your hemoglobin is fine, you can’t possibly be in a crisis.” [72].
One finding was the impact of poor pain control and racism-based discrimination from HCPs on patients’ quality of life and psychological well-being. One quantitative study [33] and one mixed methods study [60] reported that perceptions of racism-based discrimination significantly negatively impacted pain scores, and led to elevated depression, anxiety, and insomnia scores. Several studies utilizing qualitative methodology also reported poor psychological well-being as an outcome in patients reporting MM, as well as the development of fear, anxiety, frustration, anger, helplessness, loss of self-esteem, and fatalism [34, 37, 41, 50, 51, 53, 56, 69, 73]. Another psychological outcome described in qualitative studies [76] was the development of medical trauma due to pain medication being withheld, dosed incorrectly, or being made to wait for pain medication [76].
Across studies, a common finding was the discussion of the development of maladaptive coping strategies to seek a sense of control due to being left in uncontrolled pain. Participants described illicit substance use (e.g., marijuana) as a way of managing pain in a “non-opioid” manner. In contrast, others described the use of non-prescribed opioids in both inpatient and outpatient settings to manage the pain. Commonly, participants expressed a desire to learn about alternative pain medication strategies so pain could be managed on their own, in their own home, and to avoid hospital utilization [45, 62, 63]. Another form of maladaptive coping in order to maintain a sense of control was the practice of nondisclosure to medical providers [72]; this strategy was common after being made to feel helpless or like a “drug addict” during medical care. Another maladaptive coping mechanism was the recurring discussion of self-discharging from inpatient settings when care was perceived to be poor quality, racist, or harmful [58]. Figure 2 conceptualizes the findings of this review, and depicts the predictors and outcomes of MM development in patients with SCD.
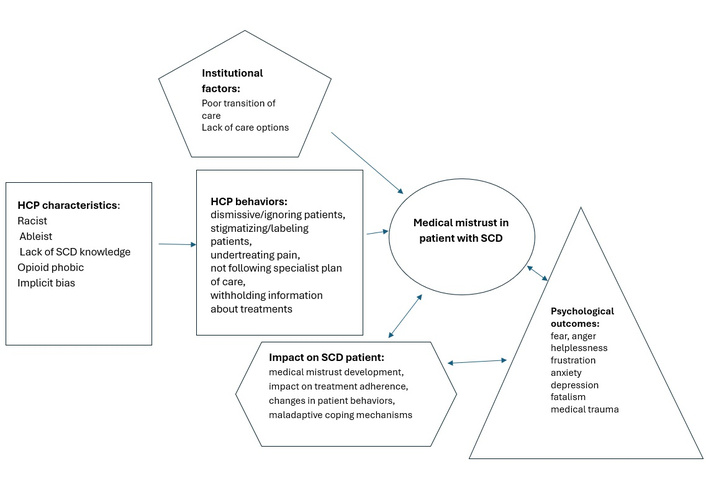
Conceptualization of medical mistrust development in patients with sickle cell disease (SCD). HCP: healthcare provider.
This systematic review surveyed the extant literature on MM in patients with SCD. Study characteristics and findings were compiled to present the overall results of the review and the types of research conducted to date. The predictors of MM centered around HCP characteristics, HCP specific behaviors, and institutional factors. The outcomes of the development of MM in patients with SCD included patient behaviors negative psychological conditions, negative impacts on treatment plan adherence, development of medical trauma, and the development of maladaptive coping mechanisms. Overall, the review summarized the linkage of the predictors and the resultant outcomes of MM.
Most surprisingly, with a genetic disease found almost exclusively in populations of persons of color, this review found significant deficits in the measurement and evaluation of race-based MM. There were no studies that explicitly examined (quantitatively or qualitatively) MM as a primary study aim, predictor, or outcome. In addition, despite the availability of two psychometrically validated and widely used MM scales (e.g., GBMMS or the MMI) [23, 24], none of the quantitative studies measured MM utilizing either of these scales in their analyses. Furthermore, there were no quantitative associations measured between MM and SCD-specific health outcomes despite the multitude of chronic illness studies reporting an association between MM and health outcomes [24, 79–83]. These findings represent opportunities for future research using valid and reliable MM measures to capture quantifiable data specific to sickle cell health outcomes of interest.
Even though the racial and ethnic makeup of people with SCD in the US is primarily African American [52], only 17 of the 42 studies reported the ethnicities of patients with SCD as either non-Black or non-African American. Similarly, the location of most studies in the review was limited to US, with only a few from non-US countries, Europe, Canada, and South America. As the paradigm of race has a very unique history and a myriad of sociopolitical implications in US [84–86], it can be assumed that race may not play the same role in the development of MM in other countries, especially in ethnically homogenous nations where patient-provider racial discordance does not occur. Future studies that examine MM with a non-racial lens in patients with SCD of other ethnicities and in other countries may provide a more comprehensive picture of this phenomenon. Additionally, future studies conducted in US should also take into consideration the nuances of group-based MM across different geographical regions of US, as perspectives about racial/ethnic minorities vary widely.
All but one quantitative study [33] and two qualitative studies [34, 35] employed cross-sectional study designs. Given that individuals with SCD have frequent interaction with the health care system, it is imperative that future studies examine the longitudinal and dynamic nature of MM across the SCD continuum. The importance of examining how the developmental stages of adolescence and emerging adulthood impact the development of MM requires significant attention. Although few studies have examined MM in this population [87–89], early research suggests that MM can be intergenerationally transmitted [90]; therefore, its development likely begins much before adulthood [16, 17]. Future studies should include an assessment of the impact of intergenerational MM among sickle cell patients and their caregivers/family members. While patient-caregiver dyads were studied across three studies in this review [42, 51, 52], this potential contributor to MM development was not explicitly studied as a predictor in these studies. Also, as disease self-management increases with chronological age and as these adolescents with SCD approach the transition to care from pediatric hematology to adult hematology, it is critical to understand how MM in adolescents with SCD impacts the transition process.
Another key aspect to examine is the influence of gender on the phenomenon of MM in patients with SCD. Most studies had predominantly female participants; it is imperative to examine the male perspective since the literature on MM has found differences by gender [91]. Furthermore, only a handful of studies recruited patients while they were inpatients. The contribution of inpatient admission, while the patient is acutely in a sickling crisis, to the development of MM deserves targeted attention. A comparison of inpatient versus outpatient predictors of MM may provide insight into tailored interventions by care setting.
Qualitative studies examining MM in patients with SCD should provide a more nuanced investigation across the lifespan and across the genotypes of SCD. Studies should explicitly investigate patient-identified suggestions to mitigate MM in this population. While qualitative studies are more likely (than quantitative studies) to use a theoretical framework [92], future qualitative studies examining MM in patients with SCD would benefit basing their studies on theories, utilizing structured study designs, and creative use of data collection processes. The use of technology, such as Photovoice [93], should be explored to enhance day-to-day narratives and a more comprehensive understanding of MM in this population.
Future quantitative studies need larger sample sizes, operationalized empirical predictors of MM in this population, and need to examine MM as a mediator using more advanced statistical methodologies. Benkert and colleagues [17] argue that MM is not solely a psychological outcome of the healthcare system, but also behaves as a mediator between the system and patient health outcomes, such as medication adherence and healthcare utilization patterns. Future studies should also stratify results related to MM by age, gender, and type of SCD. Specifically, future quantitative studies should examine the relationship between MM and healthcare utilization, HU medication adherence, or mistrust toward blood transfusions, which are frequent and lifelong components of sickle cell medical care.
Strengths of this systematic review include a thorough review of the perspectives of MM in patients with SCD as informed by an extensive literature search. The searches were conducted with the support of an experienced librarian. To avoid selection bias, there were three researchers involved in the article selection process. The review also identified specific HCP behaviors that contribute to the development of MM. One unique aspect was the HCPs’ outward display of mistrust towards patients, which then led to development of mistrust within patients. Similar to Benkert and colleagues’ findings [17], this review found that anxiety and depression were described as psychological outcomes of MM. A new finding of this review is the identification of medical trauma and medical fatalism as outcomes of MM in patients with SCD. These outcomes need to be rigorously investigated and measured in future SCD studies.
This review had limitations as well. First, by design, the review excluded studies that focused on the perspectives of caregivers, family members, and friends of patients with SCD. However, caregivers and family are an important aspect of MM development, particularly the intergenerational component of MM [16, 17]. The development of MM in patients with SCD could be influenced by family members who also have SCD and/or negative health care experiences. This review also excluded studies that examined mistrust of medical research and/or blood transfusions in patients with SCD. As important aspects of a sickle cell medical plan of care, these two foci need further study.
Another limitation was the lack of availability of descriptors among studies of “preventive management techniques” used by patients to prevent a sickling crisis and subsequent healthcare utilization. Although avoidance was a result identified in several studies, clear descriptions by patients were not provided regarding exact management strategies utilized to avoid hospitalization or emergency room (ER) visits. This remains an area that requires further probing in future studies to elicit as a potential healthcare behavior whose onset is induced by MM in patients with SCD. Another limitation of the review was that most of the included studies recruited patients who were already affiliated with regular clinical care. Consequently, the results of this review may not represent the views of those patients with SCD who have low healthcare utilization. The results may not represent the views of those with other genotypes of SCD (such as thalassemic variants) that have fewer crises, have less intensive medical plans of care, and thus have fewer encounters with the health care system.
Despite these limitations, the review highlights the precursors of MM as well as the medical and psychological outcomes in patients with SCD. The paucity of extant literature on this topic emphasizes the need for more rigorous and larger-scale studies in the sickle cell population to establish more conclusive linkages between MM and health outcomes. Furthermore, HCPs such as emergency physicians and nurses, PCPs, and adult hematology providers can utilize these findings to identify modifiable characteristics and behaviors that contribute to the development of MM in their patients with SCD. By doing so, MM onset can be prevented, delayed, or even reversed in this population, and can ultimately cease to be a barrier to medical care.
In conclusion, this systematic review provides a solid basis for further detailed investigation into the concept of MM in patients with SCD. More studies are needed using various methodologies, frameworks, and theories to further elucidate this concept. The qualitative predictors of race-based MM presented in this systematic review may help inform clinicians to improve care delivery. A foundation for comprehensive interventions can be developed from the findings to decrease MM and improve health behaviors in patients with SCD. The authors urge other researchers to use the findings to develop more in-depth studies focused on the predictors, development and consequences of MM in patients with SCD.
ED: emergency department
GBMMS: Group-Based Medical Mistrust Scale
HCPs: healthcare providers
HU: hydroxyurea
MM: medical mistrust
MMI: Medical Mistrust Index
PCP: primary care physician
RBC: red blood cell
SCD: sickle cell disease
The supplementary table for this article is available at: https://www.explorationpub.com/uploads/Article/file/1001400_sup_1.pdf.
We would like to thank the information specialist Dr. Elizabeth Jenuwine at Wayne State University for assistance in the literature search.
MS: Conceptualization, Methodology, Data curation, Formal analysis, Writing—original draft, Writing—review & editing. MF: Conceptualization, Methodology, Data curation, Formal analysis, Writing—review & editing. JB: Writing—original draft, Writing—review & editing. NS: Methodology, Writing—review & editing. AW: Writing—review & editing. AKG: Conceptualization, Writing—review & editing. RB: Conceptualization, Writing—review & editing, Supervision. All authors read and approved the submitted version.
The authors declare no conflicts of interest in the design, collection/analyses/interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Not applicable.
Not applicable.
Not applicable.
The available data is included in Table S1. Other data used in this study are available upon request from the corresponding author.
No funding was utilized in the development of this manuscript.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 872
Download: 20
Times Cited: 0
