 Systematic Review
Systematic Review

Affiliation:
1Department of Cellular and Molecular Medicine, Rush University, Chicago, IL 60612, USA
Affiliation:
2Department of Pharmacy Practice, Retzky College of Pharmacy, World Health Organization Collaborating Centre for Traditional Medicine, University of Illinois at Chicago, Chicago, IL 60612, USA
3Department of Pharmaceutical Microbiology, University of Ibadan, Ibadan 200005, Nigeria
ORCID: https://orcid.org/0000-0001-8106-3086
Affiliation:
3Department of Pharmaceutical Microbiology, University of Ibadan, Ibadan 200005, Nigeria
ORCID: https://orcid.org/0000-0001-9096-2235
Affiliation:
4Federal Neuropsychiatric Hospital, Abeokuta 110121, Nigeria
Affiliation:
2Department of Pharmacy Practice, Retzky College of Pharmacy, World Health Organization Collaborating Centre for Traditional Medicine, University of Illinois at Chicago, Chicago, IL 60612, USA
Email: Mahady@uic.edu
ORCID: https://orcid.org/0000-0003-1820-5963
Explor Endocr Metab Dis. 2026;3:101474 DOI: https://doi.org/10.37349/eemd.2026.101474
Received: February 17, 2026 Accepted: May 08, 2026 Published: May 27, 2026
Academic Editor: Viduranga Y. Waisundara, Australian College of Business & Technology—Kandy Campus, Sri Lanka
Background: Diabetes mellitus (DM) refers to a group of metabolic diseases characterized by reduced insulin synthesis and release, leading to hyperglycemia, oxidative stress, and inflammation. The prevalence of DM continues to increase worldwide, primarily driven by type 2 DM (T2DM). While numerous prescription drugs are widely available for the management of T2DM, these treatments must be coupled with significant changes in diet and lifestyle to have long-term effects. This comparative review aims to summarize and critically evaluate some of the dietary antioxidant and anti-inflammatory functional foods (FFs), including bioactive compounds on glycemic regulation, oxidative stress, inflammatory markers, and other outcomes in T2DM patients.
Methods: A comprehensive literature search was performed from June 2014 to December 2025 in Cochrane Library, Embase, Google Scholar, PubMed/Medline, and Scopus databases.
Results: Thirty-one meta-analyses describing the effects of specific FFs on glycemic outcomes, including fasting blood glucose, HbA1c, insulin levels, insulin resistance, oxidative or inflammatory stress, and/or the doses needed to achieve these endpoints, in T2DM patients were included. Comparative analyses of the data for green tea in T2DM showed significant antioxidant effects, but conflicting data for glycemic regulation, and no significant effect on inflammatory markers. Flaxseed products significantly reduced oxidative stress and HbA1c but had no anti-inflammatory effects. Both anthocyanins and resveratrol from fruits and vegetables significantly reduced fasting blood glucose, HbA1c, as well as oxidative and inflammatory markers. Turmeric and curcumin significantly reduced fasting blood glucose, but the data for ginger were conflicted. In T2DM patients, turmeric and ginger significantly reduced markers of oxidation and inflammation.
Discussion: Overall, improvements in diet, including the incorporation of specific FFs and exercise, along with standard treatments, may be cost-effective methods to reduce the public health impact of T2DM. Limitations included the significant heterogeneity, high risk of bias, and low to moderate quality of the randomized controlled trial (RCT).
According to the World Health Organisation (WHO), the number of adults currently living with diabetes mellitus (DM) is ~828 million, an increase of 630 million since 1990 [1]. The global prevalence of DM has quadrupled, driven by increased cases of Type 2 DM (T2DM) that are associated with aging, obesity, and poor lifestyle choices [1–5]. The largest increases in T2DM were observed in the Caribbean, Central America, Middle Eastern countries, North Africa, and Southeast Asia [1]. Increasing T2DM rates lead to higher morbidity and mortality, straining healthcare systems, especially in low- and middle-income nations [1–5]. Therefore, there is an urgent need for inexpensive preventative and therapeutic interventions to treat T2DM, along with better global access to healthcare [2–5].
DM refers to a group of metabolic diseases characterized by reduced insulin synthesis and release, leading to hyperglycemia, oxidative stress, and inflammation [1–5]. According to the National Institutes of Health, there are many types of DM, including T1DM, T2DM, maturity-onset diabetes in young adults, and others [6]. T1DM is a genetic autoimmune disorder in which the immune system attacks and destroys the insulin-producing pancreatic β-cells, leading to little or no insulin production [7–9]. The disease presents in children and adolescents and is treated normally with daily insulin injections [7–9]. T2DM patients have reduced levels of insulin production and secretion, as well as insulin resistance (IR) due to β-cell dysfunction. It usually presents in middle-aged and older adults and is often associated with aging, obesity, and lack of exercise [10]. Genetics and lifestyle have also been reported to have a primary role in T2DM, as these patients often have at least one parent with the disease [10].
The current prevalence of T2DM in the USA is ~9% of adults over the age of 18, but this increases to ~25% in adults over the age of 65 [11]. However, in recent years, the prevalence of T2DM in younger populations has risen due to the increased incidence of obesity and lack of exercise in adolescents [11]. The International Diabetes Federation estimates the global prevalence of DM will continue to increase, most significantly in low to middle-income countries [12]. Ethnicity also plays a role in the prevalence, as T2DM is up to 6 times more common in African Americans, First Nation populations, and Hispanic populations in comparison to Caucasians [13]. While genetics and ethnicity play a role in the development of T2DM, lifestyle and environmental factors also greatly increase the risk of T2DM [14, 15].
Both T1DM and T2DM are a result of impaired insulin biosynthesis, secretion, or action [16–18]. Insulin biosynthesis begins in the endoplasmic reticulum (ER) of the pancreatic islet β-cells and is an orchestrated multistep process involving the ER-resident protein-folding complex comprised of chaperones, glycosylating enzymes, and oxidoreductases [16]. Proinsulin is an inactive prohormone polypeptide produced in the pancreatic β-cells and is formed by the cleavage of pre-proinsulin. Proinsulin is required for the proper folding of insulin and is converted to mature insulin through the effects of two endoproteases, the prohormone convertases PC2 and PC3, and carboxypeptidase H. These enzymes remove the C-peptide and four basic amino acids, leaving the insulin A- and B-chains linked by disulfide bonds [18]. For proper synthesis and function of insulin, correct folding of the proinsulin peptide is critical, and misfolding of this protein may lead to the accumulation of proinsulin. Increased levels of proinsulin in the β-cells increase ER stress, resulting in β-cell dysfunction, protein unfolding, loss of β-cell mass, reduced production of insulin, and ultimately diabetes [17]. T2DM is distinguished from T1DM by the loss of insulin-producing pancreatic β-cell mass and function over time. In addition, IR is another primary feature of T2DM as the cells in muscles, fat, and liver tissues no longer respond properly to insulin, leading to increased insulin production in the pancreas. When the pancreas can no longer maintain the increased insulin need, high blood sugar levels occur [16, 17].
The loss of β-cell mass and function is commonly attributed to increased β-cell apoptosis, leading to a continuous loss of β-cells and insulin deficiency [16, 17]. Pancreatic β-cell apoptosis is triggered by chronic metabolic stress and inflammation, through both intrinsic and extrinsic apoptotic pathways [16, 17]. Genetics, hyperglycemia, hyperlipidemia, and oxidative stress all contribute to chronic ER stress in pancreatic β-cells, as well as protein misfolding or unfolding of proinsulin [19, 20]. The unfolded protein response (UPR), a highly conserved canonical pathway that allows β-cells to adapt and survive by restoring homeostasis, is activated by protein unfolding [19, 20]. In cases of ER stress, the UPR reduces protein synthesis, increases protein folding, and enhances the degradation of damaged proteins to restore homeostasis (Figure 1). However, during prolonged ER stress, the UPR induces apoptosis to remove damaged cells by activating stress sensors in the ER. These sensors include the activating transcription factors 4 and 6 (ATF4 and 6), inositol-requiring enzyme 1α (IRE1α; ERN1 gene), and pancreatic ER kinase (PERK; EIF2AK3 gene) [21–23]. IRE1α detects misfolded proteins, activates, and splices XBP1 mRNA, leading to transcription of chaperones and ER-associated degradation components. PERK phosphorylates eIF2α to rapidly inhibit general protein translation to reduce the stress load and activate ATF4, which promotes chaperone production and stress response genes [21–23]. ATF6 releases transcription factors that increase the production of chaperones and other ER-resident proteins. While initially protective, the UPR allows β-cells to adapt and survive, but during increased insulin demand and chronic stress in prediabetes, UPR signaling upregulates pro-apoptotic signals, leading to significant β-cell apoptosis, the loss of pancreatic β-cells, and reduced insulin synthesis (Figure 1) [21–24]. Thus, the UPR plays a role in T2DM pathology and is associated with the development of IR [21–24]. Conversely, when ER stress is reduced, the UPR enables the cells to return to normal protein homeostasis, thereby reducing β-cell dysfunction and apoptosis. These data suggest that T2DM symptoms may be reversed by reducing reactive oxygen species (ROS) generation, ER stress, and the UPR in pancreatic β-cells.
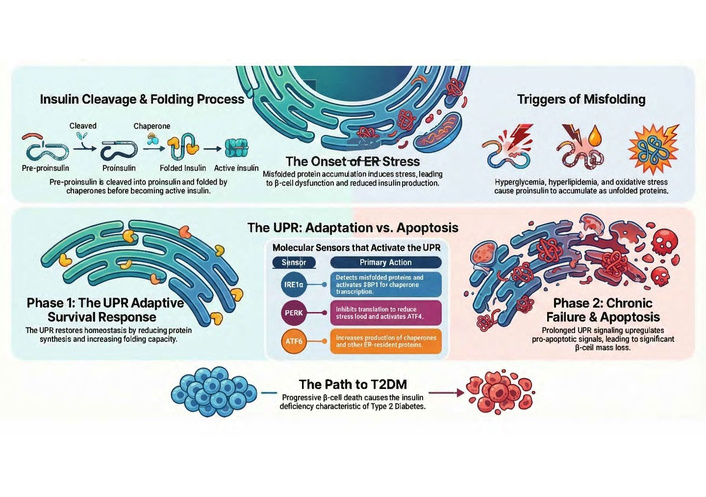
Pancreatic β-cells normally process millions of proinsulin molecules per day. When this process becomes dysregulated due to hyperglycemia, hyperlipidemia, or excessive production of ROS, proinsulin becomes misfolded, activating the UPR. The UPR is a canonical signaling pathway that is a protective mechanism in β-cells, allowing them to adapt and survive during hyperglycemia and increased insulin demand in prediabetes. However, prolonged or excessive UPR activation shifts to pro-apoptotic signals, contributing significantly to β-cell apoptosis, loss of β-cell mass, and reduced insulin synthesis in both T1DM and T2DM. ER: endoplasmic reticulum; ROS: reactive oxygen species; T2DM: type 2 diabetes mellitus; UPR: unfolded protein response.
Chronic oxidative stress leads to excessive, prolonged ROS formation and cellular damage that eventually activates immune-mediated inflammation, including the interleukin 6 (IL-6), C-reactive protein (CRP), and tumor necrosis factor-α (TNF-α) [25]. Chronic ROS generation in T2DM is also linked with obesity, hyperglycemia, and enhanced IR. IR leads to impaired glucose transport and increased release of glucagon from the liver, further adding to hyperglycemia and ROS production. Prolonged hyperglycemia induces the nonenzymatic glycation of proteins and lipids, which is measured using the glycated hemoglobin (HbA1c) test. HbA1c is a blood test measuring average blood sugar levels over the past 2–3 months and is used as a diagnostic tool to diagnose and monitor the progression of prediabetes and T2DM. A suggested normal result is < 5.7%, while the range of 5.7–6.4% suggests prediabetes, and 6.5% or higher is a diagnosis of diabetes [25]. Excessive glycation can eventually damage small blood vessels in the retina, kidney, and peripheral nerves that can induce vascular complications of T2DM, such as heart disease, kidney disease, peripheral neuropathy, and retinal changes [25]. Thus, lifestyle changes are an essential part of the therapeutic regimen for T2DM patients, and should include weight loss, a nutrient-dense diet, and an exercise program to decrease oxidative stress and inflammation and prevent some of these chronic sequelae. While prescription anti-diabetic medications, such as metformin and glucagon-like peptide 1 (GLP-1) agonists, are effective and reduce both hyperglycemia and inflammation in T2DM, these patients still require significant diet and lifestyle modifications.
Since T2DM is associated with reversible lifestyle factors, positive interventions such as improvements in nutrition and exercise, along with traditional treatments, can improve health and reduce long-term consequences in a cost-effective manner [26–29]. Numerous preclinical and randomized controlled trials (RCTs) have reported that the addition of specific antioxidant and anti-inflammatory functional foods (FFs) or their bioactive compounds can have beneficial effects on T2DM by reducing hyperglycemia and the chronic effects of oxidative stress and inflammation [30–40]. Some of these FFs have been shown to suppress oxidative and inflammatory damage to healthy cells, tissues, and organs to restore homeostatic balance over time [35–40]. Thus, considering that ER stress and oxidation play a significant role in the pathology of T2DM, the inclusion of dietary FFs and their bioactive compounds may have antioxidant effects and increase ER function in pancreatic β-cells, thereby reducing hyperglycemia and inflammation.
The debate on what constitutes an FF is currently ongoing, as the US Food and Drug Administration (FDA) has not proposed a formal definition for these products, and they remain poorly regulated [41]. The term “functional food” is not new, as it originated in Japan in the 1980s and describes foods regularly consumed for enhanced health, immunity, and disease prevention [42–44]. More recently, FFs were broadly defined as whole, enhanced, fortified, or improved foods that, when consumed regularly, at sufficient levels as part of a healthy diet, provide therapeutic advantages beyond basic nutrition [42–44]. In 2018, FFs were defined as: “natural or processed foods that contain biologically active compounds which, in defined, effective, and non-toxic amounts, provide clinically proven and documented health benefits utilizing specific biomarkers for the prevention, management, or treatment of chronic disease or its symptoms” [42–45]. This broader definition of FFs highlighted the importance of the pharmacological and molecular effects of bioactive compounds present in FFs, as well as the scientific and medical evidence that they provide the health benefits, beyond basic nutrition [42–44]. More recently, a 2022 publication defined FFs as “novel foods that have been formulated so that they contain substances or live microorganisms that have a possible health-enhancing or disease-preventing value, and at a concentration that is both safe and sufficiently high to achieve the intended benefit. The added ingredients may include nutrients, dietary fiber, phytochemicals, other substances, or probiotics.” [46]. This narrower definition highlights enhanced foods only, and as such would exclude normal food products such as fermented foods, including kefir and yogurt, as well as breakfast cereals with added vitamins and other similar food items [46]. This narrower definition focuses more on the addition of bioactive ingredients, at an appropriate level (dose), to normal food products to make them functional. Regardless of the definition, specific FFs and their bioactive components have clinical effects that extend beyond basic nutrition, supporting their role in the prevention and treatment of chronic diseases, including T2DM [42–47]. Considering the strong consumer interest in these products (current market ~$320 B/yr, with > 60% of US consumers using FFs), it makes good sense to clinically evaluate and promote the use of FFs when shown to be safe and effective [41].
For this review, we performed extensive literature searches for antioxidant and anti-inflammatory FFs with clinical efficacy in T2DM. Searches of numerous electronic databases, including the Cochrane Library, PubMed Central/Medline, Embase, Google Scholar, and the Scopus electronic databases, were performed from June 15, 2014, to December 15, 2025, without language restrictions, using relevant keywords in both free text and Medical Subject Headings (MeSH terms) format (Figure 2). The search databases were selected for their different but complementary capabilities. PubMed for its biomedical research coverage. Cochrane for its focus on systematic reviews and meta-analyses. Embase for its broad range of pharmacological studies and data. Google Scholar and Scopus for their grey literature and other non-indexed sources. The combination of these databases enables a more comprehensive and equitable retrieval of peer-reviewed research articles and meta-analyses. Terms used in specific searches of the scientific and medical literature are presented in the Supplementary materials. The Boolean search terms used included AND, OR, and NOT. Secondary literature searches were conducted in UIC repositories, books, abstracts, and websites. However, abstracts and conference proceedings were finally omitted, and only full-text peer-reviewed publications were included in the review. Inclusion criteria included peer-reviewed articles, English language, meta-analyses involving T2DM patients and FFs with oxidative and/or anti-inflammatory properties. Except for mechanistic studies to explain potential mechanisms of action, meta-analyses of animal and in vitro studies were excluded. Meta-analyses and systematic reviews that analyzed original RCTs, investigating flaxseed, green tea, turmeric/curcumin, anthocyanins (ACNs), resveratrol (RES), and ginger in T2DM patients were included. Excluded studies included meta-analyses of animal studies and in vitro studies, opinion pieces, and studies not in English or that did not connect FF ingestion with T2DM, oxidation, and/or antioxidant effects in these patients. A systematic method was used to extract the data from each study by two independent researchers. Disagreements about the data were resolved through consensus with a third researcher. The included meta-analyses were critically evaluated to verify their credibility, methods, and bias. The evaluation process included examining the methodology used, sample sizes, and data collection techniques. In addition, the quality of the included clinical trials, assessment of sources of bias, methods of statistical analysis, and reproducibility. Ultimately, 31 meta-analyses and systematic reviews that analyzed the clinical trials for ACNs and RES from fruits and vegetables, flaxseed, green tea, turmeric, and ginger in meta-analyses and systematic reviews of glycemic controls, effects on oxidative and inflammatory parameters in T2DM patients, as well as some preclinical studies describing molecular mechanisms of action were included. The available data that correlated the effects of these FFs on T2DM were critically analyzed, and a comparison analysis of these data was performed. Possible future directions for this research were also suggested. While this was not a registered PRISMA study, we followed PRISMA guidelines and have included a PRISMA-flow diagram to detail and track the study selection to improve transparency, reproducibility, and reduce bias for this review (Figure 2) [48]. All images, tables, graphs, and diagrams are original and drawn using Excel v16.1, NotebookLM, Adobe Creative Suite 2025, and modified using Photoshop 2025.
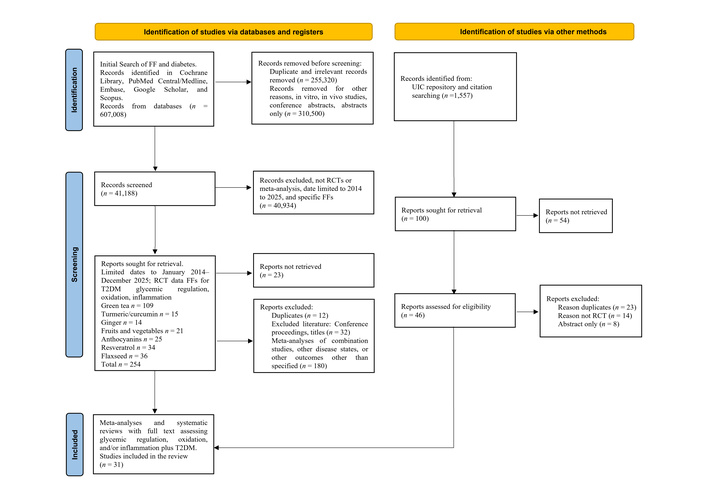
PRISMA systematic flow diagram [48] of the literature search process, including databases, number of publications (n), number of studies per category of functional food (meta-analyses), as well as inclusion and exclusion criteria. Initially, we found 607,008 studies (all formats) investigating FF in T2DM from all databases, that was then reduced to 254 randomized controlled trials of FF in T2DM patients from 2014 to 2025. This was further reduced to 128 meta-analyses, which were reduced after exclusion of irrelevant studies, meta-analyses of combination products, and studies that analyzed preclinical data (in vitro or in vivo studies) to 31 included meta-analyses. FF: functional food; RCT: randomized controlled trial; T2DM: type 2 diabetes mellitus. Adapted from [48]. © The Author(s) 2026. Licensed under a Creative Commons Attribution (CC BY 4.0).
As previously mentioned, oxidative stress, inflammation, and the UPR signaling pathway all play significant roles in reducing β-cell function and the development of T2DM. Regular consumption of specific FFs reduced oxidative stress, inflammation, and IR, as well as enhanced glucose regulation in T2DM patients [49, 50]. Some examples include fruits, leafy green vegetables, nuts, seeds (such as flaxseed), whole grains, dark chocolate, teas such as green tea, turmeric, ginger, yogurts, and fiber-added foods. These FFs contain specific bioactive compounds that reduce the production of free radicals and reduce oxidative stress and inflammation. In terms of clinical data, ACNs, flaxseed, ginger, green tea, turmeric/curcumin, and RES have all been investigated in numerous RCTs for the management of T2DM, and many of these studies have been analyzed in meta-analyses and systematic reviews [51–55]. These FFs and bioactive compounds were included in this systematic review.
Tea is the second most-consumed drink in the world, after water [56]. Globally, black tea makes up ~78% of the market, especially in Western countries. Green tea has ~20% of the market share, is used extensively in Asia, and is valued for its health benefits. Oolong and herbal teas (such as Hibiscus and Rooibos) make up smaller portions of the market [56]. Black, green, and Oolong teas are products of leaves of Camellia sinensis L. (Theaceae) but differ in the level of fermentation [57, 58]. Black tea is prepared by full fermentation of Camellia sinensis leaves, resulting in the formation of oxidized and polymerized chemical compounds that are responsible for the distinct flavors and aromas [57, 58]. Green tea is unfermented and thus retains most of its bioactive compounds, including catechins (polyphenols), caffeine, the amino acid L-theanine, methylxanthines (theobromine, theophylline), phenolic acids (gallic acid), vitamins (B2, C, E), and small amounts of carbohydrates and minerals due to minimal processing [58]. While teas have little nutritional value, they are rich in phytochemicals that have well-documented pharmacological activities for the management of chronic diseases [59–62]. The catechins are antioxidant compounds, of which epigallocatechin gallate (EGCG), catechin, epicatechin, and others make up ~30% of the dry weight of tea leaves [59–61]. These compounds have been extensively investigated for their antioxidant effects and for reducing oxidation and inflammation in preclinical studies [56, 57, 59]. EGCG and other tea catechins may manage T2DM symptoms by improving insulin sensitivity, reducing HbA1c levels and hyperglycemia, as well as decreasing oxidative stress. Numerous preclinical and clinical studies have reported that both black and green teas have protective effects against oxidative injury caused by excessive ROS generation [62–67]. EGCG was also reported to improve pancreatic β-cell function by reducing ROS-induced ER-stress and altering the UPR [63]. In cultured kidney podocytes, EGCG reduced oxidative ER stress caused by high glucose levels [64]. In a diabetic rat model, treatment with 80 mg/kg of EGCG reduced hyperglycemia and the expression of pro-inflammatory cytokines in the kidney [65]. EGCG also reduced UPR signaling by downregulating the expression of IRE1, ATF6, PERK, CHOP, XBP1, NLRP3, and caspase-1 [65]. Furthermore, Wu et al. [66] reported that EGCG treatment of ethanol-treated cultured βTC-6 and INS-1 pancreatic β-cells reduced CHOP expression and apoptosis, also suggesting the involvement of the UPR signaling pathway.
Along with preclinical studies, numerous RCTs have studied green tea in patients with prediabetes and T2DM. Over the past 10 years, five meta-analyses have evaluated these RCTs to assess the effects of green tea on glucose regulation in T2DM patients, as well as oxidation and inflammatory markers (Table 1, Figure 3) [67–71].
Results from five meta-analyses of RCTs evaluating the efficacy of green tea products on glycemic outcomes, oxidative and inflammatory markers in T2DM patients.
| Reference | Number of studies/patients included | Intervention/dosage form/doses | T2DM outcomes | Conclusions | Study limitations |
|---|---|---|---|---|---|
| Dehzad et al. [67] (2025) | 38 RCTs/n = 1,985 | Green tea extracts/infusions/200 mg/day (green tea extract) or 9 g/day (green tea leaves) | Supplementation significantly improved oxidative stress markers, including MDA, TAC, sulfoxide dismutase, and GPX levels in T2DM patients. No significant effects were observed on CRP, IL-6, or TNF-α. | Green tea reduced markers of oxidative stress. Green tea had no effect on inflammatory markers. | Significant heterogeneities in the RCTs, products used and patient characteristics. Included healthy patients, patients with prediabetes, T2DM and other disease states.Low to very low-quality studies included. RCTs on multiple disease states including T2DM. |
| Jia et al. [69] (2024) | 15 RCTs/n = 722 subjects | Green tea, caffeinated and decaffeinated tea/infusions and extracts | Supplementation significantly improved FBG and HbA1c. In T2DM patients, green tea supplements reduced the body mass index and IR. | Consumption of green tea improved FBG levels, HbA1c, and IR in T2DM patients. | Only analyzed the effect of green tea on the glycemic control indexes of T2DM patients, but no other parameters.Some of the extracted data was converted by software, which may have resulted in deviations from the original data.Significant heterogeneity as different green tea preparations were used, different intervention times, and doses were used. |
| Asbaghi et al. [68] (2021) | 14 RCTs/Not stated | Green tea/extracts and infusions/Not stated | Analysis found that green tea did not have a significant impact on FBG, fasting insulin levels, HbA1c, or HOMA-IR. | Green tea had no significant effects on parameters of glycemic control in patients with T2DM. | Significant heterogeneity in the patient populations, intervention duration, intervention times, and dosage. |
| Asbaghi et al. [70] (2019) | 8 RCTs/614 subjects | Green tea/extracts and infusions | Significantly reduced CRP but no significant effect on TAC and MDA. | Green tea consumption reduced CRP but did not reduce oxidative stress in T2DM patients. | A small number of clinical trials and subject included.Significant heterogeneity in intervention duration, intervention times, and dosage. |
| Wang et al. [71] (2014) | 7 RCTs/510 subjects | Green tea/ extracts and infusions | Results showed no statistical difference in FBG, serum insulin, 2-h plasma glucose tolerance test, HbA1c, or IR. | Supplementation with green tea did not decrease the levels of FBG, insulin, HbA1c, or other parameters in subjects at risk for T2DM. | A small number of clinical trials and patients were included in the analysis. Poor methodologies in some of the included RCTs. Significant heterogeneity in the intervention, dose, and study design. Data quality was graded as “very low to low” due to small sample sizes, short duration of treatment (4 weeks–6 months), and methodological deficiencies. Studies included in English and Chinese only. |
CRP: C-reactive protein; FBG: fasting blood glucose; GPX: glutathione peroxidase; HbA1c: glycated hemoglobin; HOMA-IR: homeostasis model assessment of insulin resistance; MDA: malondialdehyde; RCTs: randomized controlled trials; ROS: reactive oxygen species; SOD: superoxide dismutase; T2DM: type 2 diabetes mellitus; TAC: total antioxidant capacity.
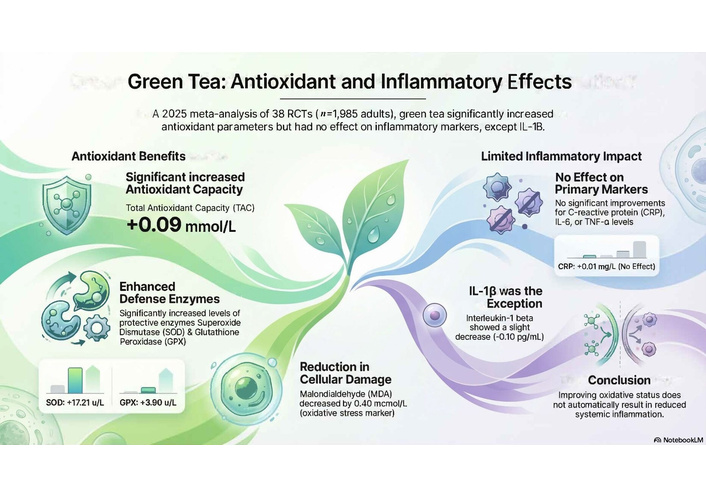
Anti-oxidant and anti-inflammatory effects of green tea. Results from the largest and most recent meta-analysis of 38 clinical trials showed that regular ingestion of green tea significantly reduced markers of oxidative stress, including MDA, TAC, and increased the activities of two antioxidant enzymes, SOD and GPX, that metabolize ROS [67]. While green tea purportedly had a small effect on IL-1β, no effect on other common inflammatory markers was observed. CRP: C-reactive protein; GPX: glutathione peroxidase; MDA: malondialdehyde; RCTs: randomized controlled trials; ROS: reactive oxygen species; SOD: superoxide dismutase; TAC: total antioxidant capacity.
The results of the largest and most recent meta-analysis involving 38 RCTs and 1,985 subjects concluded that green tea ingestion resulted in a significant reduction in malondialdehyde (MDA), a primary marker of lipid peroxidation in T2DM patients (Figure 3) [67]. Treatment also increased total antioxidant capacity (TAC), as well as the activities of superoxide dismutase (SOD) and glutathione peroxidase (GPX), two enzymes used to neutralize ROS. A pooled analysis of 19 of 38 RCTs showed that green tea supplementation did not significantly improve overall CRP levels or other markers of inflammation [67]. Similarly, green tea supplementation did not show a beneficial effect on the inflammatory markers IL-6 or TNF-α. Limitations of this meta-analysis include significant heterogeneity in the RCTs, high publication bias, and low to very low quality of evidence for the CRP data (Table 1). Furthermore, the long-term effectiveness of green tea appeared to be reduced after eight weeks [67].
In addition to this large study, four smaller meta-analyses included in Table 1 analyzed RCTs further analyzed the efficacy of green tea for the management of T2DM symptoms, and/or measured oxidative status and inflammatory markers. [68–71]. Overall, the conclusions of these meta-analyses were conflicting. Two of the meta-analyses [68, 71] found no significant effect on glycemic outcomes, while Jia et al. [69] found significant improvements in fasting blood glucose (FBG), HbA1c, and IR. Contradictory effects were reported for CRP, with one meta-analysis suggesting strong evidence [70], while another found none [67]. Other markers of inflammation, such as IL-6 and TNF, were not significantly reduced in any study, suggesting that green tea has limited effects on inflammation.
The effects of green tea on oxidative stress were also conflicting. One meta-analysis suggested that clinical evidence did not support a significant effect of MDA or TAC, and another found significant improvements [67, 70]. The discrepancies in these findings may be largely attributed to the methods used to perform the meta-analyses, as well as the quality of the RCTs included, variations in the health status of participants, variations in the biological assays used to measure markers, different green tea products and doses used, and treatment durations across the included clinical trials. Other issues include the type of green tea product and dose used in the RCTs, as green tea extracts have higher concentrations of catechins than green tea infusions, and may have significantly altered outcomes. Furthermore, the dose of green tea and the timing of biological assays appear to be critical, as some RCTs suggested that consumption of one to six cups of tea significantly increased the plasma antioxidant capacity in subjects ~1 h after consumption [62, 72].
Another common FF used for the management of prediabetes and T2DM is flaxseed [73]. Flax is an annual flowering plant known scientifically as Linum usitatissimum L. (Linaceae). Flaxseeds are nutrient-dense, ~40% oil by weight, of which ~55% is alpha linolenic acid (ALA). As an FF ingredient, flaxseed or flaxseed oil can be included in baked goods, yogurt, juices, muffins, pasta, and meat products [73, 74]. Flaxseeds contain numerous bioactive constituents, including dietary fibers, polyphenolic compounds, lignans, vitamins, and minerals (Figure 4). Some of these compounds, e.g., secoisolariciresinol diglucoside, have significant antioxidant, anti-hyperlipidemic, and antihyperglycemic effects in vitro and in vivo [75–77]. One preclinical study of rats with adenine and streptozotocin (STZ)-induced diabetes and chronic kidney disease showed that treatment with feed containing 15% w/w flaxseed powder significantly reduced inflammatory and oxidative biomarkers, including 8-isoprostane,8-hydroxy-2-deoxy guanosine, and IL-1β, IL-6, and NF-κ [75]. Flaxseed treatment increased renal TAC, the activities of SOD and catalase, as well as 8-hydroxy-2’-deoxyguanosine and 8-isoprostane, and reduced diabetes-induced kidney damage [75]. In another rodent study, flaxseed oil treatment of mice fed a high-fat diet (HFD) exhibited significantly reduced IR and inflammation, as well as improved lipid profiles [76]. Interestingly, ALA reduced ER-stress, as well as UPR and Jun N-terminal kinase (JNK) signaling in mouse liver. These in vivo studies suggest that flaxseed and flaxseed oil have antioxidant and anti-inflammatory effects in rodent models of diabetes that may explain some of the effects of flaxseed in human studies [76].
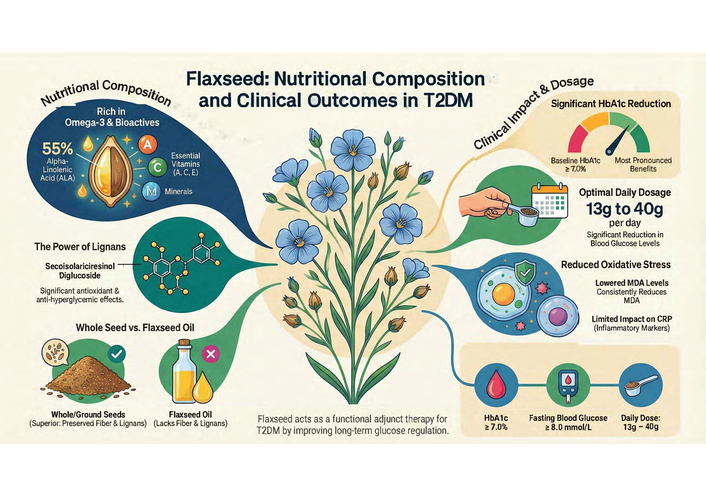
Flaxseeds are ~40% oil by weight, of which ~55% is composed of the omega-3-fatty acid, and alpha linolenic acid (ALA). Other phytochemical components include fibers, polyphenols, lignans (secoisolariciresinol diglucoside), vitamins (A, C, and E), and minerals. In clinical trials, flaxseed at a dose of 14–30 g/day reduced markers of oxidative stress and HbA1c, improved glycemic control, but had little effect on inflammatory markers. HbA1c: glycated hemoglobin; T2DM: type 2 diabetes mellitus.
Over the past 10 years, numerous meta-analyses have analyzed the RCTs for flaxseed products (whole, powdered, oil, and others), of which six have investigated the effects on symptoms, oxidative status, inflammation, and outcomes in T2DM patients. The results of these six meta-analyses are presented in Table 2.
Data describing the efficacy of flaxseed products on glycemic outcomes, oxidative and inflammatory markers in patients with T2DM from six meta-analyses of RCTs.
| Reference | Number of studies/patients included | Intervention/dosage forms | T2DM outcomes | Conclusions | Study limitations |
|---|---|---|---|---|---|
| Fornari Laurindo et al. [78] (2025) | 11 RCT (2 for flaxseed oil FO)/n = 203 | Flaxseed oil alone or in combination with other seed oils | Significant decrease in the oxidative stress marker MDA in T2DM patients. Flaxseed oil improved lipid profiles; however, FBG was not changed. | Reduced lipid levels and oxidative stress. However, no effects were observed on FBG levels. | A limited number of clinical trials and subjects were included.Significant heterogeneity in intervention duration, intervention times, and dosage form. Some studies analyzed a combination of flaxseed oil and other seed oils. |
| Musazadeh et al. [79] (2025) | 16 RCTs/n = 1,136 | Flaxseed/Flaxseed oil products | Significantly reduced BW and WC, but not BMI, blood pressure, TC, or TG in T2DM patients. | Flaxseed supplements reduced anthropometric indices and triglyceride levels, but blood pressure or lipids were not impacted. | A limited number of clinical trials and subjects were included.Significant heterogeneity in intervention duration, intervention times, dose, and dosage. |
| Xi et al. [80] (2023) | 13 RCTs/n = 1,720 | Flaxseed/flaxseed oil products | Significant reduction in HbA1c in T2DM patients. BMI, BW, BP, FBG, or HOMA-IR, quick insulin sensitivity check index, or lipid parameters were not changed. Sub-group analyses showed significant reductions in FBG if the baseline FBG was ≥ 8.0 mmol/L or baseline HbA1c ≥ 7.0%. Elevation in HDL-C and reduced TC and LDL-C were also significant. | Flaxseed supplementation significantly reduced HbA1c in participants with T2DM, especially those with poorly controlled blood sugar levels. | Many RCTs with a small number of subjects were included.Significant heterogeneity in the patient characteristics, flax products used, intervention duration, intervention times, and dosage.While the study showed an improvement in HbA1c in patients with T2DM, sensitivity analyses showed the result was not stable. The study included patients with stable blood glucose levels, that may have biased the study. High risk for publication bias was reported. |
| Villarreal-Renteria et al. [81] (2022) | 7 RCTs/n = 355 | Milled or ground flaxseed | FBG, HbA1c, HOMA-IR, and insulin levels were significantly reduced. | Overall improvement in glucose levels and reduced IR in prediabetes and T2DM patients. Effective doses not reported. | A small number of studies and subjects. High risk of bias as blinding in some RCTs was not optimal.Significant heterogeneity due to products used, patient population, and doses. |
| Mohammadi-Sartang et al. [82] (2017) | 25 RCTs/n = 2,592 | Flaxseed/Flaxseed products | Significant reduction in FBG and insulin levels, as well as HOMA-IR index. Supplementation raised the QUIKI. No effect on HbA1c. Sub-group analysis showed that these effects were significant only for whole or ground flaxseed but not flaxseed oils or lignan extracts. | Whole flaxseed supplements may improve glycemic control in patients with high FBG treated for more than 12 weeks. | While 17/25 studies were of high quality, most of the trials had small sample sizes, n < 30–50 participants. Significant heterogeneity among studies, different methodologies, and different populations. |
| Ursoniu et al. [83] (2017) | 17 RCTs/n = 1,256 | Flaxseed powder/extract/oil | No significant effect on CRP levels in T2DM patients. | Flaxseed supplementation does not alter CRP plasma levels. | A small number of clinical trials were analyzed. Some RCTs were of low quality. Significant heterogeneity between RCTs due to the wide range of supplement dosage forms and doses used. |
BMI: body mass index; BP: blood pressure; BW: body weight; CRP: C-reactive protein; FBG: fasting blood glucose; HbA1c: glycated hemoglobin; HDL-C: high-density lipoprotein cholesterol; HOMA-IR: homeostasis model assessment of insulin resistance; LDL-C: low-density lipoprotein cholesterol; MDA: malondialdehyde; RCTs: randomized controlled trials; T2DM: type 2 diabetes mellitus; WC: waist circumference; QUIKI: quantitative insulin sensitivity check index; TC: total cholesterol; TG: triglycerides.
Overall, meta-analyses presented in Table 2 show that flaxseed supplementation resulted in a significant reduction in MDA and/or lipid profiles [78], body weight [79], and glycemic outcomes [80–82], but had little effect on inflammation, as measured by CRP levels [83]. However, results across multiple meta-analyses showed a consistent impact on long-term glucose regulation. Significant reductions in HbA1c levels were observed, with one analysis reporting a standardized mean difference of –0.442, while another highlighted that the benefit was most pronounced in patients with baseline HbA1c ≥ 7.0%. Clinically, every 1% reduction in HbA1c levels can reduce the incidence of microvascular events by 37%. Conflicting data were reported for FBG results and insulin concentrations. Some studies showed significant reductions, while others reported no effect in the general T2DM population unless baseline FBG was high (≥ 8.0 mmol/L). Increases in the homeostasis model assessment of IR (HOMA-IR) were noted, but these may be inconclusive due to small sample sizes in individual RCTs. In terms of body weight, while the reductions were statistically significant, they were clinically modest. Whole or ground flaxseed was superior to flaxseed oil for weight loss and glycemic control. This was associated with the presence of fiber and lignans in the whole seed, which are largely absent in the oil. The trials utilized doses ranging from 10–100 g per day, where 13–40 g per day showed significant reductions in blood glucose. Doses of at least 13 g/day improved insulin concentrations and HOMA-IR in some studies. A dose of 30 g of flaxseed/day was associated with improved HbA1c when delivered in yogurt. These studies suggest that flaxseed may be a promising adjunct therapy for managing glycemic control and as an antioxidant in populations with prediabetes or T2DM. However, its effects on inflammatory markers such as CRP appear to be limited.
Fruits and vegetables have a central role in the human diet and are necessary for proper nutrition, and have been shown to reduce the incidence of chronic disease [84–86]. These benefits of fruits and vegetables have been shown to be due to their high levels of bioactive compounds (phytochemicals, vitamins, minerals, fiber), water and fiber content, and low levels of fat [84–86]. While the recommended number of daily servings varies from country to country, approximately 5 servings/day has been recommended by most national and international health organizations [84–86]. The United States Department of Agriculture (USDA) suggests 5 to 9 servings of fruits and vegetables per day, while the WHO suggests at least 400 g (5 servings) per day. Unfortunately, most populations do not meet these basic guidelines, and thus do not get sufficient nutrients, including potassium, vitamins, minerals, and fiber daily [87–89]. Thus, the increasing incidence of chronic diseases, including diabetes, is thought to be directly associated with poor dietary habits and poor nutrition due to a lack of fruits and vegetables.
In the broad sense, fruits and vegetables are important FFs, as ingestion of sufficient quantities has been shown to have preventative and therapeutic effects in numerous chronic diseases, including cardiovascular, cancer, hypertension, and T2DM [90–94]. The functional benefits of fruit/vegetable drinks, products, or extracts and their potential effects on diabetes are based on the presence of specific naturally occurring phytochemical compounds, including flavonoids, polyphenols, vitamins and minerals, phytoestrogens, and other compounds that act as antioxidants [95–97]. Many of the bioactive phytochemical compounds present in fruits and vegetables have a phenolic or polyphenolic structure, including the flavonoids [96, 97]. The flavonoids are a group of naturally occurring compounds, phenolic in nature, and are present in high concentrations in fruits, vegetables, and grains [97, 98]. More than 9,000 different flavonoid compounds have been identified and categorized into seven sub-groups based on modifications of their basic ring structure. These include the ACNs, catechins (flavan-3-ols), chalcones, flavones, flavanones, isoflavones, and flavonols [98]. ACNs/anthocyanidins are the water-soluble pigments that are responsible for the colors of berries, vegetables, red/black grapes, and red wine (Figure 5) [99–101]. There are > 500 ACNs and anthocyanidins (aglycones) of which the most common dietary compounds are cyanidin > malvidin > pelargonidin > delphinidin > petunidin > peonidin [102–104]. ACNs are reported to be the most highly consumed group of flavonoids in the US diet, with a daily estimated intake of 12 to 21 mg/day, which has significantly declined since 1976, when daily levels were as high as ~180 mg/day [99, 105].
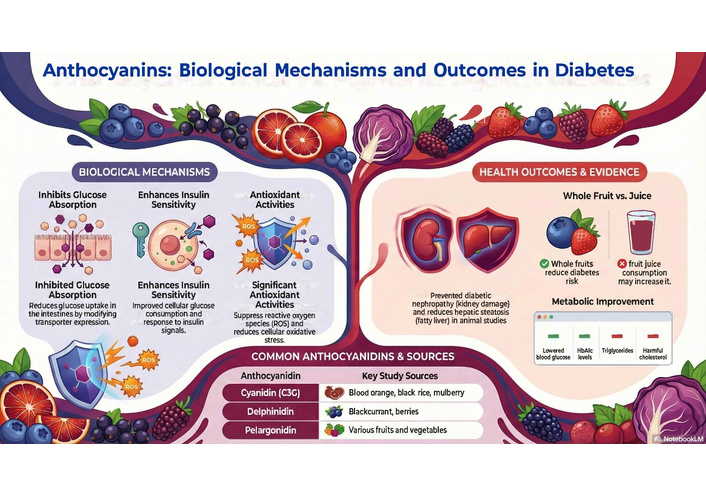
Sources of common anthocyanins (ACNs), biological mechanisms, and outcomes of common ACNs in T2DM. ACN supplementation significantly reduced oxidative stress and ROS generation, reduced fasting blood glucose levels and HbA1c, and improved insulin sensitivity as well as reduced nephropathy and hepatic steatosis in animal models. C3G: cyanidin-3-glycoside; T2MD: type 2 diabetes mellitus.
In terms of diabetes, ACN-rich fruits and pure ACNs have been extensively investigated for their effects in numerous preclinical and clinical studies. Searches for the antidiabetic, antioxidant, and anti-inflammatory effects of ACNs in numerous databases led to > 20,000 citations, mainly from the past 10 years. The pharmacological activities of the ACNs are due to the presence of multiple phenolic hydroxyl groups, which enable them to donate electrons to neutralize ROS and decrease oxidative damage caused by ROS accumulation (Figure 5) [106]. For example, delphinidin-3-glycoside (D3G), a component of blueberry, has five hydroxyl groups and superior antioxidant activities than either cyanidin-3-glycoside (C3G, 4 hydroxyl groups) or pelargonidin-3-glycoside (3 hydroxyl groups) [107–109]. In one preclinical study, a D3G-rich blueberry extract significantly reduced blood glucose levels in diabetic mice, increased antioxidant SOD activity, and improved insulin sensitivity [107]. In addition, cyanidin and delphinidin both reduced HFD-induced IR and inflammation, as well as altered redox signaling to reduce IR in high-fat-fed mice [109].
C3G and D3G also had significant anti-inflammatory effects and reduced TNF-α and NF-κβ, as well as promoted the regulation of Nrf2, a protein essential for protecting cells from oxidative stress and inflammation [110]. In terms of human studies, > 37 RCTs have assessed the effects of ACNs on glycemic control and other symptoms associated with T2DM. Many of these RCTs were meta-analyzed and systematically reviewed over the past 10 years, and Table 3 presents an overview of the results from six meta-analyses.
Results from six meta-analyses of ACNs from fruits and vegetables on glycemic indices, insulin resistance, hyperlipidemia, inflammation, and oxidation in patients with T2DM.
| Reference | Number of studies/patients included | Intervention/dosage form/dose | T2DM outcomes | Conclusions | Study limitations |
|---|---|---|---|---|---|
| Tiwari et al. [111] (2024) | 21 RCTs/not stated | ACN-rich foods, various sources/dose not stated | Results of clinical trials showed that ACN-rich foods significantly reduced the FBG, TC, HbA1c, and TG. | Consumption of ACN-rich foods improves blood glucose regulation and lipid levels in diabetic and obese subjects. | A low number of studies were included in the analysis. Many studies had an unclear risk of bias and were from China and the Middle East, suggesting that they may not be generalizable. |
| de Oliveira et al. [112] (2023) | 8 RCTs/n = 390 | Fresh or freeze-dried blueberries/dose not stated | The study showed no differences in BP, FBG, TC, LDL-C, ApoB, or HbA1c. Decreases in hs-CRP, IL-6. ROS and TNF were reported. | Administration of fresh or frozen whole berry products had no significant effect on diabetic parameters, except for reduced inflammation and oxidative stress markers. | Analyses only included papers in English or Spanish. Only included studies of whole fruits. Many studies included a high risk of bias. |
| Mao et al. [113] (2023) | 13 RCTs/n = 703 T2DM | ACN-rich extracts/supplements/ 320 mg/day | A study reported that a median ACN dose of 320 mg/day from concentrated fruit extracts or powders significantly reduced FBG, HbA1c, TG, and LDL-C. No significant difference was seen in insulin levels, HOMA-IR, TC, HDL-C, or BP. | Significant improvements in glycemic parameters and lipid profiles in patients with T2DM. Concluded that ACNs in fruit extracts or powders were useful in T2DM, to reduce lipiddisorders and resultant cardiovascular diseases. | A low number of studies and subjects were included in the analysis. More than half of the studies had an unclear risk of bias for allocation concealment. Many studies from China and the Middle East indicate that the study may not be generalizable. |
| Sandoval-Ramírez et al. [114] (2022) | 5 systematic reviews/meta-analyses/n = 2,314,336 and 8 RCTs/n = 4,984 | Various ACN-rich products/200 and400 mg/day | Supplementation with ACNs at doses between 200 and 400 mg/day significantly reduced both FBG (–5.58 mg/dL) and Hb1Ac (–0.65 units).In T2DM patients, doses of ACNs of 31.45 to 1,050 mg/day reduced the HOMA-IR. | Supplementation with ACNs improved lipid profiles, glycemic indices, and endothelial function, but had no effect on BP. | High heterogeneity between disease states, products, populations, and ACN doses. Umbrella reviews limitations include the restriction of the information, limiting the data that can be analyzed. |
| Fallah et al. [115] (2020) | 37 RCTs/n = 2,068 | Various ACN-rich fruit extracts and purified ACNs | Significant reduction in FBG, the 2-hour level PPG (2h-PPG), HbA1c, HOMA-IR, resistin, and PAI-1. No significant change in the levels of fasting insulin or CRP. | ACN supplementation for longer than 8 weeks at a high dose of > 300 mg/d significantly reduced levels of FBG, 2h-PPG, HbA1c, and HOMA-IR in patients with T2DM. | High heterogeneity as studies included different sources of ACN products, doses, and patient populations. Products also contained other active compounds that may have introduced bias into the study. |
| Araki et al. [116] (2021) | 22 RCTs based on ACN structure type/not stated | Cyanidin-, delphinidin-, or malvidin-based ACNs/wide range of products: juices, fruit, extracts, freeze-dried berries, purified ACNs | Significant reduction in LDL-C cholesterol by delphinidin-based ACNs. Increased HDL-C. No significant effect on fasting glucose levels, insulin levels, HbA1c, or HOMA-IR for any ACN. The insulin resistance index was reduced by cyanidin-based ACNs. | No significant effects on glucose levels, insulin levels, HbA1c, or HOMA-IR. TG, LDL-C, and HDL-C levels were significantly improved by delphinidin-based ACNs.Cyanidin-based ACN products showed improvements in TC and insulin resistance.Malvidin-based ACNs showed improvement only in HDL-C. | The clinical trials included had low to moderate qualities. Small number of participants, particularly for the individual ACNs trials. The effects of malvidin-based ACNs on glucose related parameters and of cyanidin-based ACNs on HbA1c was not determined due to insufficient data. |
ACNs: anthocyanins; BP: blood pressure; CRP: C-reactive protein; FBG: fasting blood glucose; HbA1c: glycated hemoglobin; HDL-C: high-density lipoprotein cholesterol; HOMA-IR: homeostasis model assessment of insulin resistance; LDL-C: low-density lipoprotein cholesterol; PAI-1: plasminogen activator inhibitor-1; PPG: postprandial glucose; RCTs: randomized controlled trials; T2DM: type 2 diabetes mellitus; TC: total cholesterol; TG: triglycerides.
Based on the reviewed meta-analyses from Table 3, dietary ACNs in a median dose of 320 mg/day for > 8 weeks had significant therapeutic effects in patients with T2DM. In terms of glycemic control, high-dose ACN supplementation significantly improved glycemic markers, including HbA1c (~0.31% reduction). Interestingly, complex ACNs from fruit extracts or powders were more effective in reducing HbA1c than purified ACN supplements. FBG was reduced by an average of ~0.63 mmol/L, which was significant. This effect appears to be independent of the intervention length or dosage (within the 4–24-week range). The 2h-PPG was also significantly reduced (~1.60 mmol/L). For IR, the results were conflicting, with some studies reporting significant reductions in HOMA-IR, while others found no effect on fasting insulin. In addition, ACN consumption showed significant improvements in lipid levels and reduced low-density lipoprotein cholesterol (LDL-C) and triglycerides (TG). Furthermore, ACNs significantly improved endothelial function and reduced oxidative and inflammatory markers. The antihyperglycemic activities of ACNs were associated with their antioxidant properties, their ability to inhibit carbohydrate-digesting enzymes, as well as their role in modulating glucose transporters.
In addition to ACNs, RES, a chalcone compound found in fruits, including red and black grapes, vegetables, and red wine, has significant antidiabetic, antioxidant, and anti-inflammatory activities in both preclinical and human studies [117–121]. RES (3,5,4’-trihydroxystilbene, Figure 6) is reported to have antioxidant, antibacterial, and anti-inflammatory activities, and may be of benefit for the management of cancer, osteoporosis, and DM, as well as other chronic disorders [120–125]. Administration of RES to obese, diabetic mice improved glucose levels and increased cellular glucose uptake by upregulating GLUT, a membrane glucose transporter that facilitates insulin-induced glucose uptake in muscle cells [126, 127]. Other studies in obese, diabetic mice showed that RES improved endothelial dysfunction, altered carbohydrate metabolism, and increased insulin secretion by activating adenosine monophosphate kinase (AMPK) and silent information regulator sirtuin 1 (SIRT1), by regulating downstream targets, including peroxisome proliferator-activated receptor (PPAR)-α/γ, PPAR-γ coactivator-1α (PGC-1α), and the forkhead transcription factor O1 (FOXO1) [128, 129]. In addition, mice with STZ-induced diabetes treated with RES showed increased insulin secretion by reducing pancreatic β-cell apoptosis [130]. Furthermore, RES exhibited significant antioxidant and anti-inflammatory effects and reduced ROS generation, increased SOD activities, and suppressed IL-1β, IL-6, and TNF-α expression and signaling (Figure 6) [131]. Thus, the preclinical data suggest that RES may have significant potential as a bioactive compound for the management of T2DM.
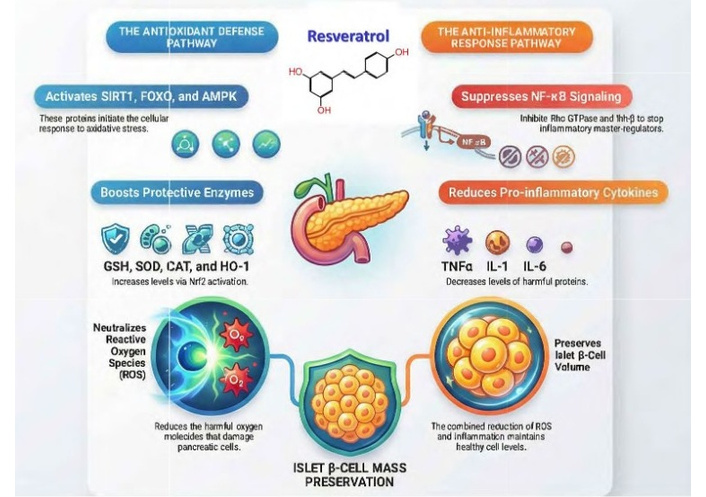
Resveratrol (RES), a functional food bioactive compound found in fruits and vegetables, is reported to have numerous effects in diabetes. In pancreatic β-cells, RES altered carbohydrate metabolism and increased insulin secretion by activating AMPK, SIRT1, and regulating downstream targets, PPAR-α/γ, PGC-1α, and FOXO1. RES treatment of streptozotocin-induced diabetic mice increased insulin secretion and reduced pancreatic β-cell apoptosis, thereby preserving β-cell mass. Furthermore, RES inhibited ROS formation, increased SOD activity, and reduced interleukin (IL)-1β, IL-6, and tumor necrosis factor α (TNF-α), showing significant antioxidant and anti-inflammatory effects. AMPK: adenosine monophosphate kinase; CAT: catalase; FOXO1: forkhead transcription factor O1; GSH: glutathione; HO-1: heme oxygenase 1; PGC-1α: PPAR-γ coactivator-1α; PPAR: peroxisome proliferator-activated receptor; SIRT1: sirtuin 1; SOD: superoxide dismutase.
In terms of human studies, data from RCTs have been meta-analyzed to determine the effectiveness of RES in the management of T2DM symptoms and its possible antioxidant effects. Three meta-analyses published in the past 10 years are included below in Table 4 [132–134].
Analyses of the systematic reviews and meta-analyses of the RCTs investigating the clinical outcomes of RES treatments in T2DM patients.
| Reference | Number of studies/patients included | Intervention/dosage form | T2DM outcomes | Conclusions | Study limitations |
|---|---|---|---|---|---|
| Zhu et al. [132] (2025) | 6 RCTs/n = 533 | RES/not stated | RES supplementation significantly reduced CRP, lipid peroxide levels, and oxidative stress score, and significantly increased GPX levels and catalase levels. No significant effects for IL-6, TNFα, superoxide dismutase levels, total antioxidant capacity, or MDA. | RES supplements had anti-inflammatory effects and reduced oxidative stress. score in T2DM patients. | A limited number of RCTs and a small sample size. Low-quality clinical trials were included in the analyses.Significant heterogeneity exists in the dose and intervention times for RES supplements varied widely.Many studies from Middle Eastern countries, that may reduce generalizability. No subgroup analyses performed. |
| Zhang et al. [133] (2021) | 15 RCTs/n = 896 | RES/300–500 mg/d | RES reduced the HOMA-IR, HbA1c, FBG, and fasting insulin levels, which were significantly different. No significant difference in HDL-C, MDA, TC, or TG levels. No significant difference in adverse events between RES and placebo. | RES supplementation may improve insulin resistance, lower fasting blood glucose and insulin levels, and improve oxidative stress in T2DM patients, but has no effect on lipid parameters. | Significant heterogeneity in the data and studies included.Some of the RCTs analyzed were of low methodological quality due to poor randomization methods or blinding. A small number of subjects in some studies. Significant variations in the dose range and duration of RES may have impacted the conclusion and introduced bias. |
| Gu et al. [134], (2022) | 19 RCTs/n = 1,151 | RES/300– > 1000 mg/d | In T2DM patients, high doses of RES (≥ 1000 mg) reduced FBG, SBP, and DBP. No significant effect was observed for waist circumference, TG, or HDL-C levels. | RES supplementation reduced SBP and DBP in T2DM patients. High dose RES reduced fasting blood glucose but had no significant effect on waist circumference, TGs, or HDL levels. | Significant heterogeneity for the subjects included variation in the dose range and duration of RES treatment. These may have impacted the overall conclusion. |
CRP: C-reactive protein; DBP: diastolic blood pressure; FBG: fasting blood glucose; GPX: glutathione peroxidase; HbA1c: glycated hemoglobin; HDL-C: high-density lipoprotein cholesterol; HOMA-IR: homeostasis model assessment of insulin resistance; MDA: malondialdehyde; RCTs: randomized controlled trials; RES: resveratrol; SBP: systolic blood pressure; T2DM: type 2 diabetes mellitus; TC: total cholesterol; TG: triglycerides.
Current clinical evidence from recent meta-analyses suggests that RES has significant therapeutic potential for the management of symptoms associated with T2DM [132–134]. Comparative analyses of the studies suggest that RES has clear dose-dependent benefits for glycemic control. High-dose RES (≥ 1000 mg/day) significantly reduced FBG, improved HOMA-IR, reduced HbA1c levels, and fasting insulin levels, all critical indicators of long-term glucose management. However, the studies also reported that doses of ≥ 1000 mg/day are required to achieve these effects, and doses < 1000 mg/day had no significant effect on FBG. RES treatment also significantly reduced both systolic (> 7 pt reduction) and diastolic (> 3 pt reduction) blood pressure, suggesting potential cardioprotective effects in T2DM patients. In terms of antioxidant and anti-inflammatory parameters, RES supplementation significantly reduced CRP levels and pro-inflammatory cytokines and reduced oxidation by decreasing lipid peroxides. RES also increased antioxidant enzyme activity (catalase and GPX). Thus, RES may be useful for reducing T2DM complications, including kidney and retinal damage. The meta-analyses also consistently showed that RES did not impact total cholesterol (TC), LDL-C, high-density lipoprotein cholesterol (HDL-C), or TG, and had no effect on waist circumference. Despite these benefits, the findings were often characterized by high heterogeneity across studies due to significant variations in dosage and treatment duration. Also limiting the conclusions were low patient numbers, low-quality clinical studies, and methodologies. Overall, RES was generally well-tolerated, with few adverse events reported as compared with placebo.
Herbs and spices have been used for millennia for the symptomatic management of many diseases, including diabetes [135]. Reviews of the pharmacological activities of these plants show that they contain multiple chemical constituents that have significant antioxidant and anti-inflammatory effects, reduce blood glucose levels, improve insulin secretion and function, as well as reduce diabetic retinopathy and neuropathy [136–138]. A virtual screening of 2,300 compounds from these plants against 18 known diabetes drug targets indicated that many herbs and culinary spices contained multiple bioactive compounds that impacted multiple targets, suggesting excellent potential for the management of T2DM [135].
Turmeric, known scientifically as Curcuma longa L., is a perennial flowering plant belonging to the Zingiberaceae (ginger family). The plant is native to India and Southeast Asia but is used worldwide as a culinary spice [138–140]. Known for its bright yellow-orange-colored rhizomes, turmeric has an earthy, slightly bitter, peppery flavor and is commonly used in Indian, Middle Eastern, and Caribbean cuisines [138–140]. While the major components of the rhizome are the curcuminoids, including curcumin, dimethoxy-curcumin, and 5’-methoxycurcumin, with curcumin being the primary compound, and making up ~77% of the rhizomes [141].
Beyond its use as a spice, turmeric and the curcuminoids have antioxidant and anti-inflammatory activities, and have been extensively studied for their anticancer, antiobesity, and antidiabetic effects [139–143]. The medical use of turmeric dates back almost 4,000 years and was described in Sanskrit medical treatises, as well as Ayurvedic and Unani systems of medicine [139, 140]. Many published preclinical studies have shown that turmeric has anti-diabetic activities and reduced diabetes-induced oxidation in rodent models [144–147]. In rats with STZ-induced diabetes, 0.5% of turmeric added to chow decreased oxidative stress and increased antioxidant enzyme activities [144]. In another study, reduced serum glucose concentrations were reported in STZ-diabetic mice treated with an ethanol extract of turmeric (0.2–1.0g/day) [145]. A recent 2024 study in STZ-induced diabetic mice reported that treatment with purified curcumin (50 mg/kg body weight) reduced the serum glucose, creatinine, and urea levels, as well as TG and TC. In addition, curcumin had significant effects on oxidative status and inflammatory markers, and increased MDA, and reduced IL-6 and TNF-α levels. However, curcumin was not as effective as the glibenclamide positive control [146]. Mechanistically, curcumin inhibited the stress-response PERK-eIF2α-ATF4 and UPR signaling pathways, thereby reducing oxidative damage [147]. Thus, curcumin has anti-inflammatory effects by reducing NF-κ and inhibiting the expression of inflammatory cytokines. These activities reduce ER stress by downregulating UPR by suppressing signaling through PERK-eIF2α-ATF4 in vivo [147–149].
In terms of human studies, numerous RCTs, meta-analyses, and reviews have investigated the efficacy of turmeric/curcumin in T2DM (Figure 7). For diabetes, approximately fifteen meta-analyses have been published in the last 10 years, of which five of the most recent, which included antioxidant and anti-inflammatory data for turmeric/curcumin products, are presented in Table 5.
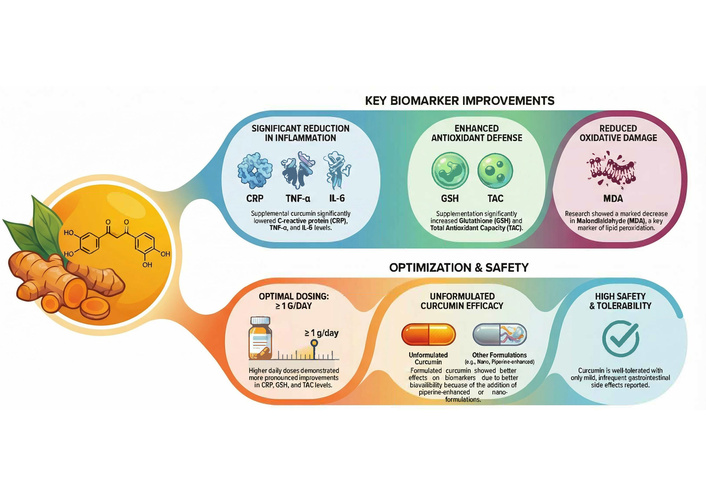
Turmeric/curcumin improved key biomarkers in T2DM patients; however, this was dose and formulation-dependent. Turmeric and curcumin reduced inflammatory parameters and increased antioxidant markers, as well as reduced oxidative damage in T2DM patients. Optimal doses were > 1 g/day, and the newer formulated products containing piperine or nano-formulations had better efficacy than the unformulated products due to better bioavailability. Turmeric/curcumin has high tolerability and a good safety profile. CRP: C-reactive protein; GSH: glutathione; MDA: malondialdehyde; T2DM: type 2 diabetes mellitus; TAC: total antioxidant capacity.
Meta-analyses of the RCTs for turmeric/curcumin supplements and their effects on glycemic indices, inflammatory markers, and oxidative stress in T2DM patients.
| Reference | Number of studies/patients included | Intervention/dosage form/dose | T2DM outcomes | Conclusions | Study limitations |
|---|---|---|---|---|---|
| Kehinde et al. [150] (2025) | 104 RCTs/n > 6,500 | Turmeric/curcumin/various dosage forms and doses | Significantly reduced FBG, HbA1c, TG, and LDL-C. Increased HDL-C and TAC. In addition, inflammation was reduced, including CRP and IL-6, in T2DM patients. | Supplementation of T2DM patients with turmeric/curcumin improved glucose regulation and lipid metabolism and reduced inflammation and oxidative stress. | Some studies had small sample sizes. Most studies from the Middle East or India, so generalizability may be an issue.Significant heterogeneity among the studies in terms of products used, disease severity, and methodological quality. Some studies had issues with randomization, nonadherence to planned interventions, and missing outcomes. |
| Bahari et al. [151] (2025) | 28 RCTs/not stated | Turmeric/curcumin/various dosage forms and doses | Significantlyreduced markers of inflammation and oxidative stress, such as CRP, TNF-α, IL-6, and MDA. Increased glutathione and TAC. Higher doses (≥ 1 g/day) and unformulated curcumin showed better effects. | Turmeric/curcumin supplementation reduces inflammatory and oxidative stress biomarkers in prediabetes and T2DM patients. Favorable safety profile. | Studies included were relatively small in sample size, short duration, and geographically concentrated.High heterogeneity, signs of publication bias, and the reliance on surrogate biomarkers rather than clinical endpoints. |
| Marton et al. [152], (2021) | 16 RCTs/n = 1,309 | Turmeric/curcumin/various dosage forms and doses (80 –2,100 mg/day) | Significantly reduced lipid peroxidation, FBG levels, HbA1C, TG, TC, LDL-C, CRP, systolic, and DBP. Significantly increased HDL-C levels and serum antioxidant capacity were also found. | Turmeric/curcumin supplementation improved FBG, HbA1c, insulin resistance, lipid profiles, and reduced inflammationbiomarkers in T2DM patients. | A limited number of databases and RCTs were included.Significant heterogeneity in intervention duration, intervention times, and dosage. Most studies were from the Middle East or Southeast Asia; thus, this potentially induces bias, and the generalizability may be poor. |
| Qiu et al. [153] (2023) | 13 RCTs/n = 785 | Curcumin/various | Supplementation reduced waist circumference, FBG, TC, and BP, and inflammatory markers, including TNF- and CRP. MDA was also reduced, suggesting a decrease in oxidative stress. No significant results were seen for total triglycerides, IL-6, or hs-CRP. | Curcumin significantly reduced markers associated with T2DM and metabolic syndrome, including inflammation and oxidative stress. | Twelve of the 13 RCTs were from Asian and Middle Eastern countries; the analysis may not be generalizable to other populations.A small number of trials and patients included in the analysis was low. Many studies were of very low to moderate quality.High bias in some of the studies due to only male participants or female participants. Some RCTs used combination curcumin studies (including piperine or alkaloids) to enhance bioavailability, but other ingredients may have caused bias in the analysis. The curcumin dose was not analyzed. |
| Macena et al. [154] (2022) | 17 RCTs included/5 RCTs for turmeric/curcumin n = 745 | Turmeric/curcumin/various products/80–1,500 mg/day | Significant reductions in HbA1c, proteinuria, and MDA in T2DM patients. Also increased in the GFR.Sub-group analyses indicated a reduction in CRP concentrations in the group receiving polyphenols and soy protein. No effects on FBG. | Statistically significant but clinically modest effects of turmeric/curcumin and polyphenol consumption for reductions in HbA1c, proteinuria, GFR, CRP, and MDA. | A limited number of clinical trials were included. Difficult to interpret due to specific polyphenols having different overall effects.Significant heterogeneity in the interventions, intervention duration, intervention times, and dosage. Most studies had a high risk of bias and poor reporting of methodology. |
CRP: C-reactive protein; DBP: diastolic blood pressure; FBG: fasting blood glucose; GFR: glomerular filtration rate; HbA1c: glycated hemoglobin; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; MDA: malondialdehyde; RCTs: randomized controlled trials; T2DM: type 2 diabetes mellitus; TAC: total antioxidant capacity; TC: total cholesterol; TG: triglycerides.
Another culinary spice plant in the same plant family as turmeric is ginger, known scientifically as Zingiber officinale Roscoe, Zingiberaceae. Ginger is a tropical, herbaceous perennial plant having a pungent, aromatic rhizome that is used worldwide as a culinary food, a dried, ground spice, and a medicinal herb [155]. Known for its hot and slightly sweet flavor, ginger is an important part of Asian cuisines, curries, baked goods, teas, and other beverages. Ginger rhizomes contain several antioxidant and anti-inflammatory constituents, including the gingerols, saponins, terpenes, anthraquinones, phlobatannin, and glycosides [155–157]. These compounds and ginger extracts have been extensively investigated for their antioxidant, anti-nausea, anti-inflammatory, anti-cancer, cardiovascular, and anti-diabetic effects [156–158]. These activities of ginger are associated with its phytochemical compounds gingerol, shogaol, paradol, and zingerone that induce Nrf2 signaling, which is associated with improved cellular defense against oxidative stress. Both 6-gingerol and 6-shogaol induced the Nrf2 signaling and the expression of antioxidant genes and decreased ROS production [156]. Ginger’s anti-inflammatory activities are reportedly due to suppression of Akt and NF- signaling, as well as increased production of anti-inflammatory cytokines and decreased proinflammatory cytokines [156].
In terms of diabetes, ginger was investigated in numerous preclinical studies [159–167]. The results of these studies suggest that various ginger extracts and oils, as well as the purified gingerols and shogaols, may enhance the uptake of glucose into muscle cells, similar to the action of some diabetes medications such as metformin. Ginger extracts and oil also have other activities that may reduce the risk of diabetes-related complications [160, 161]. In pancreatic β-cells, gingerols, zingerone, and zingiberene increased insulin secretion by modulation of KATP channels [162]. In addition, these compounds inhibited α-glucosidase and α-amylase activity, two primary enzymes that control carbohydrate metabolism associated with hyperglycemia. In vivo, gingerols (specifically [S6]- and (S)-[8]-gingerol) enhanced glucose uptake into muscle cells by increasing the movement of the glucose transporter GLUT4 to the plasma membrane in Leprdb/Db T2DM mice [163]. Ginger extracts also enhanced the GLP-1-mediated glucose-induced insulin secretion in pancreatic β-cells [163]. Interestingly, one in vivo study showed that treatment of STZ-diabetic rats with ginger oil resulted in an elevated FBG after one week of treatment, but FBG concentrations were significantly reduced, and serum insulin levels increased after 8 weeks of treatment [159]. Treatment with the same ginger oil also upregulated the expression of Neurog3 and Mafb mRNA, two genes that are associated with pancreatic islet cells regeneration [159]. These results suggest that ginger oil may help restore pancreatic β-cell mass and improve insulin production [159].
Many RCTs have investigated the clinical effects of ginger products on the symptoms and outcomes of T2DM. These studies have been analyzed in numerous meta-analyses, of which six published in the past 10 years are included in Table 6.
Meta-analyses of the RCTs for ginger supplements and their effects on glycemic indices, inflammatory markers, and oxidative stress in T2DM patients.
| Reference | Number of studies/patients included | Intervention/dosage form/dose | T2DM outcomes | Conclusions | Study limitations |
|---|---|---|---|---|---|
| Garza et al. [168] (2024) | 45 RCTs (9 for ginger)/n = 3,050 | Ginger/Ginger oil /1.2–3 g/day | Ginger supplementationsignificantly reduced FBG and HbA1c, and improved insulin levels. | Supplementation with ginger significantly reduced FBG, HbA1c, and improved insulin levels in T2DM. | Significant heterogeneity between the studies in terms of products used and doses.Some studies had poor methodology, such as a lack of blinding of investigators and subjects, poor analytical methods, and a lack of control for confounding factors. Only four trials controlled for confounding, and only fourteen studies fully reported investigators’ blinding. Some studies had small sample sizes, and most studies were from the Middle East, so generalizability may be an issue. |
| Schumacher et al. [169] (2024) | 5 RCTs/n = 232 | Ginger/Fresh and dried ground to a powder/ 1.2–2 g/d | No significant effect of ginger supplementation on FBG or HbA1c. Mixed results for a reduction in fasting blood glucose in T2DM patients. | No conclusions can be made due to the limited number of trials and subjects included. | A small number of studies and subjects were included. Many studies included women only; thus, there may be a gender bias. Limitations in the ginger products included other methodical issues. |
| Ebrahimzadeh et al. [170] (2022) | 10 RCTs/not stated | Ginger/ginger oil | Ginger supplements significantly reduced FBG, HbA1c, and SBP and DBP. No significant effect on lipids. | Ginger reduced fasting blood glucose, HbA1c, and systolic and diastolic BP in patients with T2DM, but had no effect on lipid profiles. | Only studies in English were included. Most RCTs from Eastern countries, so generalizability is unknown.High heterogeneity as various doses and intervention times were used between studies. |
| Mohammad et al. [171] (2021) | 5 RCTs/n = 288 | Ginger supplements/1.6–3 g/d | Ginger supplementation significantly reduced hs-CRP, TNF-α, and IL-6 levels in patients with T2DM. | Ginger supplements reduced inflammatory parameters in patients with T2DM. | High risk of bias in some studies. A small number of studies and participants were included.Most studies from Middle Eastern countries are so generalizability is unknown. Additionally, no subgroup analyses were performed.High heterogeneity in products used, doses, and intervention times between studies. |
| Huang et al. [172] (2019) | 8 RCTs/n = 454 | Ginger supplements/ 1.6–4 g/d | No significant effect on FBG. However, a significant reduction in HbA1c. | Ginger supplementation had no significant effect on FBG but may reduce HbA1c over time in T2DM patients. | A small number of studies and participants were included.Significant heterogeneity in follow-up time period (8 to 12 weeks) and ginger products and doses. |
| Zhu et al. [173] (2018) | 10 RCTs/n = 490 | Ginger/various | Significant improvements in glycemic control and insulin sensitivity in T2DM. Reduced HbA1c and FBG. Improvements in lipid parameters were also observed. | Ginger improved glycemic control, insulin sensitivity, and lipid profiles in T2DM patients. | The study was limited in that it only included RCTs published in English or Chinese, and thus, the results may be biased. A limited number of studies and subjects may restrict the validity and generalizability. Brief treatment duration in most studies. Limited ability to detect statistically significant changes in BMI. |
CRP: C-reactive protein; DBP: diastolic blood pressure; FBG: fasting blood glucose; HbA1c: glycated hemoglobin; RCTs: randomized controlled trials; SBP: systolic blood pressure; T2DM: type 2 diabetes mellitus.
Critical analysis of data from the six meta-analyses in Table 6 suggests that ginger supplementation in doses of 1.2–4 g/day reduced markers of oxidation and inflammation in T2DM patients. However, the results for HbA1c and FBG were conflicting, with three studies showing a significant reduction in FBG and four showing reductions in HbA1c, while two studies showed no significant difference. Ginger extracts and compounds inhibited cyclooxygenase-1 (COX-1), COX-2, and 5-lipoxygenase enzymes, indicating anti-inflammatory activities. Ginger supplementation further suppressed the activation of NF-κ and significantly reduced hs-CRP, TNF-α, and IL-6 levels. Ginger further reduced the production of ROS and nitric oxide, as well as enhanced free radical scavenging. Ginger supplementation also resulted in significant reductions in blood pressure. Data from the current meta-analyses suggest that ginger did not reduce serum lipids in T2DM patients.
Since ginger is classified as “Generally Recognized as Safe” (GRAS) by the FDA, it is considered non-toxic. While some participants in clinical trials reported mild heartburn, no serious complications were observed. Most studies utilized doses between 1.6 g and 3 g per day of ginger powder in capsule form, with administration in two doses, often before or after breakfast and dinner. Several of the meta-analyses noted that many included studies were at a high risk of bias, particularly regarding selective reporting and allocation concealment. In addition, a significant portion of the RCT data originated from Iran and China, which could reduce the generalizability of these results to other populations. Other issues noted were the numerous variations in extraction methods, ginger product origin, and storage conditions, which may reduce the antioxidant and bioactive capacity of ginger.
Critical analysis of thirty-one meta-analyses and systematic reviews from (2014 to 2025) of specific FFs, including green tea, flaxseed, ACNs, and RES from fruits and vegetables, turmeric/curcumin, and ginger, suggests they may be of some benefit for the management of symptoms and chronic sequelae associated with T2DM. The primary findings suggest that while most of these FFs offer significant antioxidant benefits, their impact on glycemic regulation and systemic inflammation is highly dependent on dosage, formulation, and baseline patient health status (Table 7). Comparison analyses of the data for these FFs showed that green tea had a significant clinical impact on markers of oxidation, but limited or inconsistent effects on inflammation and long-term glycemic control. The required doses for this effect ranged from 200 mg/day of a green tea extract to 9 g/day of green tea leaves. The outcomes varied based on product type and timing; green tea extracts were more effective than infusions, and increased plasma antioxidant capacity was observed ~ one hour post-consumption.
Comparison analysis of FFs and their impact on antioxidant, anti-inflammatory, and glycemic indices in T2DM patients.
| Functional food/ingredient | Dose and dosage form | Glycemic control effects | Impacton lipids | Inflammatory markers | Oxidative stress | Cardiovascular outcomes | Study limitations and strength of evidence |
|---|---|---|---|---|---|---|---|
| Green tea | ~200 mg/day (extract) or 9 g/day (leaves). | Data were conflicting; some studies show no effect, but recent studies reported improvements in FBG, HbA1c, and insulin resistance. | Not reported. | No significant improvement in CRP, IL-6, or TNF-, slight improvement in IL-1. | Significant reduction in MDA; increased TAC, SOD, and GPX. | Not reported | Significant heterogeneity due to product, dose, treatment period, and patient population. High risk of publication bias, low to very low quality of RCTs. A small number of studies and subjects. Long-term effectiveness was reduced after 8 weeks due to variations in participant health. |
| Flaxseed | 10–100 g/day (13–40 g/day for glucose reduction); whole/ground seed superior to oil. | Significant reduction in HbA1c (especially if baseline > 7%); conflicting results for FBG and insulin unless baseline FBG is > 8 mmol/L. | Reduced lipid profiles. | No significant effect on CRP levels. | Significant reduction in MDA. | Not reported | Significant heterogeneity due to a wide range of doses and dosage forms, and patient characteristics. High risk of bias, small number of studies, and subjects. HOMA-IR results inconclusive due to small sample sizes; modest clinical weight loss. |
| Resveratrol (RES) | High dose > 1000 mg/day only | Significantly reduced FBG, HbA1c, and fasting insulin levels; improved HOMA-IR in T2DM patients. | No significant effect on TC, TG, LDL-C, or HDL-C. | Significantly reduced CRP levels and pro-inflammatory cytokines. | Reduced lipid peroxides and increased antioxidant enzyme activity (catalase and GPX). | Reduced SBP (> 7 mm Hg) and DBP (> 3 mm Hg). | Significant heterogeneity due to variations in dosage and treatment duration. High risk of bias due to small numbers of studies and subjects, and low-quality studies included in meta-analyses. |
| ACNs | Median dose of 320 mg/day for at least 8 weeks; fruit extracts and powders tested better than purified ACNs. | Reduced HbA1c (~0.31%), FBG (0.63 mmol/L), and 2h-PPG (~1.6 mmol/L). | Reduced LDL-C and TG. | Reduced markers of systemic inflammation. | Reduced markers of systemic oxidation. | Improved endothelial function, but no effective reduction in existing high blood pressure. | Significant heterogeneity in products, dose, and patient population. High risk of bias, and due to data from specific countries, may not be generalizable to all T2DM patients. A small number of studies and subjects. Low to moderate quality of included RCTs. Conflicted results for insulin resistance (HOMA-IR vs. fasting insulin). |
| Turmeric/curcumin | > 1g/day. Bioavailability-enhanced products(nanocurcumin/phytosomal) were superior. | Significantly reduced FBG and HbA1c; improved HOMA-IR. | Increased HDL; significant reductions in TG, LDL, and TC. | Reduced TNF and CRP. | Significant reduction in MDA. | Lowered DBP (~3 mmHg); inconsistent effect on SBP. | Significant heterogeneity due to products, dose, and methods. High risk of bias due to the small number of studies and subjects used in some meta-analyses. Low to moderate quality in RCTs. Magnitude of effects dependent on dose and formulation. |
| Ginger | 1.6 g to 3 g/day of powder in capsules; doses > 1 g/day. | Conflicting results in T2DM patients. Four studies show a reduction in HbA1c, three show a reduction in FBG, and two reported no difference in either. | No significant effects on TG, TC, LDL, or HDL. | Reduced hs-CRP, TNF-, and IL-6. | Inhibited ROS and NO production; enhanced free radical scavenging. | Significant reductions in SBP and DBP. | Significant heterogeneity in products and a wide range of doses used. High risk of bias due to small sample sizes, limited generalizability due to study populations, and variations in extraction/storage. |
ACNs: anthocyanins; CRP: C-reactive protein; DBP: diastolic blood pressure; FBG: fasting blood glucose; FFs: functional foods; GPX: glutathione peroxidase; HbA1c: glycated hemoglobin; HDL-C: high-density lipoprotein cholesterol; HOMA-IR: homeostasis model assessment of insulin resistance; LDL-C: low-density lipoprotein cholesterol; MDA: malondialdehyde; NO: nitric oxide; PPG: postprandial glucose; RCTs: randomized controlled trials; ROS: reactive oxygen species; SOD: superoxide dismutase; T2DM: type 2 diabetes mellitus; TAC: total antioxidant capacity; TC: total cholesterol; TG: triglycerides.
Flaxseed products also had significant antioxidant effects, but no significant effect on inflammation or CRP levels. Flaxseed was also reported to reduce HbA1c levels but showed conflicting results for FBG and insulin concentrations (Table 7). Flaxseed showed superior benefits when consumed as a whole or ground seed in doses of 14–30 g/d, rather than as a seed oil. The data for RES, ACNs, ginger, and turmeric/curcumin suggested that these FFs had the best potential for improving long-term glycemic control and showed significant improvements in both HbA1c and FBG. Meta-analyses reported that both RES and turmeric/curcumin had a significant effect on insulin signaling and IR indices (HOMA-IR), as well as blood pressure management, provided that specific dosage thresholds or high-bioavailability formulations were used. Interestingly, the dose requirement for these effects for both RES and turmeric/curcumin appeared to be > 1,000 mg/day, with doses below this level showing no effects. ACNs at a dose of 320 mg/d from fruit extracts or powders were more effective in reducing HbA1c than purified ACN supplements. While the studies for ginger remain conflicted, the largest, most recent, and comprehensive meta-analysis showed that ginger supplementation, at doses of 1.2–3 g/day, reduced HbA1c, FBG, and inflammatory markers. Interestingly, ACNs, ginger, and turmeric/curcumin were also reported to improve lipid profiles in T2DM patients (Table 7). Furthermore, turmeric/curcumin supplementation significantly reduced waist circumference, a primary indicator of dysfunctional adipose tissue and abdominal adiposity, two key drivers of T2DM morbidity and mortality.
While the outcomes of this review were positive, there are many limitations to the study. Systematic reviews and meta-analyses of RCTs are foundational to evidence-based medical practice and help to show causality. However, the quality of RCTs included in these studies is critical for the overall outcomes and strength of the evidence. The RCTs reviewed in the meta-analyses included in this work were routinely reported as having significant heterogeneity, low to moderate methodologies, and high risk of bias, including poor blinding of investigators and subjects, analytical methods, and poor control of confounding factors. This was found across all FFs analyzed. Thus, the strength of the data for these FFs is low to moderate. Other issues included a lack of a dose-response, wide variations in the FFs products/compounds and doses used, short length of the trial study period, and many studies were from foreign countries, which may reduce the overall generalizability. Also, meta-analyses from 2014–2025 were included in this review, thus containing the most current evidence; previous studies prior to 2014 may have had different outcomes. Furthermore, other confounding factors, such as alcohol consumption, diet, genetics, obesity, exercise, and smoking, were not included in all RCTs.
Overall, data from meta-analyses and systematic reviews of specific FFs with antioxidant and anti-inflammatory properties suggest that these products may improve glycemic regulation and therefore show promise as adjunct therapies for the management of T2DM. Considering that T2DM is driving the increased incidence of diabetes worldwide, research and development of these products as adjunct therapies for T2DM appears warranted. New large-scale, high-quality RCTs with robust methodologies and statistics are needed to confirm these data and the long-term benefits of FFs for T2DM.
ACNs: anthocyanins
ALA: alpha linolenic acid
C3G: cyanidin-3-glycoside
CRP: C-reactive protein
D3G: delphinidin-3-glycoside
DM: diabetes mellitus
EGCG: epigallocatechin gallate
ER: endoplasmic reticulum
FBG: fasting blood glucose
FDA: Food and Drug Administration
FFs: functional foods
GLP-1: glucagon-like peptide 1
GPX: glutathione peroxidase
HbA1c: glycated hemoglobin
HFD: high-fat diet
HOMA-IR: homeostasis model assessment of insulin resistance
IL-6: interleukin 6
MDA: malondialdehyde
RCT: randomized controlled trial
RES: resveratrol
ROS: reactive oxygen species
SOD: superoxide dismutase
STZ: streptozotocin
T2DM: type 2 diabetes mellitus
TAC: total antioxidant capacity
TC: total cholesterol
TG: triglycerides
TNF-α: tumor necrosis factor-α
UPR: unfolded protein response
WHO: World Health Organisation
The supplementary material for this article is available at: https://www.explorationpub.com/uploads/Article/file/101474_sup_1.pdf.
SMW: Investigation, Writing—original draft, Writing—review & editing. TOL: Validation, Writing—review & editing. BAA: Investigation, Validation, Writing—original draft, Writing—review & editing. GPA: Investigation, Writing—review & editing. GBM: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
All information and data in this review are in the public domain. The primary data for this systematic review were sourced online from databases listed in the methods. Referenced articles are accessible on Cochrane Library, PubMed Central/Medline, Embase, Google Scholar, and the Scopus electronic databases. Additional supporting data are available from the corresponding author upon request.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 1908
Download: 33
Times Cited: 0
