Original Article
Original Article

Affiliation:
1Dermatology Department, General Hospital 8th September, 1000 Skopje, North Macedonia
2Higher Medical School, University St. Kliment Ohridski, 7000 Bitola, North Macedonia
Email: vesna.dojcinovska@gmail.com
ORCID: https://orcid.org/0009-0000-4043-2236
Affiliation:
3Dermatology Department, Remedica Hospital, 1000 Skopje, North Macedonia
4Faculty of Dental Medicine, International Balkan University, 1000 Skopje, North Macedonia
Affiliation:
5Department of Dermatology, Faculty of Medicine, Bahcesehir University, 34353 Istanbul, Türkiye
6Institute of Allergology, Charité-Universitätsmedizin, 12203 Berlin, Germany
ORCID: https://orcid.org/0000-0003-2801-0959
Affiliation:
7Moscow Research and Clinical Center of Allergy and Immunology, City Clinical Hospital 52, Moscow 123182, Russian Federation
8Department of Clinical Immunology and Allergology, I.M. Sechenov First Moscow State Medical University, Moscow 119991, Russian Federation
9Department of Pulmonology, Astana Medical University, Astana 010000, Kazakhstan
ORCID: https://orcid.org/0000-0002-5083-6637
Affiliation:
10University Clinic of Dermatology, SS Cyril and Methodius University, 1000 Skopje, North Macedonia
ORCID: https://orcid.org/0009-0005-2072-2160
Affiliation:
11Department of Pulmonology and Allergology, General Hospital 8th September, 1000 Skopje, North Macedonia
12Faculty of Medical Sciences, Goce Delcev University, 2000 Stip, North Macedonia
ORCID: https://orcid.org/0000-0002-9292-5232
Affiliation:
1Dermatology Department, General Hospital 8th September, 1000 Skopje, North Macedonia
ORCID: https://orcid.org/0009-0002-2823-2068
Affiliation:
1Dermatology Department, General Hospital 8th September, 1000 Skopje, North Macedonia
ORCID: https://orcid.org/0009-0005-5461-0773
Affiliation:
1Dermatology Department, General Hospital 8th September, 1000 Skopje, North Macedonia
ORCID: https://orcid.org/0009-0007-2193-8742
Affiliation:
1Dermatology Department, General Hospital 8th September, 1000 Skopje, North Macedonia
ORCID: https://orcid.org/0009-0008-5323-6275
Affiliation:
1Dermatology Department, General Hospital 8th September, 1000 Skopje, North Macedonia
ORCID: https://orcid.org/0009-0001-6336-777X
Explor Asthma Allergy. 2025;3:1009101 DOI: https://doi.org/10.37349/eaa.2025.1009101
Received: September 10, 2025 Accepted: November 13, 2025 Published: December 01, 2025
Academic Editor: Lawrence DuBuske, George Washington University Hospital, United States
The article belongs to the special issue Bridging Experimental and Translational Allergology
Aim: Angioedema is a common but often underestimated manifestation of chronic spontaneous urticaria (CSU). Its presence may indicate higher disease severity, longer duration, and autoimmune involvement. This study aims to assess the clinical relevance and associations of angioedema in CSU patients with disease severity and duration, treatment response to H1-antihistamines, correlation with autoimmune status, and autologous serum skin test (ASST) positivity.
Methods: A prospective study was conducted at the Dermatology Department, General Hospital 8th September, Skopje, North Macedonia, from December 2021 to November 2022, including 230 CSU patients. Disease activity was assessed using the Urticaria Activity Score over 7 days (UAS7), and severity was categorized accordingly. Response to H1-antihistamines was defined as achieving UAS7 < 7 for several months. Angioedema was recorded as a symptom regardless of localization. Autoimmune status was based on autoimmune disease history and/or autoantibody (AAb) detection. The ASST was performed, classifying patients as ASST-positive (ASST⁺) or ASST-negative (ASST⁻).
Results: Angioedema was observed in 70% of CSU patients, all with accompanying wheals. It was significantly more common in severe CSU than in moderate (82.02% vs. 65.38%, p = 0.026), mild (82.02% vs. 65.96%, p = 0.036), and well-controlled disease (82.02% vs. 45.45%, p = 0.0004). Patients with a positive autoimmune status more often had angioedema than those with a negative status (75.17% vs. 61.18%, p = 0.025). CSU showed longer duration in patients with angioedema (p = 0.000012), with no association to good antihistamine response (p = 0.55).
Conclusions: Angioedema in CSU is associated with higher disease activity, autoimmune status, and prolonged disease duration but not with differences in antihistamine response. Its presence marks a more severe phenotype, emphasizing the need for careful monitoring and individualized management.
Chronic spontaneous urticaria (CSU) is a multifaceted, heterogeneous dermatological disorder characterized by the spontaneous and recurrent appearance of wheals (hives), angioedema, or both, persisting for a minimum of six weeks in the absence of identifiable external triggers [1, 2]. The condition represents a significant public health burden due to its high prevalence and its marked impact on patients’ quality of life [3]. Patients frequently experience intense pruritus, disfiguring skin changes, and unpredictable symptom recurrence, which can lead to sleep disturbance, emotional distress, impaired work productivity, and social withdrawal [4, 5].
Angioedema, defined as sudden, pronounced [6] and transient swelling of the deep dermis, mucosa, or subcutaneous tissues, most frequently involves the lips, eyelids, face, extremities, and, in some cases, the upper airway [6, 7]. It is observed in 29.4–44.5% of patients with CSU, with approximately 5–10% presenting with angioedema in the absence of wheals [7–9]. These episodes can be particularly distressing due to their disfiguring nature and their unpredictable onset [9, 10].
The underlying pathophysiology involves activation and degranulation of cutaneous mast cells and basophils, leading to the release of histamine and other proinflammatory mediators [9]. Angioedema, when present in CSU, reflects deeper dermal and submucosal vascular leakage, primarily mediated by histamine, though additional pathways such as bradykinin and complement activation may contribute in some cases [8–10]. The coexistence of urticaria and angioedema likely represents overlapping but distinct pathogenic mechanisms, differing in mediator profile, vascular involvement, and tissue depth [9, 10].
Multiple studies have indicated that CSU with concomitant angioedema is associated with greater disease severity, longer disease duration, and poorer treatment responsiveness [7–9, 11]. Furthermore, CSU demonstrates a highly variable duration, ranging from several months to many years, with angioedema frequently emerging as a potential marker for prolonged disease course [9–11].
A growing availability of evidence suggests that autoimmunity—specifically the presence of circulating autoantibodies in approximately 40–50% of patients plays a key role in the pathogenesis of CSU [12]. Several reports have shown higher autologous serum skin test (ASST) positivity among CSU patients with angioedema, indicating that angioedema may serve as a clinical marker of autoimmunity in CSU [13–17], though this association requires further investigation. Angioedema may serve as a surrogate clinical marker pointing to the potential underlying autoimmune mechanisms, but its particular role remains to be clarified in future studies [18–24].
Participants were ≥ 18 years of age, fulfilling diagnostic criteria of a confirmed diagnosis of active CSU based on the EAACI/GA²LEN/EDF/WAO 2022 guideline [1]. Active CSU was defined as the spontaneous development of wheals, angioedema, or both, persisting for at least six consecutive weeks without a known external trigger. Exclusion criteria included the presence of any form of inducible urticaria (cold, cholinergic, or delayed pressure urticaria, etc.), or bradykinin-mediated angioedema [25–27].
This study was originally designed to investigate 230 CSU patients as a whole. Angioedema was included as one of the parameters within the broader study.
Although conducted at the Dermatology Department of General Hospital 8th September in Skopje, the center serves as a referral hospital, and the cohort included patients from across North Macedonia.
The study population included patients of various ethnic backgrounds, including ethnic Macedonians, Albanians, Turks, and Roma, reflecting the multiethnic composition of North Macedonia. Ethnicity was not a factor in recruitment, and no significant differences in CSU characteristics were observed between ethnic groups.
At baseline, demographic characteristics (age, sex), disease history (age at onset, disease duration), atopic background, presence of autoimmune comorbidities, and prior or ongoing treatments were recorded in a standardized case report form.
Disease activity was quantified using the Urticaria Activity Score over 7 days (UAS7), integrating daily wheal counts and itch severity scores collected over 7 days. UAS7 categories were as follows: severe (28–42), moderate (16–27), mild (7–15), well-controlled (1–6), and asymptomatic (0) [6].
Treatment response was assessed at follow-up visits. A responder was defined as achieving a UAS7 ≤ 7 while taking up to 4 tablets/day of a non-sedating H1-antihistamine. Non-responders were those with persistent disease activity (UAS7 > 7) despite similar or escalated antihistamine dosing [6].
Disease duration was measured as the time elapsed between the onset of the first urticaria symptoms and the date of inclusion. Recurrence was defined as the reappearance of wheals and/or angioedema after a remission period of ≥ 6 months [6].
The autoimmune status was proven by a previously confirmed autoimmune disease based on medical record review or serological positivity for at least one autoimmune marker: anti-thyroid peroxidase (anti-TPO) antibodies, antinuclear antibodies (ANA), or rheumatoid factor (RF) [6, 28–30]. This stratification allowed for the identification of the potential immunopathogenic disease subtypes.
The ASST was performed to detect in vivo autoreactivity. To minimize false-negative results, participants were instructed to discontinue antihistamines for at least 48 hours, H2-receptor antagonists or leukotriene receptor antagonists for 7 days, and systemic corticosteroids or cyclosporine for at least 1 month before testing [30–32].
Approximately 5 mL of venous blood was collected from each patient under aseptic conditions using standard venipuncture techniques. The samples were allowed to clot at room temperature for 30 min. Following clot formation, the specimens were centrifuged at 2,000 × g for 15 min at room temperature to separate the serum from cellular components [31, 32].
The procedure involved intradermal injection of 0.5 mL autologous serum into the volar forearm, with histamine (positive control) and physiological saline (negative control) injected at separate sites. Readings were taken 30 min post-injection. A positive ASST was defined as a serum-induced wheal exceeding the saline control by more than 1.5 mm in mean diameter [31, 32].
Data were analyzed using SPSS version 23 (IBM Corp., Armonk, NY, USA). Continuous variables were first tested for normality using the Kolmogorov-Smirnov and Shapiro-Wilk tests. For normally distributed data, comparisons between two groups were made using the Student’s t-test, and between more than two groups using one-way ANOVA. For non-normally distributed data, the Mann-Whitney U test or Kruskal-Wallis test was applied as appropriate.
Categorical variables were compared using the Chi-square test or Fisher’s exact test when expected counts were below five. All statistical tests were two-tailed, and a p-value < 0.05 was considered statistically significant [33].
In the present cohort, angioedema was observed in 70% (n = 161) of CSU patients. When stratifying patients according to UAS7 categories, the highest prevalence of angioedema was recorded among those with severe CSU disease activity (82.02%) (Table 1). This proportion was not only markedly elevated but also statistically significant when compared to patients with moderate disease, mild disease, and well-controlled CSU (p < 0.05 for all).
Disease activity in CSU and angioedema.
| Variable | UAS7 disease activity in CSU | |||||
|---|---|---|---|---|---|---|
| n | Severen (%) | Moderaten (%) | Mildn (%) | Well-controlledn (%) | No symptomsn (%) | |
| Angioedema | ||||||
| Present | 161 | 73 (82.02) | 34 (65.38) | 31 (65.96) | 10 (45.45) | 13 (65.00) |
| Not present | 69 | 16 (17.98) | 18 (34.62) | 16 (34.04) | 12 (54.55) | 7 (35.00) |
| p-level | ||||||
| severe/moderate | χ2 = 4.9, *p = 0.026 | |||||
| severe/mild | χ2 = 4.4, *p = 0.036 | |||||
| severe/well-controlled | χ2 = 12.5, *p = 0.0004 | |||||
CSU: chronic spontaneous urticaria; UAS7: Urticaria Activity Score over 7 days; *p < 0.05. Adapted from the author’s original, unpublished thesis data.
When evaluating the relationship between therapeutic response to H1-antihistamines—as defined by achieving a UAS7 score below 7 while on a daily dose of one to four tablets—no statistically significant difference emerged in the frequency of angioedema between treatment responders and non-responders (Table 2). Specifically, the occurrence of angioedema remained comparably high in both groups.
Therapeutic response to H1-antihistamines and angioedema.
| Variable | Therapeutic response to H1-antihistamines | p-level | ||
|---|---|---|---|---|
| n | Presentn (%) | Not presentn (%) | ||
| Angioedema | ||||
| Present | 161 | 116 (71.17) | 45 (67.16) | χ2 = 0.36, p = 0.55 |
| Not present | 69 | 47 (28.83) | 22 (32.84) | |
Adapted from the author’s original, unpublished thesis data.
A particularly notable finding emerged in the context of autoimmune status. Patients with serological or clinical evidence of autoimmunity—defined by the presence of anti-TPO antibodies, ANA, RF, or a documented autoimmune disease—showed a significantly higher prevalence of angioedema compared with absent status (Table 3).
Autoimmune status and angioedema.
| Variable | Autoimmune status | p-level | ||
|---|---|---|---|---|
| n | Positiven (%) | Negativen (%) | ||
| Angioedema | ||||
| Present | 161 | 109 (75.17) | 52 (61.18) | χ2 = 4.99, *p = 0.025 |
| Not present | 69 | 36 (24.83) | 33 (38.82) | |
*p < 0.05. Adapted from the author’s original, unpublished thesis data.
Analysis of ASST reactivity, an in vivo surrogate marker of autoreactivity, demonstrated a numerical trend toward higher angioedema prevalence in ASST-positive patients compared with their ASST-negative counterparts (Table 4). However, these differences failed to reach statistical significance across all subgroup comparisons.
Autologous serum skin test (ASST) test and angioedema.
| Variable | Autoimmune status | p-level | ||
|---|---|---|---|---|
| n | Positiven (%) | Negativen (%) | ||
| Angioedema | ||||
| Present | 161 | 101 (72.14) | 60 (66.67) | χ2 = 0.80, p = 0.38 |
| Not present | 69 | 39 (27.86) | 30 (33.33) | |
Adapted from the author’s original, unpublished thesis data.
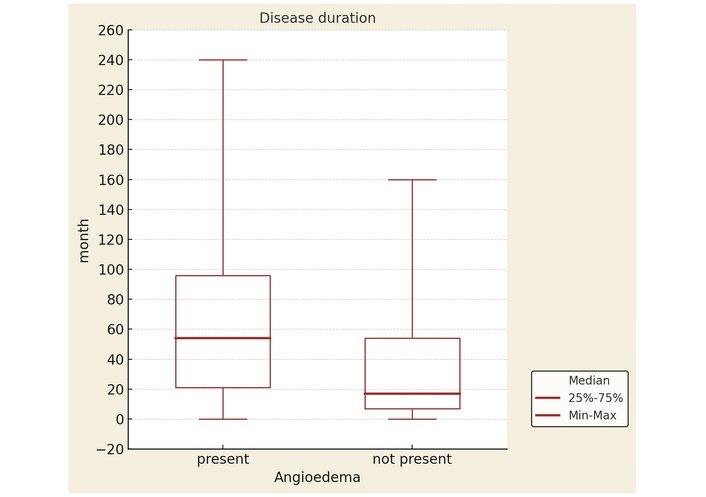
Patients with a history of angioedema reported significantly longer CSU duration than patients without angioedema (Figure 1).
The reported statistics reflect the entire CSU patient population rather than focusing solely on patients with angioedema. Future analyses are planned to generate dedicated statistics specifically for the subgroup of angioedema patients.
The present study provides robust evidence that angioedema in CSU is not merely a co-occurring symptom but a clinically meaningful marker associated with increased disease severity, an autoimmune predisposition, and prolonged disease persistence. In contrast, its frequency appears largely independent of patient responsiveness to H1-antihistamines or ASST reactivity, underscoring the need for clinicians to treat angioedema as a distinct, prognostically relevant domain of CSU. By contextualizing our findings against established literature, we highlight converging evidence from multiple independent cohorts and identify critical areas where existing data remain inconclusive.
In our cohort, angioedema was present in 82.02% of patients with severe CSU activity, markedly higher than in those with moderate (65.38%, p = 0.026), mild (65.96%, p = 0.036), or well-controlled disease (45.45%, p = 0.0004). This strong gradient across severity levels, with an estimated odds ratio (OR) of ~5.48 for severe versus well-controlled disease, parallels findings from Sussman et al. [17] and Örnek Özdemir et al. [10], both of whom reported prevalence rates of high prevalence rates in severe CSU. Our data reinforce these reports, extending their implications by demonstrating that angioedema frequency scales proportionally with disease activity even within stratified severity categories. This consistency across studies supports angioedema’s role as a high-value clinical marker for identifying patients with a more aggressive CSU phenotype.
Strikingly, even among patients in clinical remission—defined by the absence of active wheals—more than half reported previous or intermittent episodes of angioedema. This mirrors the longitudinal observations of several studies [7–9], which documented that angioedema can recur or persist independently of urticarial wheals, sometimes becoming the sole clinical manifestation in quiescent phases of disease. Our findings, therefore, underscore that disease control, as traditionally measured by UAS7, may underestimate the ongoing morbidity in patients with a history of angioedema. This has direct clinical implications: patients achieving wheal suppression should still be monitored specifically for angioedema recurrence, as its presence may signal persistent subclinical inflammatory activity.
When comparing antihistamine responders and non-responders, the rates of angioedema were statistically indistinguishable (71.17% vs. 67.16%, p = 0.55). This aligns with Kaplan’s conclusions [26] that standard-dose and even up-dosed second-generation H1-antihistamines often fail to control angioedema effectively, despite reducing pruritus and wheal formation. Our results, together with Kaplan’s, suggest that histamine-mediated pathways may not be the sole drivers of angioedema in CSU. Instead, alternative mediators—such as bradykinin, platelet-activating factor, or complement-derived anaphylatoxins—may play a larger role, thereby justifying early consideration of biologic therapies like omalizumab or emerging agents targeting IgE, IL-4Rα, or Siglec-8 [11].
The presence of autoimmunity—defined by positive anti-TPO, ANA, or RF serology or confirmed autoimmune disease—was associated with a significantly higher angioedema prevalence (75.17% vs. 61.18%, p = 0.025; RR ≈ 1.23). This finding resonates with Kolkhir et al. [30] and Kocatürk et al. [13], who reported that autoimmune CSU subtypes typically exhibit greater symptom burden, higher recurrence rates, and more prolonged disease courses. Our study not only corroborates these associations but also quantifies the relative risk specific to angioedema, strengthening the hypothesis that immune dysregulation underpins both superficial wheal formation and deeper dermal or submucosal swelling. The autoimmune link suggests that immune-modifying treatments—rather than purely symptomatic regimens—may be particularly warranted in this subgroup.
Although angioedema was numerically more frequent among ASST-positive patients (72.14%) than ASST-negative ones (66.67%), the difference was not statistically significant (OR: 1.30, p = 0.34). These results reflect the mixed evidence reported in prior studies: while some investigators have identified ASST positivity as a marker of more severe or treatment-resistant disease [34–39], others have failed to find consistent predictive value [12]. The absence of statistical significance in our analysis may reflect limited power for this endpoint or heterogeneity in the underlying pathomechanisms of ASST reactivity. Nevertheless, the numerical trend warrants further investigation in larger, multi-center cohorts.
Perhaps the most clinically consequential observation is the strong association between angioedema and prolonged disease duration. Patients with a history of angioedema experienced CSU for an average of 61.7 ± 46.2 months (median 54 months), compared to 35.4 ± 39.2 months (median 17 months) in those without angioedema (p = 0.000012; Cohen’s d ≈ 0.59). This corresponds closely to the ~2-year increase in disease persistence reported by different authors [6, 38, 39]. Our regression analysis further confirmed angioedema as an independent predictor of disease duration (β = 0.34, p < 0.001), suggesting it may serve as an early prognostic indicator for identifying patients at risk for chronicity. From a management perspective, such patients may benefit from earlier escalation of therapy and more intensive long-term follow-up.
In conclusion, although this study was designed to investigate CSU as a whole, with angioedema included as one of its parameters, our findings—when considered alongside existing evidence—reinforce angioedema’s role as a marker of severe, autoimmune-associated, and persistent CSU. Unlike wheals, its occurrence appears largely resistant to conventional antihistamine therapy, underscoring an unmet therapeutic need. Future research should aim to elucidate the molecular mediators specific to angioedema and develop targeted interventions to mitigate its clinical and prognostic impact.
Given these associations, patients presenting with angioedema—especially those with autoimmune markers—may benefit from early escalation beyond H1-antihistamines, including omalizumab or cyclosporine [11, 34–41]. Routine autoimmune screening could support prognosis and therapeutic decisions.
A limitation of this study is that the data for angioedema were derived from a larger CSU cohort rather than exclusively from angioedema patients; consequently, the current statistics reflect the overall CSU population and may not fully capture characteristics unique to angioedema. Dedicated analyses focusing only on angioedema patients will be needed in future research to provide more precise insights.
The cross-sectional design limits causal inference, particularly regarding whether angioedema prolongs CSU or reflects more severe phenotypes. Being a single-center study, the findings may not generalize to diverse populations with differing genetic and environmental backgrounds.
An additional limitation of this study is the absence of treatment arms involving second-line or third-line agents such as omalizumab or cyclosporine, which are recommended in current guidelines for patients with refractory CSU. By restricting the therapeutic response analysis to H1-antihistamines, we were unable to assess whether angioedema persistence in our cohort reflects true pharmacologic resistance across treatment classes or merely inadequate exposure to advanced therapies. Furthermore, we did not systematically document or control for concomitant treatments targeting non-allergic comorbidities (e.g., ACE inhibitors, hormonal therapies, or systemic anti-inflammatory agents) that may independently precipitate or exacerbate angioedema. This omission introduces potential confounding, as such medications and comorbid conditions could influence the frequency, severity, or chronicity of angioedema episodes in CSU, thereby biasing observed associations.
Lastly, the absence of standardized disease activity and control measures, such as the Angioedema Activity Score (AAS) and the Urticaria Control Test (UCT), represents a further limitation. Without these validated tools, the assessment of symptom burden and disease control relied on non-standardized clinical impressions, potentially reducing the accuracy and comparability of our findings.
This study was originally designed to investigate CSU as a whole, with angioedema included as one of its parameters. Our findings refer to angioedema be a pivotal clinical indicator within the spectrum of CSU, consistently linked to higher disease severity, autoimmune reactivity, and markedly prolonged disease duration. Notably, the persistence of angioedema into remission phases, independent of wheals, reinforces its role as a chronic and burdensome component of CSU. The absence of significant differences between antihistamine responders and non-responders, together with the limited predictive value of ASST reactivity, suggests that current first-line and diagnostic paradigms may insufficiently address angioedema-specific disease mechanisms. By systematically quantifying angioedema prevalence and its associations, this study emphasizes the necessity of integrating angioedema assessment into routine CSU evaluation, both for active disease management and for long-term monitoring. Importantly, these results call for targeted interventional studies incorporating advanced agents such as omalizumab or cyclosporine, and for careful consideration of comorbidity-related contributors to angioedema persistence. Refining therapeutic strategies in this manner may not only improve disease control but also significantly reduce the sustained quality-of-life impairment experienced by this patient population.
ANA: antinuclear antibodies
anti-TPO: anti-thyroid peroxidase
ASST: autologous serum skin test
CSU: chronic spontaneous urticaria
OR: odds ratio
RF: rheumatoid factor
UAS7: Urticaria Activity Score over 7 days
VT: Conceptualization, Investigation, Writing—original draft, Writing—review & editing, Formal analysis, Visualization. NTM: Validation, Writing—review & editing, Supervision. EK: Validation, Writing—review & editing, Supervision. DF: Validation, Writing—review & editing, Supervision. HB: Validation, Writing—review & editing, Supervision. DBI: Writing—review & editing, Supervision. ID: Investigation, Validation, Supervision. ARD: Investigation, Validation, Supervision. IT: Investigation, Validation, Supervision. SP: Validation, Writing—review & editing. KTS: Validation, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that there are no conflicts of interest.
The study was approved by the Ethics Committee of General Hospital 8th September, Skopje, North Macedonia. Ethical approval number: 2796. The study complies with the Declaration of Helsinki.
Informed consent to participate in the study was obtained from all participants.
Not applicable.
The datasets analyzed during this study are available from the corresponding author on reasonable request.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Liron Lerner ... Katarina Stevanovic