 Review
Review

Affiliation:
1Faculty of Medicine, Tbilisi State Medical University, 0186 Tbilisi, Georgia
Email: tariqnabeel88@gmail.com
ORCID: https://orcid.org/0009-0000-6763-9595
Affiliation:
1Faculty of Medicine, Tbilisi State Medical University, 0186 Tbilisi, Georgia
ORCID: https://orcid.org/0009-0007-4855-6226
Affiliation:
2Faculty of Pharmacology, K. J. Somaiya Medical College, Mumbai 400022, Maharashtra, India
ORCID: https://orcid.org/0009-0000-0539-5177
Affiliation:
3Faculty of Medicine, Jaslok Hospital and Research Center, Mumbai 400026, Maharashtra, India
ORCID: https://orcid.org/0009-0008-9464-8313
Affiliation:
4Faculty of Medicine, Dibba Hospital, Fujairah 8505, United Arab Emirates
ORCID: https://orcid.org/0009-0002-0778-2941
Affiliation:
1Faculty of Medicine, Tbilisi State Medical University, 0186 Tbilisi, Georgia
ORCID: https://orcid.org/0009-0006-5428-7643
Affiliation:
1Faculty of Medicine, Tbilisi State Medical University, 0186 Tbilisi, Georgia
ORCID: https://orcid.org/0009-0004-0659-9867
Affiliation:
5Faculty of Dentistry, Mohammed Bin Rashid University of Medicine and Health Sciences, Dubai 505055, United Arab Emirates
ORCID: https://orcid.org/0009-0006-4507-1154
Explor Cardiol. 2026;4:1012113 DOI: https://doi.org/10.37349/ec.2026.1012113
Received: March 27, 2026 Accepted: April 29, 2026 Published: July 06, 2026
Academic Editor: Cristina Sena, University of Coimbra, Portugal
Sodium–glucose cotransporter 2 inhibitors (SGLT2i) were originally developed as glucose-lowering therapies for type 2 diabetes mellitus. However, robust clinical evidence has demonstrated substantial cardiovascular and renal protective effects that extend beyond glycemic control. Emerging data highlight their systemic influence across the cardiovascular–renal–metabolic (CRM) continuum, a conceptual framework describing the shared pathophysiological links between metabolic dysfunction, heart failure (HF), and chronic kidney disease (CKD). Despite the rapid expansion of clinical and mechanistic evidence, the integration of these insights into coordinated therapeutic implementation across cardiology, nephrology, and endocrinology remains incompletely synthesized. This structured narrative review synthesized evidence from PubMed/MEDLINE, Embase, and Google Scholar to identify relevant studies published between January 2016 and December 2025. Emphasis was placed on randomized controlled trials, meta-analyses, large observational cohorts, guideline documents, and translational mechanistic investigations evaluating pharmacologic mechanisms, clinical efficacy, and multidisciplinary applications of SGLT2i across CRM conditions. Cardiovascular and renal outcome trials consistently show that SGLT2i reduce hospitalization for heart failure, delay CKD progression, and improve major cardiovascular outcomes in both diabetic and non-diabetic populations. Mechanistically, these agents restore tubuloglomerular feedback, enhance cardiac energy efficiency through increased ketone utilization, attenuate inflammatory and profibrotic signaling pathways, and improve mitochondrial bioenergetics. These multisystem effects contribute to therapeutic benefits across HF phenotypes and CKD stages while also improving metabolic parameters such as adiposity, blood pressure, and hepatic steatosis. Collectively, current evidence supports SGLT2i as foundational disease-modifying therapies across the CRM spectrum. Future investigations should prioritize precision-based treatment approaches, biomarker-guided patient selection, and rational combination pharmacotherapy to further optimize outcomes across interconnected cardiovascular, renal, and metabolic diseases.
Sodium–glucose cotransporter 2 inhibitors (SGLT2i) were originally developed as oral antihyperglycemic agents for the treatment of type 2 diabetes mellitus (T2DM) by inhibiting renal glucose reabsorption in the proximal tubule and promoting glucosuria [1]. Their insulin-independent mechanism and favorable safety profile initially positioned them as adjunctive glucose-lowering therapies in combination with other antidiabetic agents. However, findings from large cardiovascular (CV) outcome trials have fundamentally reshaped this therapeutic paradigm. Beyond glycemic control, SGLT2i have demonstrated consistent reductions in heart failure (HF) hospitalization, attenuation of chronic kidney disease (CKD) progression, and improvement in major adverse CV outcomes across diverse patient populations [1, 2]. These findings have shifted the perception of SGLT2i from conventional metabolic therapies toward multisystem disease-modifying agents with broad cardiometabolic effects.
The emerging concept of the cardiovascular–renal–metabolic (CRM) continuum reflects the complex and bidirectional interactions linking metabolic dysfunction, CV disease, and kidney injury, where conditions such as T2DM, HF, and CKD share common upstream drivers including insulin resistance, ectopic lipid accumulation, mitochondrial dysfunction, oxidative stress, chronic low-grade inflammation, and maladaptive neurohormonal activation [3, 4]. These interconnected processes promote progressive multi-organ injury through coordinated metabolic, endothelial, and hemodynamic disturbances, explaining the frequent coexistence and mutually reinforcing progression of cardiac and renal dysfunction in metabolic disease [2, 4]. The CRM framework therefore emphasizes the need for therapeutic strategies that target shared pathophysiological pathways rather than isolated disease manifestations [5, 6]. While prior reviews have mostly adopted disease-specific or organ-centered perspectives, often focusing on glycemic control or discrete cardiorenal outcomes, this review advances a unifying conceptual framework in which SGLT2 inhibition is understood as systemic metabolic stress modulation, integrating hemodynamic, energetic, inflammatory, and fibrotic pathways into a coordinated pathophysiological axis rather than parallel mechanisms [5, 7]. This approach positions metabolic stress as a central driver of CRM disease progression and extends beyond traditional models by linking mechanistic pathways with clinical phenotypes, candidate biomarkers, and therapeutic strategies, thereby providing a more integrated and translational framework for cross-disciplinary implementation of SGLT2i [1–3, 8].
The global burden of CRM disease continues to rise, driven by the close interplay between metabolic dysfunction, HF, and CKD. Approximately half of individuals with T2DM develop CKD during their lifetime, while HF and CKD frequently coexist due to shared hemodynamic, metabolic, and inflammatory mechanisms. These conditions disproportionately affect elderly individuals, populations with obesity or metabolic syndrome, and patients in low- and middle-income countries where diabetes prevalence is rapidly increasing. Improvements in survival among patients with T2DM have paradoxically prolonged exposure to CV and renal complications, amplifying the clinical and economic burden of these interconnected disorders [2, 4]. Despite this growing epidemiological convergence, much of the existing literature evaluates SGLT2i within traditional disease-specific frameworks, with reviews often focusing separately on diabetes, HF, or CKD. Such siloed approaches may overlook the broader biological mechanisms through which SGLT2 inhibition confers systemic cardiorenal protection and rarely integrate mechanistic insights with phenotype-independent therapeutic effects or multidisciplinary clinical implementation across cardiology, nephrology, and endocrinology [5–7]. In this context, the present review synthesizes mechanistic, clinical, and translational evidence to position SGLT2i as multisystem disease-modifying therapies across the CRM continuum, providing a unified framework that links metabolic, CV, and renal pathophysiology while highlighting opportunities for earlier and more coordinated clinical integration.
To support this framework, a structured narrative review was conducted using PubMed/MEDLINE, Embase, and Google Scholar to identify relevant studies published between January 2016 and November 2025. Search terms included combinations of “SGLT2 inhibitors,” “cardiorenal outcomes,” “heart failure,” “chronic kidney disease,” “metabolic syndrome,” and “cardiovascular–renal–metabolic continuum.” Priority was given to randomized controlled trials, meta-analyses, large observational studies, guideline statements, and translational mechanistic investigations. Additional references were identified through manual screening of key trial bibliographies and consensus guidelines. Adult population studies and clinically relevant therapeutic outcomes were prioritized, while preclinical data were included selectively to support mechanistic interpretation. Given the narrative design of this review, no preregistered protocol or formal risk-of-bias assessment was performed, and study selection was guided by relevance to key mechanistic and clinical themes rather than predefined inclusion criteria.
Under physiological conditions, approximately 90% of filtered glucose is reabsorbed in the proximal renal tubule via SGLT2, which couples glucose transport with sodium reabsorption to maintain metabolic homeostasis. In diabetes mellitus, chronic hyperglycemia upregulates SGLT2 expression, increasing tubular glucose and sodium reabsorption and contributing to persistent hyperglycemia and maladaptive renal hemodynamics. SGLT2i were therefore initially introduced as adjunct glucose-lowering therapies for T2DM alongside lifestyle modification and other antihyperglycemic agents. By inhibiting proximal tubular glucose reabsorption, these agents promote glucosuria and natriuresis, leading to modest reductions in glycated hemoglobin (HbA1c) levels. However, clinical trials have demonstrated that their CV and renal benefits extend beyond glycemic control and are observed even in individuals without diabetes [8].
Beyond glucose lowering, SGLT2 inhibition induces osmotic diuresis and natriuresis, resulting in modest reductions in plasma volume, blood pressure (BP), and cardiac preload. These hemodynamic effects contribute to improved ventricular loading conditions and reduced stress. Concurrent urinary caloric loss also promotes modest weight reduction and decreases ectopic fat deposition, including hepatic and myocardial fat, which may further improve cardiometabolic risk profiles, although the precise mechanisms underlying these effects remain incompletely understood [8, 9].
SGLT2i influence both cardiac metabolism and renal hemodynamics. By promoting a shift in myocardial substrate utilization toward ketone bodies, particularly β-hydroxybutyrate, these agents improve myocardial energetic efficiency and may contribute to the rapid clinical benefits observed in HF trials, supporting their use in patients with symptomatic heart failure with reduced ejection fraction (HFrEF) regardless of diabetes status [9]. At the renal level, inhibition of proximal tubular glucose and sodium reabsorption increases distal sodium delivery, restoring tubuloglomerular feedback and promoting afferent arteriolar vasoconstriction, thereby reducing intraglomerular pressure, decreasing albuminuria, and slowing CKD progression [8, 9].
In addition to these hemodynamic effects, SGLT2i exert anti-inflammatory and anti-fibrotic actions. Treatment has been associated with reductions in pro-inflammatory cytokines, chemokines, and circulating uric acid levels. Furthermore, decreased proximal tubular sodium and glucose reabsorption reduces renal oxygen demand, improving tissue oxygenation and mitochondrial metabolic efficiency in renal cells [8, 9].
SGLT2 inhibition also induces a cellular “fasting-like” metabolic state characterized by activation of adaptive pathways that promote autophagy and improve mitochondrial function. These processes enhance cellular energy homeostasis while reducing oxidative stress and inflammatory signaling. Collectively, these mechanisms suggest that the cardiorenal benefits of SGLT2i are largely glucose-independent, instead of reflecting broader metabolic and hemodynamic effects across multiple organ systems [8].
Although several individual mechanisms have been proposed, the clinical benefits of SGLT2i are unlikely to be explained by a single pathway. Instead, accumulating evidence suggests that these agents exert coordinated effects across hemodynamic, metabolic, and cellular signaling pathways that collectively restore CV and renal homeostasis. At the systemic level, osmotic diuresis and natriuresis reduce cardiac preload and interstitial congestion while improving renal oxygenation and mitigating glomerular hyperfiltration. These integrated responses form the basis for a broader mechanistic framework in which multiple molecular pathways converge to drive cardiorenal protection [8, 9].
A key renal mechanism underlying SGLT2 inhibition is the restoration of tubuloglomerular feedback through increased sodium delivery to the macula densa, which enhances adenosine-mediated afferent arteriolar vasoconstriction and reduces intraglomerular pressure. This process counteracts diabetes-associated glomerular hyperfiltration and mechanical stress, thereby decreasing albuminuria and slowing CKD progression. In parallel, interactions with the renin–angiotensin–aldosterone system (RAAS) further modulate intrarenal hemodynamics, contributing to sustained reductions in glomerular injury and improved long-term renal outcomes [8, 9].
In the myocardium, SGLT2 inhibition promotes a shift in substrate utilization toward ketone bodies, particularly β-hydroxybutyrate which serves as a more oxygen-efficient fuel compared to fatty acids. This metabolic remodeling enhances adenosine triphosphate (ATP) generation per unit oxygen consumed, improving cardiac energetic efficiency in the failing heart. Additional mechanisms may include activation of AMP-activated protein kinase (AMPK) and inhibition of mammalian target of rapamycin (mTOR) signaling, which together promote cellular energy conservation and adaptive metabolic reprogramming. These changes contribute to improved myocardial function and may partly explain the early clinical benefits observed in HF trials [9].
Beyond hemodynamic and metabolic effects, SGLT2i exert important anti-inflammatory and anti-fibrotic actions at the molecular level. These include suppression of nuclear factor kappa B (NF-κB) signaling, inhibition of the NLR family pyrin domain containing 3 (NLRP3) inflammasome, and downregulation of transforming growth factor-β (TGF-β)/SMAD pathways, all of which are central mediators of chronic inflammation and tissue fibrosis. Through these mechanisms, SGLT2 inhibition attenuates cardiac remodeling and reduces renal interstitial fibrosis, thereby limiting structural disease progression across both organ systems [8, 9].
SGLT2 inhibition also modulates oxidative stress and mitochondrial function which are key contributors to cellular injury in CRM disease. Treatment has been associated with reduced production of reactive oxygen species (ROS), improved mitochondrial biogenesis, and enhanced autophagic flux mediated through pathways such as sirtuin 1 (SIRT1) and AMPK activation. These effects improve cellular energy homeostasis and reduce oxidative damage in both cardiac and renal tissues, while decreased tubular workload further enhances renal oxygenation and mitochondrial efficiency [8, 9].
Collectively, these mechanisms support a model in which SGLT2i act as systemic modulators of the CRM axis rather than targeting isolated pathways. By simultaneously influencing hemodynamic regulation, metabolic efficiency, inflammatory signaling, and cellular stress responses, these agents restore cross-talk between the heart, kidney, and metabolic systems. This integrated, systems-level modulation provides a unifying biological explanation for the consistent therapeutic benefits of SGLT2i across HF, CKD, and metabolic disorders, reinforcing their role as disease-modifying therapies within the CRM continuum [8, 9]. These mechanisms can be conceptually grouped into interacting “stress domains”, including hemodynamic, energetic/mitochondrial, inflammatory/fibrotic, and glucotoxic/lipotoxic pathways, which together provide a unifying framework for interpreting clinical outcomes across the CRM spectrum. These mechanisms are interrelated and operate across different temporal and organ-specific levels. Hemodynamic effects, including natriuresis and restoration of tubuloglomerular feedback, occur early and are primarily renal, whereas metabolic adaptations such as enhanced ketone utilization and mitochondrial efficiency develop later and are particularly relevant to cardiac function. Anti-inflammatory and anti-fibrotic pathways likely represent downstream effects contributing to structural remodeling. While some mechanisms are organ-specific, others including oxidative stress reduction and mitochondrial optimization are shared across the CRM axis, supporting a unified systems-level model of action. Summary of all the mechanisms and pathways has been illustrated in Figure 1.
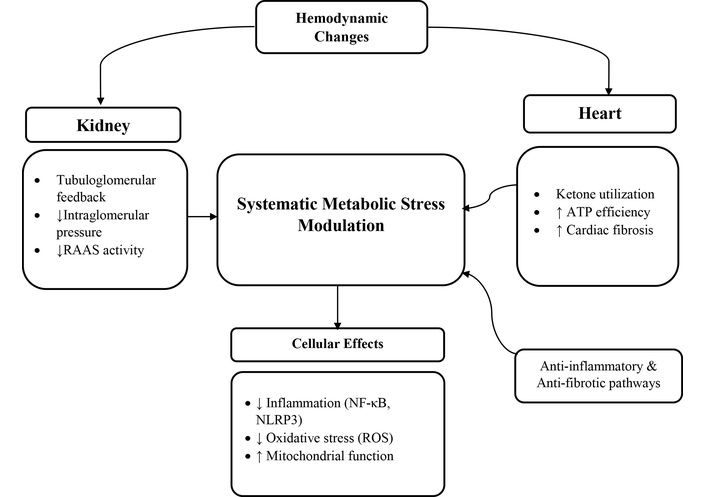
Mechanistic pathways of SGLT2i across the CRM axis. RAAS: renin–angiotensin–aldosterone system; ATP: adenosine triphosphate; NF-κB: nuclear factor kappa B; NLRP3: NLR family pyrin domain containing 3; ROS: reactive oxygen species; ↓: decreased; ↑: increased.
Large randomized outcome trials have fundamentally reshaped the therapeutic landscape of HF by demonstrating consistent benefits of SGLT2i across the left ventricular ejection fraction spectrum. Early landmark trials established their role in HFrEF. In the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF) and Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Reduced Ejection Fraction (EMPEROR-Reduced) trials, dapagliflozin and empagliflozin significantly reduced the composite outcome of CV death or worsening HF regardless of diabetes status, with relative risk reductions of approximately 25–26% [10–12]. Although both trials demonstrated comparable overall benefit, differences in baseline patient characteristics including renal function and natriuretic peptide levels likely contributed to variations in outcome distribution, with EMPEROR-Reduced showing a stronger reduction in HF hospitalization and DAPA-HF demonstrating a more balanced reduction in both hospitalization and mortality outcomes [11, 12].
Subsequent trials expanded the therapeutic scope of SGLT2i to patients with preserved or mildly reduced EF, populations historically lacking effective disease-modifying therapies. The EMPEROR-Preserved and Dapagliflozin Evaluation to Improve the LIVEs of Patients With PReserved Ejection Fraction Heart Failure (DELIVER) trials demonstrated significant reductions in the composite endpoint of CV death or HF hospitalization among patients with HF with mildly reduced ejection fraction (HFmrEF) and HF with preserved ejection fraction (HFpEF) [13–15]. In these populations, the observed benefits were primarily driven by reductions in HF hospitalization rather than mortality, reflecting persistent pathophysiological differences between preserved and reduced EF phenotypes. This difference likely reflects underlying pathophysiological heterogeneity between HFrEF and HFpEF. In HFrEF, where neurohormonal activation and ventricular remodeling are dominant drivers, SGLT2i may exert broader effects on myocardial energetics, remodeling, and survival pathways, contributing to both reduced hospitalization and mortality [14]. In contrast, HFpEF is characterized by greater phenotypic diversity, including contributions from systemic inflammation, obesity, microvascular dysfunction, and atrial myopathy, which may attenuate mortality benefits and result in more consistent effects on congestion-related outcomes such as hospitalization [14, 15].
Pooled analyses across these trials confirm a consistent class effect of SGLT2 inhibition throughout the EF spectrum, with significant reductions in CV death or HF hospitalization irrespective of baseline diabetes status [16]. Importantly, improvements in patient-reported outcomes including Kansas City Cardiomyopathy Questionnaire (KCCQ) scores have also been consistently observed, indicating meaningful improvements in symptoms and functional status beyond traditional clinical endpoints [14].
Collectively, these findings establish SGLT2i as foundational therapy in chronic HFrEF and, in line with current HF guidelines, increasingly across HFmrEF and HFpEF, despite differences in trial populations, baseline risk, and event rates, as well as underrepresentation of specific phenotypes such as severe obesity, advanced atrial myopathy, and pulmonary hypertension, warrant cautious interpretation in certain subgroups [16, 17]. Their benefits across diverse HF phenotypes including reductions in hospitalization risk, improvements in quality of life, and favorable CV outcomes support their integration into contemporary guideline-directed medical therapy [17]. A comparative summary of major randomized trials evaluating SGLT2i across the HF spectrum is presented in Table 1.
Summary of major randomized controlled trials evaluating cardiovascular outcomes of SGLT2 inhibitors across HF phenotypes.
| Trial | Drug | Population | EF range | Sample size | Primary outcome | Key results | Mortality benefit |
|---|---|---|---|---|---|---|---|
| DAPA-HF | Dapagliflozin | Symptomatic HFrEF with or without T2DM | ≤ 40% | 4,744 | Composite of CV death or worsening HF | 26% relative risk reduction in primary outcome | Reduced CV death and HF hospitalization |
| EMPEROR-Reduced | Empagliflozin | Chronic HFrEF | ≤ 40% | 3,730 | CV death or HF hospitalization | 25% reduction in primary composite endpoint | Trend toward reduced CV mortality |
| EMPEROR-Preserved | Empagliflozin | HFpEF | > 40% | 5,988 | CV death or HF hospitalization | 21% reduction driven mainly by reduced HF hospitalization | No significant mortality reduction |
| DELIVER | Dapagliflozin | HFmrEF and HFpEF | > 40% | 6,263 | CV death or worsening HF | 18% reduction in primary composite outcome | Modest mortality effect |
| EMPULSE | Empagliflozin | Acute decompensated HF (hospitalized patients) | All EF ranges | 530 | Composite clinical benefit at 90 days | Improved clinical status and reduced rehospitalization | Not powered for mortality |
Differences in inclusion criteria (e.g., EF thresholds, natriuretic peptide levels, renal function) and baseline characteristics across trials should be considered when comparing outcomes across HF phenotypes. CV: cardiovascular; T2DM: type 2 diabetes mellitus; HFrEF: heart failure with reduced ejection fraction; HFpEF: heart failure with preserved ejection fraction; HFmrEF: heart failure with mildly reduced ejection fraction.
The strong evidence for SGLT2i in HF goes beyond glycemic status, showing consistent benefit in both diabetic and non-diabetic individuals. Meta-analyses of large randomized studies demonstrate that SGLT2i lower the composite of hospitalization for heart failure (HHF) or CV deaths in HF, regardless of diabetes, with hazard ratios that are strikingly similar across subgroups. A comprehensive analysis found about 24% reduction in combined HF hospitalization or CV death in HF, about 23% in T2DM cohorts, and consistent benefit regardless of concurrent CKD status, indicating glycemia-independent mechanisms driving these outcomes [18]. Importantly, subgroup results from DAPA-HF and EMPEROR-Reduced show that reductions in key endpoints continue in non-diabetic HFrEF patients with effect sizes equivalent to the whole trial populations, highlighting the class effect beyond glucose lowering [19].
In terms of phenotype, SGLT2i assist people with HF across the board. While early research focused on chronic HFrEF, more recent studies involving HFpEF and HFmrEF populations show consistent decreases in HF episodes regardless of EF. In pooled analyses, SGLT2 inhibition reduced CV death/HHF outcomes in HFpEF and HFmrEF with hazard ratios about 0.80, even in non-diabetic categories, indicating phenotype-agnostic efficacy [20].
The contrast between acute and chronic HF scenarios emphasizes the range of SGLT2i use. Evidence from acute heart failure (HF) cohorts suggests that starting therapy early improves patient outcomes. This benefit applies to initiation during or immediately after a hospital stay for decompensated HF, supporting rapid rather than delayed therapy. These findings are supported by trials like Empagliflozin in Patients Hospitalized With Acute Heart Failure Who Have Been Stabilized (EMPULSE), which evaluated the selective SGLT2 inhibitor empagliflozin, as well as separate studies on the dual SGLT1/2 inhibitor sotagliflozin [21]. These early advantages which appear within weeks suggest against waiting for chronic stabilization before initiating medication and highlight the need of early SGLT2i inclusion into guideline-directed management.
Collectively, this evidence has shifted guideline positioning. SGLT2i now play a foundational role in all HF phenotypes and diabetes statuses with recommendations for early initiation in both chronic and acute settings to maximize reductions in HF hospitalization and CV mortality [21]. Although benefits are consistent across EF ranges, variabilities in patient selection and underlying pathophysiology suggest that therapeutic responses may differ across specific HF phenotypes, highlighting the need for further phenotype-specific investigation.
Evidence from large randomized trials has established SGLT2i as important therapies for slowing CKD progression and reducing CV risk. Early signals of renoprotection were observed in the Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients-Removing Excess Glucose (EMPA-REG OUTCOME) trial, where empagliflozin significantly reduced the risk of incident or worsening nephropathy and slowed decline in renal function among patients with T2DM and established CV disease [22, 23].
Subsequent dedicated renal outcome trials confirmed these findings. The Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) trial demonstrated that canagliflozin significantly reduced the composite outcome of end-stage kidney disease (ESKD), doubling of serum creatinine, or renal death in patients with T2DM and albuminuric CKD, while also lowering the risk of CV events and HF hospitalization [24]. Similarly, the DAPA-CKD trial showed that dapagliflozin significantly reduced the risk of sustained estimated glomerular filtration rate (eGFR) decline, ESKD, or renal and CV death in patients with CKD with or without diabetes, leading to early termination of the trial due to clear efficacy [25].
More recently, the Study of Heart and Kidney Protection With Empagliflozin (EMPA-KIDNEY) trial expanded these observations to a broader CKD population, including individuals without diabetes and those with lower baseline eGFR. Empagliflozin significantly reduced the risk of kidney disease progression or CV death and was associated with lower rates of hospitalization, further supporting the role of SGLT2 inhibition across diverse CKD phenotypes [26].
From a clinical perspective, these findings support early initiation of SGLT2i in patients with CKD, particularly those with albuminuria or declining renal function. Current evidence indicates that benefits extend to patients with eGFR as low as 20 mL/min/1.73 m², even when glycemic effects are attenuated. A transient decline in eGFR following treatment initiation is expected and reflects restoration of tubuloglomerular feedback rather than nephrotoxicity. When combined with RAAS blockade, SGLT2i provide complementary mechanisms that reduce intraglomerular pressure, decrease proteinuria, and slow CKD progression [23, 25, 26]. The strength of evidence is most robust in patients with diabetic and albuminuric CKD, where large randomized trials have consistently demonstrated reductions in renal and CV outcomes. Major randomized trials evaluating renal and CV outcomes of SGLT2i in CKD are summarized in Table 2.
Comparison of major randomized trials evaluating renal outcomes and cardiovascular protection with SGLT2 inhibitors.
| Trial | Drug | CKD population | Diabetes status | eGFR inclusion | Albuminuria criteria | Primary renal endpoint | Key renal outcomes | Cardiovascular outcomes |
|---|---|---|---|---|---|---|---|---|
| CREDENCE | Canagliflozin | Albuminuric CKD | T2DM only | 30–90 mL/min/1.73 m² | UACR > 300 mg/g | ESRD, doubling creatinine, or renal death | 34% reduction in renal composite outcome | Reduced HF hospitalization and MACE |
| DAPA-CKD | Dapagliflozin | CKD with and without diabetes | Mixed population | 25–75 mL/min/1.73 m² | UACR 200–5,000 mg/g | ≥ 50% eGFR decline, ESRD, renal or CV death | 39% relative risk reduction | Reduced CV mortality and HF hospitalization |
| EMPA-KIDNEY | Empagliflozin | Broad CKD population | Mixed population | ≥ 20 mL/min/1.73 m² | Included low and moderate albuminuria | Kidney disease progression or CV death | 28% reduction in disease progression | Reduced hospitalization risk |
| EMPA-REG renal subgroup | Empagliflozin | T2DM with CV disease | T2DM | ≥ 30 mL/min/1.73 m² | Not primary inclusion | Incident or worsening nephropathy | Reduced progression of kidney disease | Reduced CV mortality |
CKD: chronic kidney disease; CV: cardiovascular; T2DM: type 2 diabetes mellitus; eGFR: estimated glomerular filtration rate; UACR: urinary albumin-to-creatinine ratio; ESRD: end-stage renal disease; HF: heart failure; MACE: major adverse cardiovascular events.
While SGLT2i have demonstrated clear renal protective effects in patients with diabetic and albuminuric CKD, evidence in non-diabetic and particularly nonproteinuric CKD remains more limited and continues to evolve. These effects have been verified through major trials such as DAPA-CKD, CREDENCE, and EMPA-KIDNEY. Kidney function deterioration is further reduced by regulating signaling pathways [27].
Moreover, SGLT2i use was associated with improvement in estimated GFR decline in non-diabetic CKD. In patients with both urine protein-to-creatinine ratio (UPCR) < 0.15 g/gCre and 0.15–0.5 g/gCre, there was significant reduction in eGFR decline. Favorable effects have been seen for patients having proteinuria, but are still unclear for patients without proteinuria. Mechanism of SGLT2i showing kidney-protective effects in nonproteinuric CKD is still unknown [28]. CREDENCE trial, which had significant impact on use of SGLT2i in patients with kidney disease, was not able to provide with the details emphasizing whether the nephroprotective effects of SGLT2i could also be seen in CKD patients without diabetes [29]. DAPA-CKD trial showed SGLT2i have kidney protective effects in patients with CKD without T2DM [25].
In a randomized controlled trial conducted to determine the role of dapagliflozin on progression of proteinuria among non-diabetic adult patients with CKD, patients on dapagliflozin showed reduction in albumin-to-creatinine ratio (ACR) along with increase in eGFR as compared to placebo group which showed constant decline in eGFR and no change in ACR [30]. Canagliflozin reduced the doubling of creatinine, ESKD, and death from renal or CV causes by 30%. Patients on dapagliflozin showed reduced risk of ESKD by 36% and reduction in 50% eGFR decline by 47% [31]. Among patients who received SGLT2i, occurrence of renal death or the need for renal transplant or dialysis was 35% to 50% which is lower than that among patients who received placebo [32].
Although SGLT2i were initially developed to improve glycemic control by increasing urinary glucose excretion, accumulating evidence indicates that their metabolic effects extend well beyond glucose lowering. These agents influence multiple cardiometabolic pathways, including adipose tissue distribution, vascular function, uric acid metabolism, and hepatic lipid handling, thereby contributing to broader CRM protection [33].
One of the most consistently observed extra-glycemic effects is modest weight reduction accompanied by improvements in body composition. Meta-analyses of randomized controlled trials demonstrate that SGLT2i therapy is associated with reductions in visceral adipose tissue (VAT), subcutaneous fat, body weight, waist circumference, and body mass index. These changes likely result from chronic urinary caloric loss and may contribute to improved insulin sensitivity and reduction of cardiometabolic risk [34].
SGLT2i also exert favorable hemodynamic and metabolic effects, including modest but consistent reductions in BP independent of glycemic control. These effects are primarily mediated through natriuresis, osmotic diuresis, and improved sodium handling, which collectively reduce vascular stiffness and hemodynamic load on the CV system [35]. In addition, SGLT2 inhibition promotes increased renal urate excretion, leading to reductions in circulating uric acid levels that may further contribute to CV and renal risk reduction [36].
Emerging evidence suggests that SGLT2i may reduce liver fat content and improve liver enzyme levels in patients with metabolic dysfunction-associated steatotic liver disease (MASLD). However, much of this evidence is derived from relatively small studies using surrogate endpoints such as imaging and biochemical markers. As such, these findings should be considered preliminary, and large-scale trials incorporating histological endpoints and long-term clinical outcomes are needed to establish their role in hepatic disease [37].
Collectively, these extra-glycemic metabolic effects including improvements in adiposity, BP, uric acid metabolism, and hepatic steatosis target key drivers of cardiometabolic disease and provide a mechanistic basis for the consistent systemic benefits observed in large CV and renal outcome trials. The major metabolic effects of SGLT2i beyond glycemic control are summarized in Table 3.
Summary of extra-glycemic systemic effects contributing to cardiometabolic benefits of SGLT2 inhibitors.
| Physiological domain | Mechanism | Magnitude of effect | Clinical implication |
|---|---|---|---|
| Weight reduction | Caloric loss via glucosuria | 2–3 kg average weight reduction | Improved cardiometabolic risk profile |
| Visceral adiposity | Reduction in ectopic fat deposition | Reduced visceral and hepatic fat | Lower metabolic syndrome burden |
| Blood pressure | Natriuresis and plasma volume reduction | About 3–5 mmHg systolic BP reduction | Adjunct antihypertensive effect |
| Uric acid reduction | Increased renal urate excretion | Significant uric acid lowering | Potential reduction in CV and renal risk |
| Liver metabolism | Improved hepatic steatosis and inflammation | Reduced liver fat content and ALT/AST levels | Emerging therapy for MASLD |
| Mitochondrial efficiency | Ketone body utilization and metabolic shift | Improved myocardial energetics | Potential antiarrhythmic and HF benefit |
| Insulin sensitivity | Reduced glucotoxicity and lipotoxicity | Improved metabolic homeostasis | Delay progression of T2DM |
BP: blood pressure; ALT: alanine aminotransferase; AST: aspartate aminotransferase; CV: cardiovascular; MASLD: metabolic dysfunction-associated steatotic liver disease; HF: heart failure; T2DM: type 2 diabetes mellitus.
Large CV and renal outcome trials consistently demonstrate that SGLT2i have a generally favorable safety profile, with most adverse effects reflecting predictable pharmacologic mechanisms rather than drug-specific toxicity. The most commonly reported events are genital mycotic infections, which occur more frequently in women and are typically mild and responsive to standard antifungal therapy, rarely requiring treatment discontinuation [22].
Volume depletion–related symptoms, including dizziness or orthostatic hypotension, may occur due to osmotic diuresis and natriuresis. These events are more likely in elderly individuals and patients receiving concomitant diuretics, emphasizing the importance of assessing baseline volume status and adjusting diuretic therapy when initiating treatment [38].
Euglycemic diabetic ketoacidosis (EDKA) represents a rare but important complication of SGLT2i therapy. It is most commonly observed in conditions associated with relative insulin deficiency, such as acute illness, prolonged fasting, or perioperative stress. Because blood glucose levels may remain near normal, clinical recognition requires awareness of this atypical presentation and appropriate patient education regarding temporary drug discontinuation during high-risk situations [39].
From a practical perspective, implementation of “sick-day rules” is essential to minimize the risk of EDKA. Temporary discontinuation of SGLT2i is recommended during acute illness, major surgery, prolonged fasting, or conditions associated with reduced oral intake or relative insulin deficiency. Perioperative management should include withholding the drug at least 3–4 days prior to major procedures and resuming only once the patient is clinically stable and able to maintain adequate oral intake [39, 40].
Early concerns regarding an increased risk of lower limb amputation were primarily observed in the cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS) program involving canagliflozin. However, subsequent trials and meta-analyses have not demonstrated a consistent class-wide association. Current evidence suggests that this signal may be drug-specific or related to underlying peripheral vascular disease, although careful monitoring remains advisable in high-risk patients [40].
Initiation of SGLT2i is commonly associated with a modest and transient decline in eGFR, reflecting restoration of tubuloglomerular feedback rather than nephrotoxicity. This initial change is typically followed by long-term preservation of renal function, particularly when therapy is combined with RAAS [25]. Overall, the favorable benefit–risk profile of SGLT2i supports their use across CV and renal disease populations when appropriate patient selection and monitoring strategies are applied.
Common adverse effects, associated risk factors, and recommended monitoring strategies for SGLT2i therapy are summarized in Table 4.
Safety considerations and recommended monitoring strategies for SGLT2 inhibitor therapy.
| Adverse effect | Incidence | High-risk populations | Mechanism | Prevention strategies | Monitoring recommendations |
|---|---|---|---|---|---|
| Genital mycotic infections | Common | Females, prior infections | Glycosuria promoting fungal growth | Hygiene education, early antifungal therapy | Monitor for symptoms after initiation |
| Volume depletion | Moderate | Elderly, diuretic users | Osmotic diuresis | Dose adjustment of diuretics | Monitor BP and hydration status |
| EDKA | Rare | Insulin-deficient states, acute illness | Increased ketogenesis | Withhold drug during illness or surgery | Monitor ketone levels in symptomatic patients |
| Lower limb amputation | Controversial, rare | Peripheral vascular disease | Possibly volume and vascular effects | Careful foot monitoring | Regular foot examination |
| Acute kidney injury | Rare | Dehydrated or volume-depleted patients | Transient renal hemodynamic changes | Ensure adequate hydration | Monitor renal function after initiation |
| Hypotension | Occasional | Frail elderly | Volume contraction | Gradual drug initiation | BP monitoring during early therapy |
BP: blood pressure; EDKA: euglycemic diabetic ketoacidosis.
SGLT2i have rapidly transitioned from glucose-lowering agents to foundational therapies across HF and CKD management. Contemporary CV and nephrology guidelines recommend SGLT2i such as dapagliflozin and empagliflozin for reducing HF hospitalization, CV mortality, and CKD progression, irrespective of diabetes status or ejection fraction phenotype. These recommendations reflect consistent findings from major outcome trials demonstrating cardiorenal protection across diverse patient populations [21].
Given the multisystem benefits of SGLT2i, effective implementation increasingly requires coordinated care between cardiology, nephrology, and endocrinology. Multidisciplinary care pathways involving physicians, pharmacists, nurses, and allied health professionals can facilitate earlier therapy initiation, improve patient education, and enhance adherence to guideline-directed medical therapy. Pharmacists in particular play an important role in medication optimization, monitoring for adverse effects, and supporting safe titration of cardiometabolic therapies [41].
Emerging evidence suggests that early initiation of SGLT2i, including during or shortly after hospitalization for acute HF, is associated with rapid clinical benefits such as improved functional status and reduced rehospitalization. As a result, contemporary management strategies increasingly support early integration of SGLT2i alongside other guideline-directed therapies, including RAAS inhibitors and other cardiometabolic agents, to maximize cardiorenal protection [42].
Despite strong guideline recommendations, real-world uptake of SGLT2i remains suboptimal. Barriers include clinician hesitation related to perceived safety concerns, limited awareness of expanding indications, fragmented specialty care, and uncertainty regarding prescribing responsibility. Addressing these challenges will require targeted educational initiatives, improved interdisciplinary collaboration, and structured clinical pathways to facilitate earlier and broader adoption of SGLT2i therapy across the CRM continuum [43].
A proposed clinical algorithm for SGLT2i initiation across CRM conditions is illustrated in Figure 2.
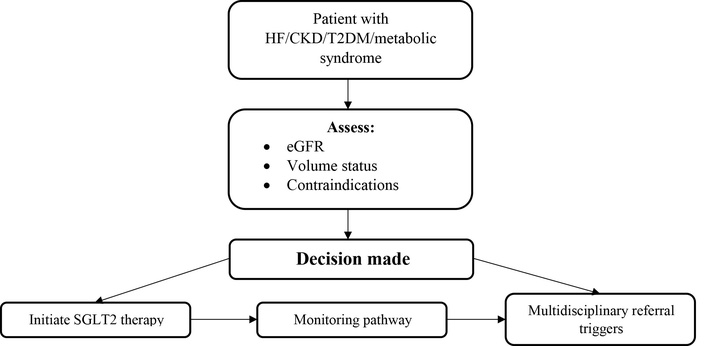
Clinical algorithm for SGLT2 inhibitor initiation across cardiovascular, renal, and metabolic diseases. HF: heart failure; CKD: chronic kidney disease; T2DM: type 2 diabetes mellitus; eGFR: estimated glomerular filtration rate; SGLT2: sodium–glucose cotransporter 2.
Despite substantial evidence supporting the CV and renal benefits of SGLT2i, several clinically important populations remain underrepresented in randomized trials. Patients with advanced CKD, particularly those with eGFR < 15 mL/min/1.73 m² or requiring dialysis, are frequently excluded, resulting in limited evidence regarding efficacy and safety in this high-risk group [7]. Similarly, frail older adults, who often have multimorbidity, polypharmacy, and increased susceptibility to volume depletion, hypotension, and adverse drug interactions, are insufficiently represented in clinical trials, raising concerns regarding tolerability and real-world applicability. In addition, ethnic minorities and populations in low- and middle-income countries remain underrepresented despite bearing a disproportionate burden of cardiometabolic disease, with disparities in access, cost, and healthcare infrastructure further limiting implementation. Addressing these gaps will require targeted, inclusive clinical trials and real-world studies designed to capture diverse and high-risk patient populations [18].
Another important area of uncertainty involves the long-term durability and safety of SGLT2i therapy. Although major outcome trials demonstrate consistent cardiorenal benefits, follow-up durations are relatively limited. Long-term observational studies and pharmacovigilance data will therefore be essential to clarify the persistence of therapeutic benefit and detect rare adverse events that may emerge with prolonged exposure [44].
An important emerging area of investigation is the role of biomarker-guided precision therapy in optimizing SGLT2i use. Several candidate biomarkers have been proposed to predict treatment response across the CRM spectrum, including natriuretic peptides such as N-terminal pro-brain natriuretic peptide (NT-proBNP) for HF outcomes, urinary albumin-to-creatinine ratio (UACR) and eGFR slope for renal response, and circulating ketone levels reflecting metabolic adaptation [45, 46]. In addition, mechanistic biomarkers related to inflammation and fibrosis, including C-reactive protein (CRP), interleukin-6 (IL-6), galectin-3, and soluble suppression of tumorigenicity 2 protein (ST2), may provide insight into individual variability in therapeutic response. However, most of these biomarkers remain exploratory and are derived largely from post hoc analyses, with limited prospective validation in biomarker-enriched clinical trials. Future research should focus on integrating biomarker profiling with phenotypic stratification to enable more precise, individualized treatment strategies and improve risk–benefit assessment across diverse patient populations [47].
Expanding therapeutic applications of SGLT2i also represents an important research priority. Emerging data suggest potential benefits in additional clinical contexts, including cardio-oncology populations exposed to cardiotoxic therapies and patients with HF characterized by obesity-related metabolic dysfunction. However, robust randomized evidence in these settings remains limited, highlighting the need for targeted trials evaluating the role of SGLT2 inhibition in diverse cardiometabolic phenotypes.
Combination cardiometabolic therapy represents another promising direction. Observational studies and meta-analyses suggest that combining SGLT2i with glucagon-like peptide-1 receptor agonists (GLP-1 RA) may provide complementary metabolic and CV benefits. Nevertheless, these findings remain largely hypothesis-generating due to the absence of large outcome-driven trials specifically designed to evaluate combination strategies [45, 46].
Several key research questions remain unanswered and should guide future investigation. These include identifying which patient subgroups derive the greatest benefit from SGLT2 inhibition, particularly among non-diabetic HF and non-proteinuric CKD populations; determining whether specific biomarkers or phenotypic profiles can reliably predict therapeutic response; defining optimal sequencing and combination strategies with other cardiometabolic agents such as GLP-1 RA; and establishing the long-term safety and durability of treatment effects beyond current trial follow-up periods. Addressing these questions through adequately powered, phenotype-driven, and biomarker-enriched studies will be essential to fully realize the potential of SGLT2i within a precision medicine framework.
SGLT2i have emerged as transformative therapies across the CRM continuum. Beyond their glucose-lowering effects, these agents consistently reduce HF hospitalization, slow CKD progression, and improve CV outcomes across diverse populations, including individuals without diabetes. These benefits are largely mediated through integrated hemodynamic, metabolic, and anti-inflammatory mechanisms that target shared pathophysiological pathways linking heart, kidney, and metabolic disease.
The incorporation of SGLT2i into contemporary cardiology and nephrology guidelines reflects their role as foundational disease-modifying therapies rather than adjunct metabolic agents. Future research should focus on expanding evidence in underrepresented populations, evaluating long-term safety, and developing precision-based strategies to optimize patient selection and therapeutic combinations. Continued advances in these areas will further define the role of SGLT2 inhibition as a cornerstone of integrated cardiometabolic care.
ACR: albumin-to-creatinine ratio
AMPK: AMP-activated protein kinase
ATP: adenosine triphosphate
BP: blood pressure
CKD: chronic kidney disease
CREDENCE: Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
CRM: cardiovascular–renal–metabolic
CV: cardiovascular
DAPA-HF: Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure
EDKA: euglycemic diabetic ketoacidosis
EF: ejection fraction
eGFR: estimated glomerular filtration rate
EMPA-REG OUTCOME: Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients-Removing Excess Glucose
EMPEROR-Reduced: Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Reduced Ejection Fraction
ESKD: end-stage kidney disease
GLP-1 RA: glucagon-like peptide-1 receptor agonist
HF: heart failure
HFmrEF: heart failure with mildly reduced ejection fraction
HFpEF: heart failure with preserved ejection fraction
HFrEF: heart failure with reduced ejection fraction
HHF: hospitalization for heart failure
MASLD: metabolic dysfunction-associated steatotic liver disease
RAAS: renin–angiotensin–aldosterone system
SGLT2: sodium–glucose cotransporter-2
SGLT2i: sodium–glucose cotransporter-2 inhibitors
T2DM: type 2 diabetes mellitus
UACR: urinary albumin-to-creatinine ratio
NT: Conceptualization, Writing—original draft, Writing—review & editing. AWI: Conceptualization, Writing—original draft, Writing—review & editing, Supervision. PD, TP, MRM, MA, SRM, and BT: Writing—original draft, Writing—review & editing. All authors read and approved the final version of this manuscript.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 329
Download: 18
Times Cited: 0
