Original Article
Original Article

Affiliation:
1Department of Pulmonology and Respiratory, Faculty of Medicine, Hasanuddin University, Makassar 90245, Indonesia
2Dr. Wahidin Sudirohusodo Hospital, Makassar 90245, Indonesia
Email: irawatydjaharuddin@unhas.ac.id
ORCID: https://orcid.org/0000-0002-5240-4950
Affiliation:
2Dr. Wahidin Sudirohusodo Hospital, Makassar 90245, Indonesia
ORCID: https://orcid.org/0000-0002-1223-9401
Affiliation:
1Department of Pulmonology and Respiratory, Faculty of Medicine, Hasanuddin University, Makassar 90245, Indonesia
ORCID: https://orcid.org/0009-0007-3155-1680
Affiliation:
3Faculty of Medicine, Hasanuddin University, Makassar 90245, Indonesia
ORCID: https://orcid.org/0000-0002-3944-9556
Affiliation:
4Department of Clinical Pathology, Dharmais National Cancer Hospital, Jakarta 11420, Indonesia
Explor Immunol. 2026;6:1003250 DOI: https://doi.org/10.37349/ei.2026.1003250
Received: June 05, 2025 Accepted: March 31, 2026 Published: April 23, 2026
Academic Editor: Narinder K. Mehra, Indian Council of Medical Research, India
Aim: Pneumonia is the leading cause of morbidity and mortality among elderly individuals. This has led to the search for reliable tools such as inflammatory biomarkers, including C-reactive protein (CRP), procalcitonin (PCT), and neutrophil-to-lymphocyte ratio (NLR), to predict disease severity and prognosis. However, the prognostic value of inflammatory biomarkers in elderly women is not fully understood, as the population is often underrepresented in clinical studies.
Methods: This retrospective study was conducted at Wahidin Sudirohusodo Hospital, Indonesia. The samples used were elderly women aged ≥ 60 years who were hospitalized with community-acquired pneumonia (CAP) between January and December 2023. CRP, PCT, and NLR levels collected within 24 hours of admission were evaluated and correlated with pneumonia severity index (PSI) scores and in-hospital mortality (IHM). Subsequently, receiver operating characteristic (ROC) curve analysis, logistic regression, and Kaplan-Meier survival analysis were performed.
Results: A total of 262 patients (median age 66 years) were included, of whom 83.2% had mild CAP, and 87.0% survived. Among inflammatory biomarkers, CRP showed the highest, with limited discriminatory ability for mortality [area under the curve (AUC) 0.543], followed by NLR (AUC 0.495), and PCT (AUC 0.466). All markers had high sensitivity (91.2%) but low specificity, and CRP ≥ 14.5 mg/L was significantly associated with reduced survival (p = 0.018).
Conclusions: CRP shows a modest prognostic value in predicting mortality among elderly women with CAP, while NLR and PCT have limited utility. These results show the need for gender- and age-specific studies to improve risk stratification and outcomes in the vulnerable population.
Pneumonia is the leading cause of morbidity and mortality among elderly individuals [1]. This has led to the search for reliable tools such as inflammatory biomarkers, including C-reactive protein (CRP), procalcitonin (PCT), and the neutrophil-to-lymphocyte ratio (NLR), to predict disease severity and prognosis [2]. However, existing literature has mainly focused on general populations, leaving a knowledge gap on how the biomarkers function specifically in elderly women, a group that is often underrepresented in clinical studies [3].
Although men are generally reported to have a 13% higher in-hospital mortality (IHM) from pneumonia, some studies show conflicting results [4, 5]. For example, a large Spanish study found a 5% higher risk of death in women, indicating the complexities of gender differences in pneumonia outcomes [4]. Potential factors contributing to variation in results include gender-related biases in healthcare delivery, with women often presenting late to hospitals and receiving delayed treatment. These delays can worsen the condition, leading to poorer outcomes, particularly in pneumonia. There is also an initial presentation with milder symptoms that contributes to underreporting of cases and delay in seeking care [5–7].
Based on the description above, this study aims to evaluate the prognostic value of CRP, PCT, and NLR in predicting mortality in elderly women diagnosed with community-acquired pneumonia (CAP). By focusing exclusively on this population, the results are expected to provide targeted insights into the role of inflammatory biomarkers in predicting adverse outcomes in elderly women with CAP. This study also hypothesizes that inflammatory biomarkers can provide valuable information for early risk stratification, potentially improving clinical decision-making for the vulnerable group.
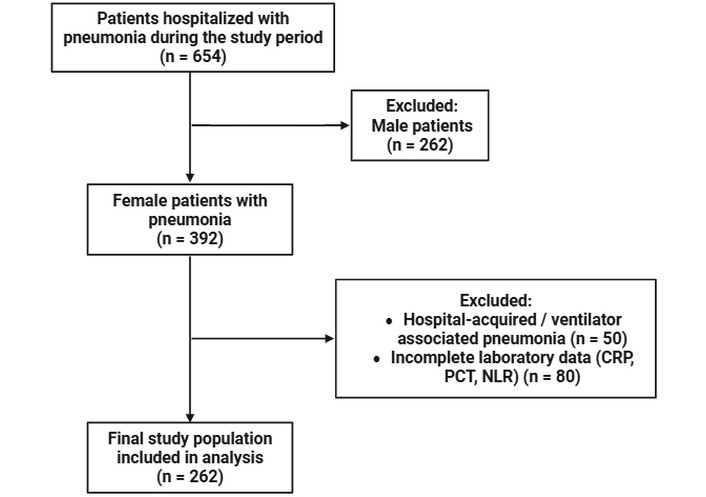
This retrospective study was conducted using data collected from January 2023 to December 2023 at Wahidin Sudirohusodo Hospital, a tertiary hospital in eastern Indonesia. The inclusion criteria were female patients diagnosed with pneumonia and aged ≥ 60 years. Patients were excluded if they were male, had hospital-acquired or ventilator-associated pneumonia, or had incomplete laboratory data (CRP, PCT, and NLR), as shown in Figure 1.
CAP was diagnosed based on typical lower respiratory tract symptoms and the presence of a new infiltrate on chest X-ray, in the absence of an alternative explanation. Treatment and hospital discharge decisions were made by medical staff. Subsequently, all patients were followed up until IHM or discharge as the outcome of interest.
All laboratory data were recorded in medical records, followed by blood sample collection in the first 24 hours of admittance. CRP, PCT, white blood cell (WBC) counts, and differential counts (neutrophils and lymphocytes) were measured from these samples, and NLR was calculated as the ratio of neutrophils to lymphocytes.
Counts of WBC, neutrophils, and lymphocytes were made using a BC-6800 Plus hematology analyzer (Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China). Serum levels of CRP and PCT were measured using immunoassay methods on the Architect Plus ci4100 analyzer (Abbott Laboratories, USA).
All continuous variables were expressed as the median and interquartile range because of their abnormal distribution. The association between inflammatory markers and pneumonia severity index (PSI) was evaluated by Spearman correlation. Furthermore, composite biomarkers were generated using bivariate logistic regression models that included CRP, PCT, and NLR. Diagnostic accuracy for each biomarker, alone and in combination, was evaluated using receiver operating characteristic (ROC) curve analysis and area under the curve (AUC) values. Multicollinearity among CRP, PCT, and NLR was assessed using the variance inflation factor (VIF) obtained from linear regression analysis.
For each biomarker, sensitivity and specificity values were obtained from ROC coordinates, and the optimal cut-off point was determined using the Youden index. The cut-off values were applied to survival analysis using Kaplan-Meier, and the data obtained were analyzed using SPSS 26.0 for Windows. The correlation graph was extracted using GraphPad Prism 10, and the level of significance for all statistical tests was defined as a two-sided p < 0.05.
A total of 262 pneumonia patients were included in this study, with a median age of 66 years (60–91). The results showed that most cases were mild (83.2%), with a median PSI of 73.00 (50–320). The majority of patients (93.5%, general wards) received in-hospital treatment, and 87.0% survived. Furthermore, the median in-hospital days was 10.00 days (1–44), with values of 5.06, 69.00 mg/L, and 1.30 ng/mL for NLR, CRP, and PCT, respectively (Table 1).
Baseline characteristics.
| Characteristics | N = 262 |
|---|---|
| Age [median (min–max)] | 66 (60–91) |
| Pneumonia severity | |
| Mild | 218 (83.2%) |
| Severe | 44 (16.8%) |
| Pneumonia severity index (PSI) | 73.00 (50–320) |
| Types of care | |
| Ward | 245 (93.5%) |
| HCU | 11 (4.2%) |
| ICU | 6 (2.3%) |
| Outcome | |
| Survive | 228 (87.0%) |
| Non-survivor | 34 (13.0%) |
| In-hospital days | 10.00 (1–44) |
| NLR | 5.06 (0.07–162.00) |
| CRP (mg/L) | 69.00 (0.05–220.00) |
| PCT (ng/mL) | 1.30 (0.01–50.00) |
HCU: high care unit; ICU: intensive care unit; NLR: neutrophil-to-lymphocyte ratio; CRP: C-reactive protein; PCT: procalcitonin.
A Spearman rank-order correlation was performed to evaluate the relationships among PSI, NLR, PCT, and CRP (Figure 2).
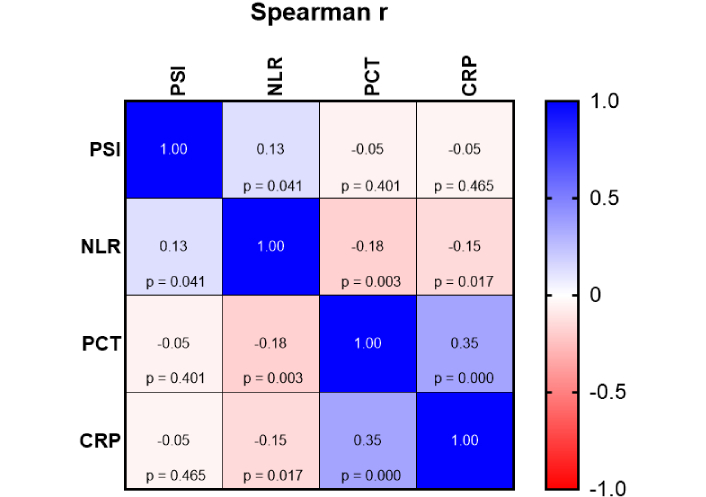
Spearman correlation matrix of PSI, NLR, PCT, and CRP levels. Spearman correlation heatmap shows the relationships between PSI, NLR, PCT, and CRP levels. Correlation coefficients (Spearman’s r) are shown in each cell, with corresponding p-values presented below. The color scale represents the magnitude and direction of the correlation, ranging from –1 (red, strong negative correlation) to +1 (blue, strong positive correlation). Statistically significant correlations (p < 0.05) are observed between NLR and PSI, PCT and NLR, PCT and CRP, and CRP and NLR. CRP: C-reactive protein; NLR: neutrophil-to-lymphocyte ratio; PCT: procalcitonin; PSI: pneumonia severity index.
The analysis showed a weak but statistically significant positive correlation between PSI and NLR (r = 0.13, p = 0.041). NLR showed a statistically significant negative correlation with both PCT (r = –0.18, p = 0.003) and CRP (r = –0.15, p = 0.017). Furthermore, a moderate and statistically significant positive correlation was observed between PCT and CRP (r = 0.35, p < 0.001). In comparison, the correlations between PSI and PCT (r = –0.05, p = 0.401) as well as PSI and CRP (r = –0.05, p = 0.465) were weak and not statistically significant.
To evaluate the predictive performance of inflammatory biomarkers for mortality in patients with CAP, ROC curve analysis was conducted for NLR, PCT, and CRP. Among these biomarkers, CRP showed the highest AUC, but with limited discriminatory ability (AUC 0.543; 95% CI 0.449–0.636). NLR showed an AUC of 0.495 (95% CI 0.394–0.596), while PCT had 0.466 (95% CI 0.367–0.564) (Figure 3A). These results indicated that none of the evaluated inflammatory biomarkers provided strong discrimination for mortality prediction in CAP. A logistic regression model combining NLR, PCT, and CRP showed an AUC of 0.538 (95% CI 0.432–0.644). However, the combined model did not show significant improvement in predictive accuracy compared to the individual biomarkers (Figure 3B).
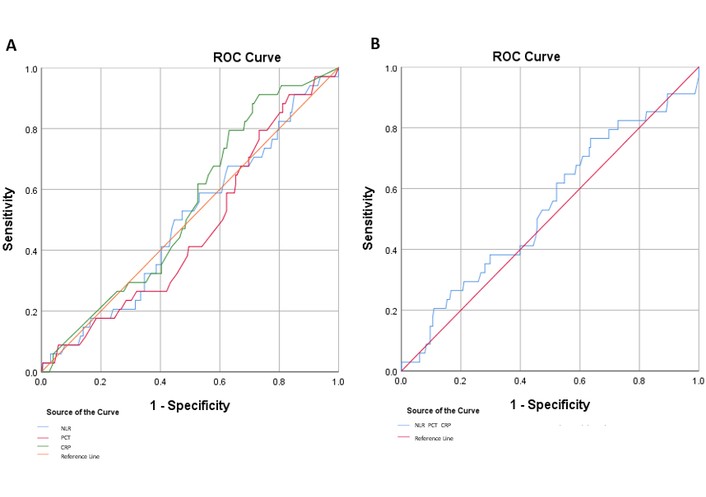
ROC curves of inflammatory biomarkers for mortality prediction. ROC curve analyses evaluating the diagnostic performance of NLR, PCT, and CRP. (A) ROC curves for NLR, PCT, and CRP in predicting mortality outcome. (B) Combined ROC analysis of the three biomarkers (NLR, PCT, CRP) to assess their collective predictive value. The reference line (red) represents a test with no discriminative power (AUC = 0.5). Sensitivity is plotted against 1 – specificity to visualize diagnostic accuracy. Biomarkers with curves closer to the upper left corner demonstrate better diagnostic performance. AUC: area under the curve; CRP: C-reactive protein; NLR: neutrophil-to-lymphocyte ratio; PCT: procalcitonin; ROC: receiver operating characteristic.
The diagnostic accuracy of individual biomarkers was further assessed using the optimal cut-off values identified from ROC analysis. The results showed that all biomarkers shared the same sensitivity value of 91.2% with a low specificity value, indicating a strong ability to identify non-survivors. Specifically, NLR, CRP, and PCT had a cut-off value of 1.72, 14.50 mg/L, and 0.115 ng/mL with a specificity of 14.9%, 26.8%, and 16.7%. These results showed that although inflammatory biomarkers were sensitive for detecting mortality, the low specificity limited standalone clinical utility (Table 2). The VIF values ranged from 1.004 to 1.052 for CRP, PCT, and NLR, indicating no evidence of significant multicollinearity among the biomarkers.
Diagnostic performance of inflammatory biomarkers for predicting mortality outcome.
| Biomarker | Cut-off value | Sensitivity | Specificity | AUC |
|---|---|---|---|---|
| NLR | 1.72 | 91.2% | 14.9% | 0.495 (95% CI 0.394–0.596) |
| CRP | 14.50 mg/L | 91.2% | 26.8% | 0.543 (95% CI 0.449–0.636) |
| PCT | 0.115 ng/mL | 91.2% | 16.7% | 0.466 (95% CI 0.367–0.564) |
Diagnostic accuracy of NLR, CRP, and PCT in predicting mortality outcomes. All three biomarkers demonstrated high sensitivity (91.2%), but low to moderate specificity. CRP showed the highest AUC, indicating slightly better discriminative performance compared to NLR and PCT. AUC: area under the curve; CRP: C-reactive protein; NLR: neutrophil-to-lymphocyte ratio; PCT: procalcitonin.
To further explore the prognostic significance of biomarkers, Kaplan-Meier survival analyses were performed (Figure 4).
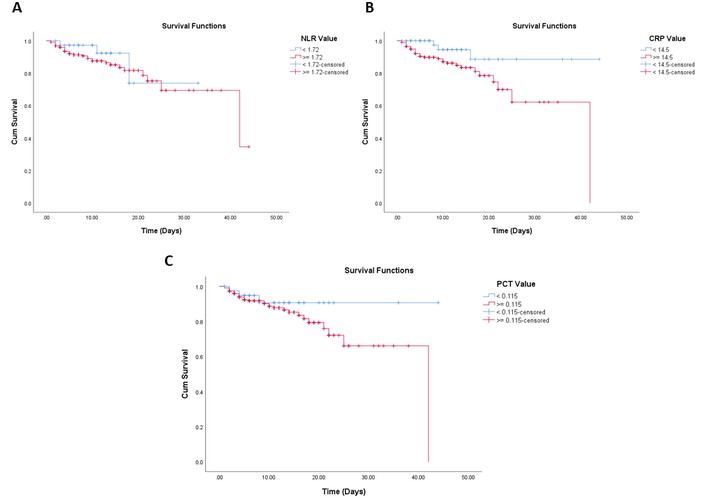
Kaplan-Meier survival curves based on NLR, CRP, and PCT values. Kaplan-Meier survival analysis illustrating the association between biomarker levels and patient survival over time. (A) Cumulative survival curves stratified by NLR, comparing patients with NLR < 1.72 and ≥ 1.72. (B) Survival analysis based on CRP levels, comparing patients with CRP < 14.5 mg/L and ≥ 14.5 mg/L. (C) Survival curves based on PCT levels, with patients grouped into < 0.115 ng/mL and ≥ 0.115 ng/mL. CRP: C-reactive protein; NLR: neutrophil-to-lymphocyte ratio; PCT: procalcitonin.
Patients with a lower NLR (< 1.72) had a mean survival time of 28.33 days (95% CI 22.97–33.68). Meanwhile, NLR patients with ≥ 1.72 had a mean survival of 34.24 days (95% CI 30.74–37.74). The difference in survival distributions between groups was not statistically significant (log-rank test: χ2 = 0.632, p = 0.427).
Based on the results, patients with lower PCT levels (< 0.115 ng/mL) showed a mean survival time of 40.39 days (95% CI 36.42–44.35), compared to 32.85 days (95% CI 29.33–36.36) in those with higher levels (≥ 0.115 ng/mL). However, the difference was not statistically significant (log-rank test: χ2 = 1.592, p = 0.207).
CRP showed a significant impact on survival. Based on the results, patients with lower levels (< 14.5 mg/L) had a longer mean survival time of 40.40 days (95% CI 36.39–44.41) compared to those with higher levels (≥ 14.5 mg/L) at 31.85 days (95% CI 27.82–35.87). The log-rank test showed a statistically significant difference between the two groups (χ2 = 5.555, p = 0.018), suggesting that high CRP levels were associated with poorer survival outcomes.
This study aimed to assess the prognostic value of inflammatory biomarkers, namely CRP, PCT, and NLR, in predicting IHM among elderly women with CAP. The results showed that most elderly women had mild pneumonia (83.2%), with a high survival rate of 87.0%. The median age was 66 years, and most were treated in general wards (93.5%).
PSI showed only a weak positive correlation with NLR, but no significant association with CRP or PCT. Although several reports have reported the use of NLR in predicting pneumonia severity [8], the weak correlations between PSI scores and inflammatory biomarkers in this study show the predominance of mild CAP cases. The negative correlations observed between NLR and both CRP and PCT were unexpected. To assess the influence of extreme values, a sensitivity analysis excluding NLR values above the 99th percentile (n = 260) was performed. The inverse correlations between NLR and CRP (r = −0.147, p = 0.017), as well as CRP and PCT (r = −0.174, p = 0.005) remained but were weaker, indicating partial distortion by outliers without fully explaining the unexpected inverse trends. This showed the dynamic immune responses in elderly patients, such as immunosenescence [9–12].
NLR shows different expression patterns depending on the underlying infection and clinical context. For example, NLR is significantly higher in post-stroke pneumonia but does not reliably predict other infections such as urinary tract infection, sepsis, or ventriculitis, indicating that the prognostic value is context-specific [13]. Additionally, NLR levels are lower in pulmonary tuberculosis compared with bacterial CAP, suggesting pathogen-related variability in immune responses [14].
Although PCT and CRP showed a moderate positive correlation, the single or combined use of both biomarkers had a strong discriminatory power for predicting mortality based on ROC curve analysis. Among the three biomarkers, CRP had the highest, but still modest, AUC (0.543). The Kaplan-Meier survival analysis showed that only CRP, at a cut-off of 14.5 mg/L, significantly impacted survival. In comparison, NLR and PCT cut-off values did not show statistically significant differences in survival outcomes. Due to the heterogeneity of pneumonia etiology and comorbidities in elderly women, several factors can reduce the predictive performance of NLR and PCT. Therefore, interpretation of these biomarkers, particularly NLR, should consider pathogen type and patients’ condition, rather than assuming uniform prognostic utility in all CAP cases.
The results showed that all biomarkers had high sensitivity (91.2%) in identifying non-survivors. However, specificity was limited, with CRP showing 26.8%, NLR 14.9%, and PCT 16.7%, suggesting limited utility as a standalone predictive tool. CRP was significantly associated with survival outcomes, suggesting potential application as an adjunct in risk stratification. Meanwhile, the combined model of CRP, PCT, and NLR did not show a significant improvement in predictive accuracy, with an AUC of 0.538 (95% CI 0.432–0.644). The results show the complexity of predicting mortality using biomarkers alone and the need for a more integrated method. The weak discriminatory performance in this study can be attributed to the mild severity of most cases and the low mortality rate (34 of 262; 13.0%).
This study correlates with existing literature that shows the limitations of using inflammatory biomarkers in isolation for CAP mortality prediction [15–17]. Previous reports have shown similar challenges with biomarkers like CRP and PCT, which are sensitive but often fail to offer sufficient specificity as reliable stand-alone prognostic tools [18, 19]. This issue is particularly observed in elderly populations, where comorbidities and multiple sources of inflammation can confound biomarker readings [20]. Despite the limitations, CRP, PCT, and NLR remain attractive due to their low cost, availability, and ease of use, particularly in low-resource settings [21, 22].
One of the key strengths of this study is the focus on elderly women. By concentrating on the demographic, the results contribute to a growing body of literature that seeks to understand how biomarkers and clinical management differ across genders in elderly patients. Gender-specific factors, such as immune responses and hormonal influences, can play a significant role in the presentation and response of elderly women to pneumonia [3].
CRP, PCT, and NLR are readily available in most clinical settings, serving as reliable tools in resource-limited environments. The cost-effectiveness of these biomarkers, combined with ease of use, indicates the essential role in early risk stratification, particularly in low- and middle-income countries [21]. However, several limitations in terms of specificity suggest that CRP, PCT, and NLR should be used as part of a broader clinical assessment, rather than standalone tools for mortality prediction.
This study has several limitations, which include the use of a retrospective design, hindering causal inferences, and introducing selection bias. The samples include predominantly mild cases, reducing the ability to detect biomarker differences in severe disease. Furthermore, PCT, CRP, and NLR were available to the treating physicians during hospitalization. This suggests potential influence of treatment intensity, such as antibiotic escalation and intensive care unit (ICU) referral, in reducing mortality risk. Another limitation is that microbiological testing was not routinely performed, hindering stratification of pneumonia etiology (bacterial, viral, or mixed). Finally, this study depends on single-time-point measurements of inflammatory biomarkers, which can be overcome through serial measurements to provide better prognostic insight.
In conclusion, CRP shows modest prognostic value in elderly women with CAP, but the limited specificity underscores the need for more comprehensive risk models. Consequently, further studies should explore the interplay of age, gender, and immune response to improve outcomes in elderly women.
AUC: area under the curve
CAP: community-acquired pneumonia
CRP: C-reactive protein
HCU: high care unit
ICU: intensive care unit
IHM: in-hospital mortality
NLR: neutrophil-to-lymphocyte ratio
PCT: procalcitonin
PSI: pneumonia severity index
ROC: receiver operating characteristic
VIF: variance inflation factor
WBC: white blood cell
ID and IN: Conceptualization, Writing—review & editing, Investigation, Visualization, Funding acquisition. DRN: Data curation, Formal analysis, Writing—review & editing. RR: Formal analysis, Writing—original draft, Writing—review & editing, Visualization. DLT: Supervision, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that there are no conflicts of interest.
This study was approved by the Health Research Ethics Commission, Faculty of Medicine, Hasanuddin University (No. 670/UN4.6.4.5.31/PP36/2023). This study complies with the 2013 Declaration of Helsinki.
Informed consent to participate in the study was obtained from all participants.
Not applicable.
Data supporting the results of this study are included in the manuscript. Additional information is available from the corresponding author upon reasonable request.
This study was supported by the BLU (Public Service Agency) fund of RSUP Dr. Wahidin Sudirohusodo (No. HK.02.03/DXIX/23369/2024). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 1500
Download: 26
Times Cited: 0