Review
Review

Affiliation:
1Managed Care Department, New York Health and Hospitals Corporation, New York, NY 10041, USA
Email: led1@nychhc.org
ORCID: https://orcid.org/0009-0007-9191-3006
Affiliation:
2Barts and The London School of Medicine and Dentistry, Queen Mary University of London, E1 2AD London, UK
Email: tuan.pham@qmul.ac.uk
ORCID: https://orcid.org/0000-0002-4255-5130
Explor Med. 2025;6:1001371 DOI: https://doi.org/10.37349/emed.2025.1001371
Received: August 05, 2025 Accepted: October 19, 2025 Published: November 19, 2025
Academic Editor: Amedeo Lonardo, Retired, Azienda Ospedaliero-Universitaria di Modena (–2023), Italy
Colorectal cancer (CRC) remains a significant global health challenge due to its high incidence and mortality, underscoring the need for early detection and precise diagnosis to improve survival outcomes. Recent advances in artificial intelligence (AI), particularly deep learning and machine learning (ML), have revolutionized medical imaging and reshaped CRC screening, diagnosis, and prognosis. AI algorithms demonstrate strong performance in analyzing computed tomography, magnetic resonance imaging, and endoscopic images, achieving superior sensitivity, specificity, and efficiency in detecting and characterizing colorectal lesions. These developments enhance lesion identification, risk stratification, and treatment planning, advancing the broader goal of precision medicine. Importantly, AI has the potential to reduce health disparities by extending access to high-quality diagnostic capabilities in low-resource regions where shortages of expert radiologists delay detection. Despite these advantages, implementation in clinical practice remains limited by several challenges, including data bias, lack of population diversity in training datasets, limited generalizability, operator dependency, and integration difficulties within existing workflows. Moreover, ethical and economic considerations—such as algorithm transparency, data privacy, and cost-effectiveness—continue to shape adoption. This review synthesizes current evidence on AI applications in CRC imaging, emphasizing methodological progress, clinical performance, and translational challenges. It also evaluates the readiness of AI systems for real-world use, highlighting ongoing needs for validation, regulatory oversight, and interdisciplinary collaboration. Ultimately, AI holds transformative potential to enhance CRC detection and management, improve diagnostic accuracy, and promote equitable access to advanced screening worldwide, provided that technological, ethical, and implementation barriers are effectively addressed.
Cancer is the second leading cause of death in the United States after heart disease, responsible for one in five deaths nationwide. In 2025, approximately 2,041,910 new cancer cases and 618,120 cancer-related deaths are projected, corresponding to an incidence rate of 445.8 per 100,000 and a mortality rate of 145.4 per 100,000 individuals [1, 2]. These figures underscore the ongoing need for effective prevention, early detection, and treatment strategies. Colorectal cancer (CRC), in particular, imposes a significant burden, with U.S. healthcare costs reaching $24.3 billion in 2022—second only to breast cancer [3, 4]. More broadly, cancer-related expenditures in the U.S. were projected to rise to $208.9 billion by 2020, largely due to population aging and expanding care needs [5–7].
Globally, CRC incidence is expected to rise sharply. By 2030, new cases are projected to exceed 2.2 million, with over 1.1 million annual deaths. By 2040, these numbers may climb to 3.2 million new cases and 1.6 million deaths. Most of this increase will occur in countries with high or very high Human Development Index (HDI) rankings, reflecting aging populations and lifestyle-related risk factors such as diet and sedentary behavior [8]. Significant variation exists in CRC incidence and mortality worldwide, strongly influenced by healthcare access and development level [9]. Global analyses reveal a tenfold disparity in CRC rates, with low- and middle-income countries (LMICs) experiencing accelerating incidence compared to high-income nations, where rates have plateaued or declined due to widespread screening and advanced therapies [9, 10]. In LMICs, limited access to timely diagnosis and care results in later-stage presentation, higher mortality, and substantial out-of-pocket costs that often drive families into poverty. For instance, CRC ranked as the second leading cause of cancer-related death in Europe in 2015, with annual costs estimated at €19.1 billion, including indirect costs from lost productivity [11]. These financial burdens are even more acute in LMICs due to systemic infrastructure limitations.
Understanding CRC’s global impact requires comparative insights into its epidemiology and economic consequences, particularly in LMICs where incidence is rising due to urbanization, aging populations, and shifting lifestyles [8]. These trends highlight the urgent need for accessible, cost-effective interventions. Innovations such as artificial intelligence (AI) offer potential solutions, enabling scalable diagnostic tools that could improve timely CRC detection in low-resource settings. This review presents a synthesis of recent CRC incidence and mortality data, with a focus on AI-driven strategies that may reduce disparities through enhanced prevention, early detection, and treatment. Special attention is given to the implications for LMICs, where novel approaches are essential to improve equity and advance sustainable global cancer care.
CRC is the third most commonly diagnosed cancer worldwide and the second leading cause of cancer death in the United States [12–17]. In 2025, an estimated 107,320 colon and 46,950 rectal cancer cases will occur in the U.S. [17]. Globally, 20 million new cancer cases and 9.7 million deaths were reported in 2022, with projections reaching 35 million cases by 2050 due to population growth alone [13, 14].
In the U.S., CRC accounted for 51,869 deaths in 2020, with an age-adjusted mortality rate of 12.6 per 100,000 [18]. Lifetime risk is 4.4% in men and 3.9% in women, with respective mortality risks of 1.6% and 1.5% [18, 19]. SEER data show that incidence peaked in the 1980s, while mortality has declined steadily since 1984, accelerating post-2000 [20, 21]. From 2011–2019, incidence declined about 1% annually in individuals ≥ 65 but increased 1–2% per year in those < 55, representing a 51% rise in early-onset CRC (EOCRC) since 1994 [22, 23]. Adults aged 50–54 now have rates comparable to those aged 55–59, and underserved groups—including Alaska Native, American Indian, and Black populations—bear disproportionate burdens [24, 25].
Men consistently exhibit higher CRC incidence and mortality than women (35.3–52.3 vs. 25.0–45.1 per 100,000) across all racial groups [19]. While most cases occur in individuals ≥ 55, approximately 15% affect those aged 45–54, with incidence peaking between 65–74 years [19, 23, 26]. Rising incidence in adults 40–54 has been linked to poor diet, obesity, inactivity, inflammation, microbiome changes, and possible environmental or epigenetic factors [27, 28].
The global incidence of EOCRC—defined as CRC diagnosed before age 50—is rising sharply, particularly among women and racial/ethnic minorities, driven by strong birth cohort effects projected to persist through 2040 [29–32]. From 1990 to 2021, incidence increased from 5.4 to 6.1 per 100,000 (AAPC = 0.39), with the steepest annual rises in individuals aged 20–29 (7.9%), 30–39 (4.9%), and 40–49 (1.6%) [30, 32]. In Norway, EOCRC rose by 66% from 1993 to 2022, and global projections estimate an increase of roughly 5.4% by 2030 [30, 32].
EOCRC is frequently diagnosed at advanced stages due to delayed symptom recognition. Common symptoms—rectal bleeding, anemia, weight loss, and abdominal pain—are often overlooked, leading to diagnostic delays of 4–6 months [33]. These delays are more pronounced in high-risk populations, including Native Hawaiian, Pacific Islander, Black, and Hispanic individuals, who face elevated incidence and mortality due to systemic inequities [29].
Studying EOCRC on a global scale remains difficult due to inconsistent disease classification, fragmented data systems, limited international collaboration, and disparities in healthcare access. Cultural and structural barriers—including poverty, stigma, fatalism, and uneven screening availability—further impede prevention and timely diagnosis [34–36].
Despite ongoing challenges, growing awareness, international collaboration, and advances in data science are enabling global progress in EOCRC prevention. Recent initiatives support risk prediction modeling, early detection, and public health campaigns via traditional and digital platforms. The 2025 Global Early-Onset Colorectal Cancer Think Tank (GEOCRCTT) convened stakeholders from 23 countries to establish coordinated strategies, following a 2024 workshop series by Fight CRC aimed at advancing risk stratification and international research efforts (Fight CRC 2024; GEOCRCTT 2025). ML models using real-world electronic health record data show promise for EOCRC risk prediction, even among individuals below traditional screening age [37].
The rising burden of EOCRC—marked by increasing incidence, delayed diagnosis, and distinct molecular features—underscores the urgency of implementing equitable, risk-adapted screening and prevention strategies for CRCs. Established screening modalities have significantly reduced CRC incidence and mortality: sigmoidoscopy lowers distal CRC mortality [38], colonoscopic polypectomy removes precancerous lesions [39], and annual fecal occult blood testing (FOBT) reduces mortality by approximately 33% [40]. Randomized and observational studies confirm the benefit of flexible sigmoidoscopy [41, 42], and although its effect on all-cause mortality is debated, the impact on CRC-specific outcomes is clear [43, 44]. Early detection improves outcomes through the identification and removal of precursor lesions [45, 46].
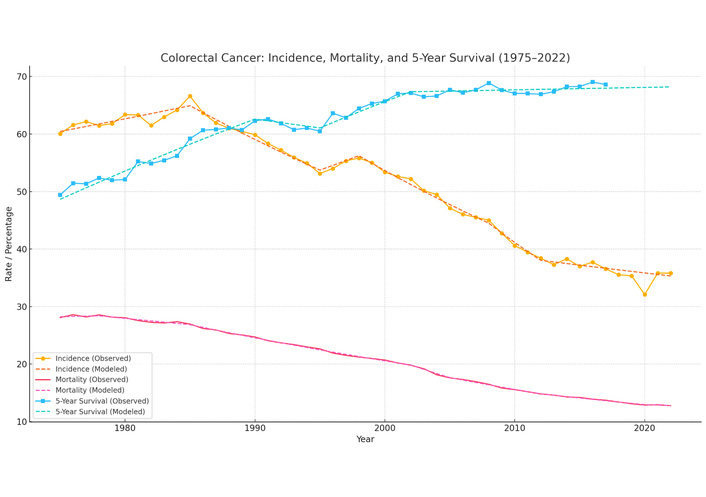
CRC trends in the U.S. from 1975 to 2022 reveal substantial improvements in prevention, treatment, and outcomes. Long-term trends in CRC incidence, mortality, and 5-year relative survival in the United States from 1975 to 2022 are illustrated in Figure 1, based on SEER and national mortality data [47]. The incidence rate, based on SEER 8 data, peaked in the mid-1980s at approximately 66.6 per 100,000 and declined steadily to about 35.8 per 100,000 by 2022—a 46% reduction—reflecting the impact of widespread screening, removal of precancerous polyps, and modifiable risk factor control. Mortality rates also fell markedly, from roughly 28 per 100,000 in 1975 to 12.8 per 100,000 in 2022 (a 54% decline), with acceleration after the mid-1990s likely due to earlier detection, advances in treatment, and coordinated care. Concurrently, 5-year relative survival improved from 49% in 1975 to over 69% by 2016, largely attributable to earlier-stage diagnoses and enhanced therapeutic strategies. While the incidence and mortality trends continue to improve, the recent plateau in survival gains highlights the need for novel approaches, including personalized treatments, targeted efforts for EOCRC, and focused interventions in high-risk populations.
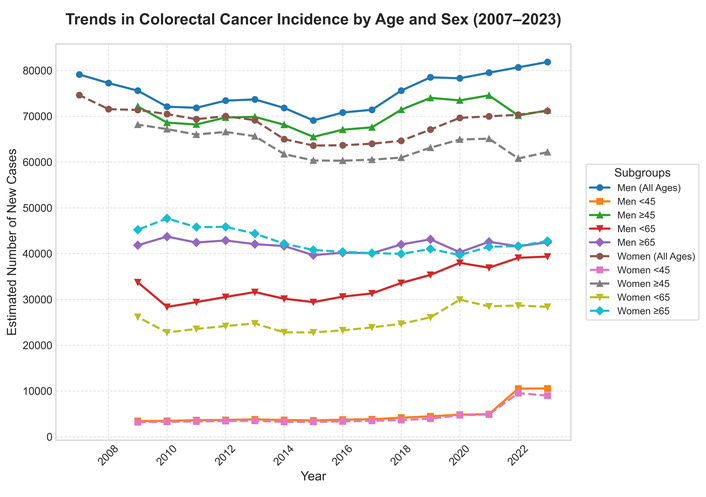
Trends in CRC incidence by age group are presented in Figure 2, though some subgroup data for 2007–2008 were not available [1, 48].
CRC patients face substantial psychological challenges after surgery, especially when postoperative complications occur [49, 50]. Complications such as infections, anastomotic leaks, prolonged recovery, and stoma formation increase the risk of depression, anxiety, and adjustment disorders, compounding physical discomfort, body-image disturbance, and social functioning difficulties. Psychiatric comorbidities in CRC patients are linked to poorer adherence to treatment, longer hospital stays, higher healthcare costs, and worse survival, underscoring the importance of early psychological screening, timely psychiatric intervention, and integration of mental health care into multidisciplinary practice [50].
Evidence supports the prognostic impact of these disorders. A three-year follow-up study of gastrointestinal cancer patients (n = 320; 210 CRC) reported baseline rates of anxiety (~40%) and depression (~33%), both of which worsened over time, with depression independently associated with reduced survival [51]. Prospective cohort studies confirm that complications and stoma creation predict poorer emotional outcomes and lower health-related quality of life, while higher anxiety and depression scores correlate with increased mortality. Predictive tools, such as risk nomograms incorporating postoperative complications, stoma creation, comorbidities, and adjuvant therapy, demonstrate good accuracy (AUC ≈ 0.79–0.81) in identifying high-risk patients [52]. Furthermore, a meta-analysis showed that anxiety modestly increases mortality risk (OR ≈ 1.07), while depression more than doubles it (OR ≈ 2.76) [53].
Taken together, these findings demonstrate that postoperative complications not only worsen psychological outcomes but may also directly influence long-term survival. Addressing mental health proactively is therefore critical for optimizing recovery, quality of life, and prognosis in CRC patients. Common disorders are summarized in Table 1.
Mental health disorders in CRC patients following postoperative complications.
| Disorder | Triggers/Associations | Impact on patients |
|---|---|---|
| Depression | Prolonged recovery, infections, stoma formation, loss of independence | Reduced quality of life, poor adherence to therapy, higher risk of mortality |
| Anxiety | Fear of recurrence, uncertainty after complications, changes in body image | Sleep disturbances, impaired coping, increased healthcare utilization |
| Adjustment disorder | Difficulty adapting to stoma, functional limitations, lifestyle disruption | Social withdrawal, reduced occupational functioning, prolonged psychological distress |
| Post-traumatic stress disorder (PTSD) | Severe or unexpected surgical complications (e.g., anastomotic leak, ICU stay) | Flashbacks, hypervigilance, avoidance behaviors, impaired daily functioning |
| Body image disturbance | Stoma placement, surgical scarring, altered bowel function | Low self-esteem, social anxiety, sexual dysfunction |
CRC: colorectal cancer.
CRC prognosis is influenced by tumor stage, histologic grade, molecular features, and host factors. Early detection through screening and molecular diagnostics has contributed to improvements in 5-year survival—from ~50% in the 1970s to 65% between 2012 and 2018—though disparities remain across age and racial groups [25, 54]. CRC development involves a complex interplay between genetic predisposition, epigenetic regulation, environmental exposures, and modifiable lifestyle factors [21, 55, 56].
Inherited syndromes (e.g., Lynch syndrome, FAP) and somatic mutations in genes such as APC, KRAS, BRAF, and TP53 underlie many CRC cases [57–59]. Epigenetic mechanisms, including MLH1 and MGMT promoter methylation, influence prognosis and therapy response. Biomarkers such as methylated NDRG4, BMP3, SEPT9, and specific miRNAs, detectable via liquid biopsy, are increasingly used for diagnosis and surveillance [60]. Polygenic risk scores enable stratified risk prediction [61], and targeted epigenetic therapies, such as DNMT and HDAC inhibitors, are under investigation [62, 63].
Modifiable risk factors include family CRC history, high-risk adenomas, IBD, diabetes, radiation exposure, and dietary habits [64, 65]. CRC often arises from adenomatous or serrated polyps, especially in the proximal colon [66, 67]. A 2025 UK cohort of over 540,000 women linked high-fiber, plant-based diets and low red/processed meat intake with lower CRC incidence, while higher fecal bile acid levels were associated with increased risk [68, 69]. Physical activity, healthy weight, and avoidance of alcohol and tobacco remain key preventive strategies [70, 71].
Environmental factors such as green space access and lower socioeconomic disadvantage are also protective [72]. The gut microbiome serves as a mediator, with Fusobacterium nucleatum promoting immune evasion and CRC progression, while beneficial microbial metabolites influence therapeutic response [73, 74]. Dietary interventions post-diagnosis—emphasizing whole grains, calcium, and coffee—improve survival, whereas high sugar and alcohol intake worsen outcomes. Obesity, especially in youth, elevates CRC risk through inflammatory and metabolic pathways, contributing to EOCRC with a 1.54-fold increased risk [32, 75]. A murine RCT showed that ketogenic diets reduced tumor burden by modulating microbiota [76], and probiotic or fiber-rich interventions are gaining clinical interest [77, 78].
Immunologically, mismatch repair-deficient (dMMR)/high microsatellite instability (MSI-H) tumors respond well to immune checkpoint inhibitors, while microsatellite stable (MSS) CRCs (~85%) remain resistant due to poor antigenicity and suppressive microenvironments [79–91]. Novel strategies such as tumor mutational burden (TMB)-based stratification, CAR-T cells, vaccines, and oncolytic viruses are being explored to overcome immune resistance [92–100].
Advanced molecular diagnostics, including next-generation sequencing (NGS), identify actionable mutations for targeted therapy and resistance prediction (e.g., KRAS, NRAS, BRAF, PIK3CA) [101–104]. Liquid biopsies enable real-time monitoring of circulating tumor DNA (ctDNA), improving surveillance for minimal residual disease and enabling adaptive treatment strategies [105–108].
Molecular pathological epidemiology (MPE) provides a transdisciplinary framework for integrating these factors [109]. MPE links exposures—such as diet, BMI, and aspirin use—with tumor-specific molecular alterations, including MSI, CIMP, and LINE-1 methylation, offering insights into etiologic heterogeneity and clinical stratification [110–116]. Gestational and early-life exposures may shape CRC phenotypes, and MPE-based pregnancy cohort studies could further elucidate these connections [117–119]. AI enhances MPE by predicting molecular subtypes from histology (e.g., Swin Transformers) and identifying prognostic multi-omics signatures, improving the integration of exposomic, imaging, and biomarker data into personalized oncology [114, 119–121].
CRC screening options vary in sensitivity, specificity, cost, and accessibility, with test selection influenced by age, risk, and patient preference. Positive results typically require diagnostic follow-up via colonoscopy. The U.S. Preventive Services Task Force (USPSTF) recommends several screening methods, including HSgFOBT, fecal immunochemical test (FIT), FIT-DNA (Cologuard), computed tomography (CT) colonography, flexible sigmoidoscopy, and colonoscopy, each with different costs and effectiveness profiles (Table 2).
USPSTF recommended colorectal cancer screening tests.
| Test | USPSTF recommended frequency | Sensitivity | Specificity | Cost | CDPHP coverage |
|---|---|---|---|---|---|
| High-sensitivity guaiac fecal occult blood test (HSgFOBT) | Every year | Low (33%) | Moderate | $22 | Yes |
| Fecal immunochemical test (FIT-iFOBT) | Every year | Moderate (75%) | Moderate | $22 | Yes |
| FIT-DNA (Cologuard) | Every 3 years | High (92%) | High | $502 | Yes |
| Computed tomography colonography | Every 5 years | High (89%) | High (75%) | $315 | Prior authorization required |
| Flexible sigmoidoscopy | Every 5 years | Moderate to high (> 95% in distal colon) | High | $520 | Yes |
| Colonoscopy | Every 10 years | High (93%) | High (73%) | $950 | Yes |
USPSTF: U.S. Preventive Services Task Force.
Cologuard, despite its $502 price, offers high sensitivity, non-invasiveness, and at-home convenience, enhancing compliance and early detection. Colonoscopy remains the gold standard with high accuracy but is more costly and invasive. Prices vary significantly by provider type: surgery centers offer 29% lower costs than outpatient hospitals—for example, $1,136 vs. $1,608 for standard colonoscopy [122].
A detailed breakdown shows facility fees make up nearly 64% of total colonoscopy costs, with anesthesia and provider fees comprising the remainder [123]. Costs also vary by state: Alaska has the highest average at $2,033, while Iowa has the lowest at $1,430 [123].
Understanding the financial aspects of CRC screening is vital for improving access, especially among uninsured populations. Transparent pricing, insurance coverage, and cost-effective options are essential to reducing disparities and enhancing preventive care.
The Affordable Care Act (ACA) mandates that private health plans initiated on or after September 23, 2010, cover USPSTF-recommended CRC screening tests with no out-of-pocket costs for eligible individuals [124]. Medicare and most Medicaid programs also cover CRC screening—including colonoscopy, sigmoidoscopy, fecal occult blood tests, and stool DNA tests—though Medicaid eligibility and guidelines vary by state [22, 125, 126]. A summary of coverage across insurance types is presented in Table 3.
Insurance coverage for colorectal cancer screening tests.
| Insurance type | Screening tests covered | Out-of-pocket costs | Guidelines and eligibility |
|---|---|---|---|
| Medicare | Colonoscopy, Sigmoidoscopy, Fecal Occult Blood Test, Stool DNA Test | No out-of-pocket costs for most services | Coverage for eligible beneficiaries as per CMS guidelines |
| Medicaid | Colonoscopy, Sigmoidoscopy, Fecal Occult Blood Test, Stool DNA Test | Varies by state | Coverage and eligibility criteria differ by state; states follow CMS and USPSTF recommendations |
| Private insurance | Colonoscopy, Sigmoidoscopy, Fecal Occult Blood Test, Stool DNA Test | No out-of-pocket costs for most services | Coverage mandated by ACA for plans starting on or after September 23, 2010; adheres to USPSTF recommendations |
CMS: Centers for Medicare and Medicaid Services; USPSTF: U.S. Preventive Services Task Force; ACA: Affordable Care Act.
Despite these provisions, disparities persist. National Health Interview Survey (NHIS) and Behavioral Risk Factor Surveillance System (BRFSS) data show lower CRC screening rates among uninsured individuals compared to those with Medicaid or private insurance [24, 127]. In adults aged 50–64, the 2005 NHIS data found screening rates of 48.5% [private Health Maintenance Organization (HMO)], 45.2% (private non-HMO), 42.1% (medicaid/other public), and only 17.2% (uninsured) [127].
Insurance coverage is critical to expanding access to preventive care. By removing financial barriers, Medicare, Medicaid, and ACA-aligned private plans improve screening uptake and early CRC detection, especially in underserved populations [128–130].
CRC screening includes stool-based, blood-based, and visual/structural exams, each with distinct sensitivity, specificity, and frequency considerations.
gFOBT detects hidden blood via a chemical reaction but requires dietary restrictions and has low specificity [131, 132].
FIT uses antibodies to detect human hemoglobin without dietary restrictions; annual use is recommended with 79% sensitivity and 94% specificity [133–135].
FIT-DNA (Cologuard®) combines FIT with DNA testing (e.g., KRAS, BMP3), offering 92% sensitivity for CRC and a 3-year interval [136–138].
See Table 4 for test comparisons.
Fecal occult blood tests (FOBT) for colorectal cancer screening.
| Test type | Example brand | Detection method | Dietary restrictions | Sensitivity to human hemoglobin |
|---|---|---|---|---|
| gFOBT | Hemocult® | Chemical reaction | Yes | Less specific |
| FIT | InSure® | Immunological reaction | No | More specific and sensitive |
| FIT-DNA | ColoGuard® | DNA and immunological test | No | More specific and sensitive |
FIT: fecal immunochemical test.
Blood-based screening detects CRC-related cell-free DNA (cfDNA) and methylation markers like methylated SEPT9 (mSEPT9). Tests include Epi proColon®, Guardant, Freenome, Grail, and others [139, 140].
Epi proColon® is an FDA-approved blood-based screening test for CRC that detects mSEPT9 DNA in plasma. However, its sensitivity (approximately 48–73%) and specificity (around 80%) do not meet the Centers for Medicare and Medicaid Services (CMS) minimum thresholds for coverage (≥ 74% sensitivity and ≥ 90% specificity), and thus it is not currently covered by Medicare [139, 141–145].
Guardant Shield, validated by Chung et al. [146], showed 83.1% sensitivity and 89.6% specificity in average-risk adults.
Compared to FIT, mSEPT9 has lower specificity (82% vs. 97%) [147].
See Table 5 for details.
CRC screening tests using blood-based markers with AI integration and cited performance.
| Blood test name or vendor | Analytes | Target | AI algorithm + input Data | Performance metrics | References |
|---|---|---|---|---|---|
| mSEPT9 | ctDNA | CRC specific | Random forest (cfDNA methylation data) | AUC 0.82–0.89; Sens 69–77%; Spec 88–92% | [148, 149] |
| Freenome | ctDNA + protein | CRC specific | Ensemble deep learning (multi-omics: cfDNA, protein) | AUC 0.94; Sens 79–91%; Spec 91–96% | [150, 151] |
| CancerSEEK | ctDNA + protein | Multi-cancer | Random forest + logistic regression (multi-analyte) | AUC 0.94; Sens 69% (CRC); Spec 99% | [152, 153] |
| Guardant | ctDNA | CRC specific | Targeted NGS + ML classifier (proprietary) | Sens ~91%; Spec ~94% | [154, 155] |
| Grail (Galleri) | ctDNA | Multi-cancer | Deep neural networks (cfDNA methylation) | Sens 67% (CRC); Spec 99.5%; PPV 88.7%; early-stage sens ~27.5% | [156–165] |
| Clinical Genomics | ctDNA | CRC specific | Likely logistic regression/SVM on methylation | Sens 81%; Spec 91% (early trials) | [166–169] |
CRC: colorectal cancer; AI: artificial intelligence; mSEPT9: methylated SEPT9; ctDNA: circulating tumor DNA; cfDNA: cell-free DNA; Sens: sensitivity; Spec: specificity; ML: machine learning.
Capsule endoscopy captures images via a swallowed camera capsule; sensitivity is 88% for polyps ≥ 6 mm, but may miss sessile/flat lesions [170, 171].
CT colonography is noninvasive, with 67–98% sensitivity for adenomas ≥ 6–10 mm but less effective for flat polyps; recommended every 5 years [172, 173].
Sigmoidoscopy visualizes the distal colon; less favored in the U.S. due to its limited reach (only 60% of CRCs occur distally) [131].
Colonoscopy is the gold standard, enabling full visualization and polyp removal, with a 10-year screening interval and rare complications [131].
Each test offers trade-offs in accuracy, invasiveness, and cost. Selection should consider patient risk, preference, and access. Combining emerging technologies (e.g., liquid biopsy) with traditional screening methods may enhance early detection and population coverage.
CRC screening has substantially reduced incidence and mortality, accounting for 53% of a 26% decline in U.S. CRC mortality between 1975 and 2000 [174]. Screening effectiveness depends on test sensitivity, specificity, and evidence quality. The CMS recommends triennial blood-based screening for adults aged 50–85 only if sensitivity is ≥ 74% and specificity ≥ 90% [175, 176].
Historically, FOBT was supported by randomized trials, but it is no longer recommended due to limited accuracy. The FIT is now preferred for annual screening because of superior sensitivity and specificity, while stool DNA-FIT tests (e.g., Cologuard), though more costly and prone to false positives, are suggested every 1–3 years [177–179]. Colonoscopy remains the gold standard, offering the greatest reduction in CRC risk and mortality; for example, a large cohort study showed that a normal colonoscopy reduced CRC risk by 46% and mortality by 88% over 12 years [180]. Comparative modeling supports lowering the screening initiation age to 45, given the rise in EOCRC [181]. Colonoscopy prevents the most CRC cases and deaths but requires more procedures and carries higher complication risks, while FIT and stool DNA-FIT result in fewer colonoscopies per 1,000 individuals screened [182].
Despite strong evidence, screening efficacy is limited by test performance and implementation challenges. FIT may miss serrated lesions, stool DNA-FIT has higher false-positive rates, and nearly 23% of CRC deaths are linked to missed or incomplete screening [183]. Colonoscopy outcomes depend on bowel preparation quality, endoscopist skill, sedation practices, and completeness of lesion removal. Higher adenoma detection rates (ADR) are directly protective; a 1% increase in ADR reduces interval CRC risk by 3% [184, 185]. To optimize outcomes, some institutions restrict procedures to gastroenterologists, and regional differences in sedation practices affect exam completeness and patient tolerance [186]. Expanded colonoscopy uptake, as seen in Korea, has improved early detection rates [187].
Emerging innovations are reshaping CRC screening. Liquid biopsy enables early detection and recurrence monitoring through ctDNA [188], while AI-assisted tools improve polyp detection and risk stratification [189–191]. However, AI adoption faces barriers including algorithmic bias from non-representative datasets, limited annotated samples, inconsistent data quality, and ethical issues related to privacy, consent, and the opacity of “black-box” algorithms. These challenges limit clinical trust and regulatory approval, particularly in low-resource settings with constrained infrastructure and expertise.
Persistent disparities in screening uptake across income, race, gender, and geography remain a critical concern [192, 193]. Targeted strategies—such as mailed FIT kits, telehealth, mobile clinics, and culturally tailored outreach—have been effective in improving access [194–198]. Policy initiatives, including expanded insurance coverage and preventive care subsidies, have also helped reduce racial disparities in CRC outcomes by nearly 50% over the past decade [199, 200].
A combined approach—anchored in evidence-based guidelines, optimized procedural quality, technological innovation, and equitable access—is essential to maximize CRC screening effectiveness and reduce disease burden across diverse populations.
CRC screening remains a cornerstone of early detection and prevention efforts in the U.S. [201–203]. National campaigns—such as the National Colorectal Cancer Roundtable’s “80% by 2018” and Healthy People 2020—have aimed to boost uptake [204, 205]. Surveillance tools like BRFSS, NHIS, and the NCI State Cancer Profiles track national and subnational progress and disparities [203].
Screening rates for adults aged ≥ 45 rose from 52% in 2002 to 68% in 2020 but remain suboptimal, with state-level rates ranging from 50–70% [206, 207]. Disparities persist among younger adults, Asian Americans, women, and the uninsured due to lower referral rates, provider preferences, or structural barriers [25, 208, 209]. Notably, 83% of unscreened individuals had never undergone testing [208]. In light of rising EOCRC, likely due to birth-cohort effects, guidelines now recommend beginning screening at age 45 [210].
While modeling suggests that lowering the screening age to 45 could prevent 29,400 CRC cases and 11,100 deaths over five years, raising screening rates to 80% among those aged 50–75 could avert nearly three times as many deaths at a lower cost [211, 212].
Quality measurement frameworks such as the Healthcare Effectiveness Data and Information Set (HEDIS) further support screening improvements. Used by over 90% of U.S. health plans and integrated into Medicare Advantage Star Ratings, HEDIS identifies care gaps and supports performance benchmarking [213, 214]. CRC screening rates derived from HEDIS data guide incentive programs like Pay for Performance and Quality Bonus Funds [215, 216], relying on accurate billing and documentation to ensure quality assessment [217–219].
The CRC screening measure assesses adults ages 50–75 who received appropriate screening using any of the following modalities: annual fecal occult blood test, flexible sigmoidoscopy every 5 years, colonoscopy every 10 years, CT colonography every 5 years, or stool DNA test every 3 years. In alignment with the USPSTF recommendations, the HEDIS Measurement Year 2022 update expanded the eligible age range to 45–75 years [220].
Longitudinal data from 2004 to 2023 indicate evolving colorectal cancer (CRC) screening rates across four major insurance categories [220]. Commercial HMO and Medicare HMO plans consistently achieved higher screening rates compared to their Preferred Provider Organization (PPO) counterparts. Medicare HMO showed a substantial increase beginning around 2010, peaking above 70% in 2018 and 2020, while Commercial HMO maintained relatively stable rates in the low-to-mid 60% range. Medicare PPO exhibited a similar upward trend, albeit with greater variability, and Commercial PPO—though improving—persistently trailed behind HMO plans throughout the period.
Data for 2019 were unavailable for both Medicare HMO and Medicare PPO due to the CMS suspension of reporting during the COVID-19 pandemic, underscoring broader disruptions to healthcare quality measurement. These long-term trends highlight the effectiveness of managed care models, particularly HMOs, in promoting preventive screening. Ongoing investment in public health initiatives and standardized quality metrics remains essential to increasing CRC screening uptake and reducing disparities across insured populations.
AI, particularly deep learning, is rapidly transforming modern medicine, and CRC diagnosis is no exception. Built on neural network architectures, deep learning has shown strong performance in analyzing medical images, pathology slides, and genomic data with high accuracy [221–223].
CRC remains a major global health burden, where early detection is essential to improving survival. Advances in AI and ML are reshaping care through imaging, risk stratification, and precision treatment. AI enhances diagnostic accuracy via automated detection, biomarker discovery, and convolutional neural networks for image analysis, reducing variability in histopathological interpretation and supporting treatment planning [224]. For example, Case Western investigators demonstrated that AI applied to routine magnetic resonance imaging (MRI) could predict rectal cancer outcomes, offering a non-invasive strategy to avoid overtreatment [225]. At the same time, concerns remain that unequal access to quality imaging may exacerbate existing disparities [226].
AI is also transforming traditional CRC screening and diagnostics. Computer-aided detection (CAD) systems in colonoscopy improve adenoma and polyp detection [227, 228], while deep learning applied to CT and MRI enhances staging and localization [229, 230]. In pathology, AI enables automated tumor classification and prediction of MSI, informing immunotherapy decisions [231, 232]. Beyond imaging, AI augments liquid biopsy by interpreting ctDNA signals to detect minimal residual disease and recurrence risk [233]. Innovative platforms such as Zeng et al.’s real-time optical coherence tomography system [234] may improve endoscopic sensitivity, while Bilal et al. [235] and Yu et al. [236] highlight applications in immunotherapy prediction and digital epidemiology, including GeoAI.
Despite this progress, challenges remain, including dataset variability, limited generalizability, and the need for pragmatic, large-scale validation to demonstrate real-world effectiveness [237, 238]. As Wang et al. [239] emphasize, transparent validation, equitable implementation, and integration into clinical workflows are essential for AI to meaningfully advance CRC care. With deep learning and related approaches continuing to evolve, AI is emerging as a transformative tool for screening, diagnosis, and management, moving toward more precise, data-driven, and patient-centered care.
The foundation of accurate CRC diagnosis rests on imaging modalities such as CT, MRI, and 18F-FDG positron emission tomography (PET). CT and MRI offer structural detail for staging, while PET identifies metastatic spread and treatment response. Integration with AI has the potential to elevate these modalities beyond human capabilities.
Several studies have shown how imaging innovations shape CRC management. Taylor et al. [240] found whole-body MRI to be an effective, low-radiation alternative for staging, while Maas et al. [241] demonstrated its accuracy in detecting recurrent disease. García-Figueiras et al. [242, 243] highlight the diagnostic advantage of combining anatomical and molecular data.
AI-augmented radiomics, diffusion-weighted MRI, and contrast-enhanced protocols further refine these modalities. Liu et al. [244] and Serinsöz et al. [245] advocate for a tailored, multimodal imaging approach guided by clinical context. While Dobos et al. [246] and Kekelidze et al. [247] established the groundwork, newer AI-supported tools provide actionable insights that may support earlier detection, more accurate staging, and personalized surveillance.
AI-assisted endoscopy presents a practical avenue for reducing missed lesions and improving ADR. Kudo et al. [248] and Lui et al. [249] demonstrate how real-time AI integration enhances lesion detection, while Sinagra et al. [250] confirm increased adenoma recognition.
Beyond accuracy, AI supports procedural standardization and workflow efficiency. Zhou et al. [251] and Barua et al. [252] showed high diagnostic accuracy with AI models in neoplastic polyp identification. Broader applications are noted by Hsiao et al. [253], who validated AI for gastric cancer diagnosis, hinting at cross-cancer utility.
Despite the enthusiasm, reviews by Messmann et al. [254] and Wallace et al. [255] underscore implementation barriers, such as over-reliance, alert fatigue, and ethical oversight. Koh et al. [256] and Spadaccini et al. [257, 258] propose real-time image analysis and AI-driven classification as the next steps toward precision endoscopy.
Advanced imaging, when paired with AI, broadens diagnostic capability beyond conventional tools. Ferrari et al. [259] and Wang et al. [260] illustrate how AI enhances MRI-based assessment of treatment response in rectal cancer. Taylor et al. [240] further validated whole-body MRI as an efficient staging tool.
Emerging technologies, such as Fourier transform infrared (FTIR) imaging, benefit from AI’s pattern recognition capabilities. Villamanca et al. [261] and Gerwert et al. [262] demonstrated early detection of CRC and MSI, respectively. These technologies could inform treatment pathways without invasive biopsy.
Notably, AI expands accessibility. Waljee et al. [263] applied AI in sub-Saharan Africa, while Ziegelmayer et al. [264] used AI to differentiate CRC from diverticulitis on CT. Peng et al. [265] advanced image fusion methods, optimizing diagnostic efficiency. Together, these studies underscore AI’s role in scalable, context-sensitive diagnostics.
AI’s application in pathology imaging redefines tissue analysis by enabling automated classification, subtype identification, and biomarker detection. Sirinukunwattana et al. [266] and Wang et al. [267] demonstrated molecular subtype classification using deep learning, which supports tailored treatment planning.
Innovations such as Yu’s semi-supervised learning model [268] allow efficient use of limited labeled data, while Ho et al. [269] and Ju et al. [270] validated AI for tumor staging and survival estimation. Interpretability and transparency remain central concerns; Neto et al. [271] advocate for explainable models suitable for clinical adoption.
Saillard et al. [272] validated MSIntuit for MSI detection, and studies by Bilal [273], Griem [274], and Prezja [275] confirm AI’s effectiveness in prescreening and tissue classification. These tools collectively enable more efficient workflows and potentially reduce diagnostic delays.
AI’s ability to extract prognostic features from histopathology and imaging has advanced survival prediction in CRC. Kather et al. [276] demonstrated survival estimation using digitized slides, while Pai et al. [277] and Pham et al. [278, 279] built hybrid models incorporating imaging, gene expression, and deep learning for recurrence-free survival predictions.
Jiang et al. [280] validated MRI-based AI prognostics for rectal cancer, and L’Imperio et al. [281] used ML for colon cancer risk stratification. Wagner et al. [120] advanced biomarker prediction with transformer-based models, while Yin et al. [191] introduced a generalized transfer learning method for broader applicability.
Together, these findings suggest that AI-driven prognostics may surpass traditional staging in predicting outcomes and guiding treatment. Still, challenges remain in achieving cross-population generalizability and clinical integration.
The integration of AI in medicine has been transformative, especially for complex diseases like CRC. AI technologies, from deep learning to advanced imaging, have significantly improved the accuracy, efficiency, and personalization of cancer diagnostics and treatments. This table (Table 6) provides a chronological summary of key studies on AI in CRC, detailing each AI model, its benefits, and limitations. This organization illustrates both the technological advancements and the ongoing challenges in adopting AI tools in oncology, reflecting nearly two decades of progressive impact in the field.
A chronological overview of AI applications in colorectal cancer diagnosis, prognosis, and treatment.
| Citation | Authors (year) | AI model | Advantages | Disadvantages |
|---|---|---|---|---|
| [259] | Ferrari et al. (2019) | MR-based AI model | Predicts therapy response, non-invasive | Requires high-quality MRI, expensive technology |
| [282] | Yang et al. (2019) | Deep learning for imaging | High accuracy, non-invasive diagnosis | Requires large datasets, high computational resources |
| [283] | Mao et al. (2020) | MRI | High specificity for liver metastasis, non-invasive | High costs, availability limitations |
| [234] | Zeng et al. (2020) | PR-OCT with deep learning | Rapid diagnosis, high sensitivity | Expensive technology, requires specialized equipment |
| [239] | Wang et al. (2020) | AI for diagnosis and therapy | Improves diagnostic accuracy, potential for therapy optimization | High initial costs, need for integration into clinical practice |
| [248] | Kudo et al. (2020) | AI-assisted endoscopy | Improves adenoma detection rates, real-time analysis | Potential over-reliance on AI, need for high-quality images |
| [249] | Lui et al. (2020) | AI in colonoscopy | Reduces missed polyps, enhances detection rates | False positives, potential for over-screening |
| [250] | Sinagra et al. (2020) | AI for adenoma detection | Enhances detection rates, supports endoscopists | Requires large datasets for training, potential biases in AI models |
| [251] | Zhou et al. (2020) | Deep learning for optical diagnosis | High accuracy in optical diagnosis, non-invasive | Requires large datasets, expensive to implement |
| [225] | News-Medical.Net (2021) | AI-driven imaging | Real-time analysis, improved detection rates | Limited by data quality, potential biases |
| [253] | Hsiao et al. (2021) | AI in endoscopic screening | Early detection, high sensitivity | Expensive technology, requires specialized equipment |
| [284] | Parsa et al. (2021) | AI for polyp characterization | Reduces human error, enhances polyp characterization | Potential for over-reliance on AI, requires continuous updates |
| [285] | Wang et al. (2021) | AI for polyp detection | Improves detection rates, real-time classification | Requires large datasets, potential for false positives |
| [260] | Wang et al. (2021) | MRI-based AI model | High specificity for rectal cancer, non-invasive | High costs, limited availability |
| [266] | Sirinukunwattana et al. (2021) | Deep learning for subtyping | High accuracy in molecular subtyping, aids in personalized treatment | Requires large datasets, expensive to implement |
| [267] | Wang et al. (2021) | AI for histopathology | High accuracy in diagnosis, supports pathologists | Requires large annotated datasets, potential biases in AI models |
| [268] | Yu et al. (2021) | Semi-supervised deep learning | Reduces need for labeled data, high accuracy | Computationally intensive, requires continuous updates |
| [235] | Bilal et al. (2023) | Digital pathology with AI | Facilitates large-scale analysis, enhances pathology workflow | Potential for over-reliance on AI, data security concerns |
| [236] | Yu et al. (2022) | ML | Predictive capabilities, personalized treatment plans | Algorithm complexity, requires ongoing updates |
| [252] | Barua et al. (2022) | AI-based optical diagnosis | Real-time analysis, high accuracy in polyp detection | Potential for false positives, requires high-quality images |
| [254] | Messmann et al. (2022) | AI in gastrointestinal endoscopy | Standardizes detection, improves consistency | High costs, requires extensive training |
| [255] | Wallace et al. (2022) | AI in neoplasia detection | Reduces miss rates, enhances detection accuracy | Potential over-reliance on AI, needs constant updates |
| [261] | Villamanca et al. (2022) | AI with Fourier transform infrared | Non-invasive, high sensitivity | Requires specialized equipment, limited clinical application |
| [263] | Waljee et al. (2022) | AI/ML for early detection | Early detection in low-resource settings, scalable | Requires data and infrastructure, potential biases in training data |
| [269] | Ho et al. (2022) | Deep learning for histopathology | High accuracy, supports pathologists | Requires high-quality images, potential for false positives |
| [270] | Ju et al. (2022) | AI for pathological staging | High accuracy, non-invasive staging | Requires large datasets, expensive to implement |
| [256] | Koh et al. (2023) | AI-aided endoscopy | Enhances detection rates, supports experienced endoscopists | Expensive, requires integration into clinical practice |
| [257] | Spadaccini et al. (2023) | AI-aided endoscopy | Improves screening accuracy, real-time feedback | Potential for false positives, requires large training datasets |
| [262] | Gerwert et al. (2023) | AI-integrated infrared imaging | Label-free detection, fast results | Expensive technology, requires specialized training |
| [264] | Ziegelmayer et al. (2023) | Deep learning for CT imaging | Differentiates conditions accurately, non-invasive | Requires high-quality CT images, potential for misclassification |
| [273] | Bilal et al. (2023) | AI-based prescreening | Reduces workload for pathologists, improves efficiency | Potential for over-reliance on AI, data security concerns |
| [274] | Griem et al. (2023) | AI for tumor detection | Enhances detection accuracy, supports tissue analysis | Requires high-quality images, potential for false positives |
| [275] | Prezja et al. (2023) | Refined deep learning | High accuracy, supports tissue decomposition analysis | Requires large datasets, high computational resources |
| [272] | Saillard et al. (2023) | AI for MSI detection | High accuracy, supports pre-screening | Expensive to implement, requires specialized training |
| [120] | Wagner et al. (2023) | Transformer-based AI | High accuracy, supports biomarker prediction | Requires large datasets, computationally intensive |
| [191] | Yin et al. (2023) | Deep learning | High accuracy in diagnosis, early detection | Requires large datasets for training, high computational resources |
| [286] | Yin et al. (2023) | Generalized AI with transfer learning | High flexibility, supports multiple tasks | Requires large datasets, potential for overfitting |
| [279] | Pham et al. (2023) | AI fusion | Combines multiple data sources, high accuracy | Requires high-quality data, expensive to implement |
| [280] | Jiang et al. (2023) | Deep learning for MRI | Predicts outcomes, supports clinical decisions | Requires high-quality MRI, computationally expensive |
| [281] | L’Imperio et al. (2023) | ML for risk stratification | High accuracy, supports clinical risk assessment | Requires validation, potential for misclassification |
| [287] | Pham et al. (2023) | Markov models with AI | Predicts survival outcomes, supports clinical decision-making | Requires large datasets, computationally intensive |
| [288] | Tsai et al. (2023) | AI for multi-omics prediction | High accuracy, supports personalized medicine | Requires high-quality data, expensive to implement |
| [258] | Spadaccini et al. (2024) | AI-assisted colonoscopy | Enhances screening, reduces miss rates | Expensive, requires integration into existing systems |
| [265] | Peng et al. (2024) | ML for image fusion | Combines multiple imaging modalities, improves accuracy | Computationally expensive, requires large datasets |
| [271] | Neto et al. (2024) | Interpretable ML system | High interpretability, supports diagnosis | Requires high-quality images, potential for misclassification |
AI: artificial intelligence; MRI: magnetic resonance imaging; CT: computed tomography; ML: machine learning.
AI technologies are being applied across multiple domains of CRC screening and diagnosis, with varying levels of maturity, performance, and clinical applicability. CAD for colonoscopy is at an early adoption stage, supported by FDA approval and proven trial benefits, yet real-world outcomes remain inconsistent and operator dependent [176, 289]. Radiology AI (CT/MRI) is still investigational—demonstrating accuracy in staging and localization but hindered by dataset variability and integration challenges [229, 230, 290, 291]. Pathology AI has shown strong accuracy in tumor classification and MSI prediction in pilot studies, but its broader adoption is constrained by the need for large, diverse datasets and costly infrastructure [231, 232]. Infrared imaging with AI (e.g., FTIR spectroscopy) remains in early research, with encouraging sensitivity in distinguishing tumor from normal tissue, though limited by heterogeneity and sparse validation [189–191]. Liquid biopsy with AI (ctDNA) is emerging in clinical trials, offering promise for detecting residual disease and recurrence, but is challenged by low sensitivity in early CRC and assay standardization issues [233]. Collectively, these tools highlight both opportunities and barriers, underscoring the need for pragmatic trials, diverse datasets, transparent validation, and equity-focused implementation.
CAD for colonoscopy readiness: early adoption, with FDA-approved tools in use. Performance: improves adenoma detection in trials. Limitations: mixed results in real-world practice; dependent on visualization quality and bowel preparation. Applicability: useful adjunct for polyp detection but requires skilled operators.
AI in radiology (CT/MRI) readiness: moderate, investigational stage. Performance: accurate for staging and localization. Limitations: dataset variability and challenges with workflow integration. Applicability: potential for preoperative planning and non-invasive staging.
AI in pathology (digital slides) readiness: pilot adoption in select centers. Performance: high accuracy in tumor classification and MSI prediction. Limitations: requires large annotated datasets and costly infrastructure. Applicability: supports diagnostics and reduces workload in high-volume labs.
Infrared imaging + AI (FTIR spectroscopy) readiness: early research stage. Performance: sensitive to tumor-normal tissue distinctions with robust biomarkers. Limitations: experimental heterogeneity and limited clinical validation. Applicability: promising for intraoperative margin assessment but not yet routine.
Liquid biopsy with AI (ctDNA) readiness: emerging, under clinical trial. Performance: detects minimal residual disease and recurrence. Limitations: limited sensitivity in early CRC; assay standardization needed. Applicability: potential for surveillance and therapy guidance once validated.
Recent technological advances in surgical practice have embraced the IoT, which integrates interconnected devices, sensors, and data analytics to optimize patient care. In CRC, IoT applications are emerging across prevention, diagnosis, perioperative care, and long-term follow-up [292–295].
Early detection and screening: IoT-enabled home-based screening devices, such as smart fecal test kits and wearable biosensors, can continuously monitor biomarkers and relay results directly to healthcare providers. This real-time data sharing may enhance adherence to CRC screening programs and facilitate early diagnosis.
Surgical practice and intraoperative monitoring: In minimally invasive colorectal surgery, IoT-based smart instruments and connected laparoscopic systems improve precision, workflow, and safety. Integration with ML further enhances intraoperative decision-making, potentially reducing complications and improving oncological outcomes.
Postoperative care and survivorship: IoT-enabled wearables and mobile health platforms allow remote monitoring of vital signs, bowel function, and quality-of-life indicators after CRC surgery. These tools support early detection of complications, personalized rehabilitation, and continuity of care.
Data-driven personalized medicine: By linking patient-generated health data with electronic health records and AI-driven analytics, IoT provides a foundation for predictive modeling in CRC risk assessment, prognosis, and tailored treatment strategies.
Despite its promise, challenges remain in ensuring data security, interoperability, and equitable access, especially in low-resource settings. Nevertheless, IoT represents a transformative step toward connected, patient-centered CRC care [296].
AI has emerged as a transformative force in CRC screening and diagnosis, yet its integration into real-world practice reveals several unresolved challenges. While the USPSTF has established comprehensive CRC screening guidelines emphasizing early detection and test accessibility, a critical but often overlooked barrier involves diagnostic coding. When a colonoscopy is ordered as a “screening colonoscopy,” it is typically covered by insurance at minimal or no cost. Conversely, procedures coded as “diagnostic colonoscopies,” such as those performed for patients presenting with rectal bleeding or after a positive non-invasive test, may not be fully reimbursed, leaving patients responsible for substantial out-of-pocket costs [297]. These discrepancies extend to follow-up procedures after positive FIT or stool DNA assays, where the confirmatory colonoscopy is often reclassified as diagnostic rather than screening. Such financial disincentives may inadvertently discourage patients from participating in non-invasive testing despite its proven effectiveness and convenience.
Beyond systemic coding and reimbursement challenges, AI-driven tools hold great promise for improving CRC screening accuracy, enhancing polyp detection, and enabling more individualized treatment strategies through the integration of radiologic, pathologic, and genomic data. However, AI’s performance remains contingent on the quality of visual information provided during endoscopic procedures. The maxim “AI cannot detect what it cannot see” highlights its dependency on operator technique and visualization quality. Incomplete mucosal inspection due to colonic folds, residual stool, or suboptimal bowel preparation can lead to missed lesions and reduced diagnostic accuracy [176]. As such, technological advances must coincide with rigorous procedural standards and comprehensive operator training.
Evidence from clinical studies underscores the variability of AI performance between controlled and pragmatic environments. Ladabaum et al. (2023) [289] demonstrated that CAD systems did not significantly improve polyp detection rates among colonoscopists in real-world settings, contrasting with earlier randomized trials and meta-analyses showing improved ADR under experimental conditions [227, 228, 298–302]. This discrepancy underscores the persistent gap between experimental efficacy and practical effectiveness. Factors such as operator dependency, variation in bowel preparation, and system integration influence outcomes. Additional concerns include dataset bias, the generalizability of training populations, and whether excessive reliance on CAD may erode traditional diagnostic competencies among gastroenterology trainees. Several fellowship directors have expressed apprehension that overdependence on AI-assisted devices could impede the development of essential observational and interpretive skills required for independent clinical judgment. These concerns align with broader issues regarding model transparency, accountability, and long-term clinical utility [237, 238, 303].
Collectively, these findings highlight the need for a balanced approach that integrates AI as an adjunct rather than a substitute for human expertise. While AI can augment lesion detection, standardize quality metrics, and provide real-time decision support, its success ultimately depends on maintaining operator proficiency, ensuring rigorous validation, and addressing systemic and ethical constraints.
Moving forward, the integration of AI into CRC screening should focus on evidence-based, equitable, and transparent implementation strategies. Large-scale, multicenter pragmatic trials are needed to validate CAD and ML models across diverse patient populations and practice settings, ensuring reproducibility and generalizability beyond controlled environments [238]. Refinement of algorithms to mitigate bias, enhance interpretability, and ensure continuous learning within regulatory frameworks will be essential for clinical trust and adoption [237].
Parallel to technical advancements, structured training programs should educate clinicians on AI-assisted workflows without diminishing traditional diagnostic skill development. AI should serve as a complement to, not a replacement for, the human eye—providing feedback, identifying overlooked regions, and reinforcing procedural completeness. Integration within electronic health record and imaging platforms should prioritize workflow efficiency, data security, and algorithmic transparency [303].
Finally, addressing systemic barriers such as diagnostic coding inconsistencies and financial inequities is essential to ensure that screening innovations translate into real-world health benefits. Policy efforts should advocate for insurance frameworks that classify follow-up colonoscopies after positive non-invasive tests as screening procedures, reducing patient cost burdens and improving adherence. Through interdisciplinary collaboration among gastroenterologists, radiologists, data scientists, ethicists, and policymakers, AI can evolve from an experimental adjunct to a practical, equitable, and ethically grounded instrument in the global effort to reduce CRC mortality.
CRC continues to represent a major public health challenge, demanding innovative yet practical approaches that improve early detection and outcomes. AI has emerged as a pivotal component in this evolution, enhancing diagnostic precision and offering opportunities for individualized, data-driven care. However, its ultimate impact will depend on how effectively technology is aligned with the realities of clinical practice, patient equity, and system-level integration.
As the field advances, emphasis should shift from proof-of-concept demonstrations to measurable improvements in patient outcomes, workflow efficiency, and accessibility. The successful adoption of AI-driven screening requires not only technological refinement but also robust validation, transparent regulation, and sustained clinician engagement. Importantly, ethical stewardship—encompassing data integrity, patient trust, and equitable access—must remain at the forefront of AI implementation.
Looking ahead, a multidisciplinary framework that unites clinicians, data scientists, health economists, and policymakers will be critical to ensure that innovation translates into population-level benefit. By coupling precision technologies with health-system reform and patient-centered delivery models, the integration of AI into CRC screening and diagnosis can meaningfully contribute to reducing disease burden and improving long-term outcomes worldwide.
ACA: Affordable Care Act
ADR: adenoma detection rates
AI: artificial intelligence
BRFSS: Behavioral Risk Factor Surveillance System
CAD: computer-aided detection
CMS: Centers for Medicare and Medicaid Services
CRC: colorectal cancer
CT: computed tomography
ctDNA: circulating tumor DNA
EOCRC: early-onset colorectal cancer
FIT: fecal immunochemical test
FOBT: fecal occult blood testing
FTIR: Fourier transform infrared
GEOCRCTT: Global Early-Onset Colorectal Cancer Think Tank
HEDIS: Healthcare Effectiveness Data and Information Set
HMO: Health Maintenance Organization
IoT: internet of things
LMICs: low- and middle-income countries
ML: machine learning
MPE: molecular pathological epidemiology
MRI: magnetic resonance imaging
mSEPT9: methylated SEPT9
MSI: microsatellite instability
NHIS: National Health Interview Survey
PET: positron emission tomography
PPO: Preferred Provider Organization
USPSTF: U.S. Preventive Services Task Force
AI-Assisted Work Statement: During the preparation of this work, the authors used MS PowerPoint and ChatGPT to put together the text and icons to generate the graphical abstract. After using MS PowerPoint and ChatGPT to generate the image, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
TDP: Conceptualization. DTPL: Writing—original draft, Conceptualization. Both authors read, edited, and approved the submitted version.
Dr. Tuan D. Pham, who is the Editorial Board Member of Exploration of Medicine, had no involvement in the decision-making or review process of this manuscript. The other author declares that he has no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.