 Review
Review

Affiliation:
1Department of Community Health Sciences, Sohail University, Karachi 74000, Pakistan
Email: mhhammad497@gmail.com
ORCID: https://orcid.org/0000-0001-8894-3692
Affiliation:
2Department of Pharmaceutical Sciences, Riphah International University, Islamabad 46000, Pakistan
Affiliation:
3HBS Medical and Dental College, Islamabad 45550, Pakistan
ORCID: https://orcid.org/0009-0006-6388-8571
Explor Neuroprot Ther. 2026;6:1004162 DOI: https://doi.org/10.37349/ent.2026.1004162
Received: March 13, 2026 Accepted: May 18, 2026 Published: July 07, 2026
Academic Editor: Claudio Viegas-Junior, Federal University of Alfenas, Brazil
The article belongs to the special issue Neuro-Inflammation as a Target in the Design of Multifunctional Drug Candidates for Neurodegenerative Diseases
Neurodegenerative and neurodevelopmental neurological disorders represent a growing global health burden, characterized by progressive neuronal dysfunction, cognitive decline, and impaired functional outcomes. Increasing evidence highlights neuroinflammation as a central pathophysiological mechanism linking mitochondrial dysfunction, oxidative stress, microbiota dysbiosis, and synaptic impairment across diverse neurological conditions. This narrative review was conducted using a structured literature search approach, incorporating major biomedical databases to enhance transparency and reproducibility. This review synthesizes contemporary evidence on mechanistic pathways underlying neuroinflammation-mediated neurodegeneration and critically evaluates emerging neuroprotective therapeutic strategies. Particular emphasis is placed on mitochondrial transfer approaches, novel circulating and imaging biomarkers, and integrative neurotechnological innovations such as artificial intelligence-driven neuroimaging analytics. While several therapeutic approaches demonstrate promise in preclinical models, most remain at early experimental or translational stages, with limited validation in large-scale human studies. Current findings suggest that targeting neuroimmune signaling cascades, restoring mitochondrial bioenergetics, and modulating gut-brain axis interactions may provide synergistic neuroprotective benefits. The review proposes a multidimensional precision-medicine framework incorporating biomarker-guided therapeutic selection and interdisciplinary care models. Future research priorities include longitudinal biomarker validation, randomized clinical trials of mitochondrial-based therapies, and integration of digital neurodiagnostic platforms to enhance early disease detection. Despite these advances, significant gaps remain in clinical translation, standardization of biomarkers, and long-term therapeutic safety, necessitating cautious interpretation of emerging evidence.
Neurological disorders represent a primary and escalating driver of global morbidity, mortality, and disability-adjusted life years, impacting patients across the entire developmental spectrum [1–3]. Collectively, neurodegenerative diseases, neurodevelopmental disorders, and acute brain injuries impose substantial clinical, social, and economic strains on international healthcare systems [4]. Beyond their immediate clinical presentation, these conditions drive extensive long-term disability and caregiver burden while severely diminishing quality of life; this is especially pronounced in low- and middle-income regions where specialized neurological infrastructure is often scarce [5, 6]. As global populations age, the prevalence of neurodegenerative conditions continues to rise, which underscores an urgent clinical requirement for improved early diagnostic and preventive frameworks [7]. While foundational research originally focused on neuron-centric disease models, modern evidence now favors a systems-level architecture that integrates neuroimmune, metabolic, and environmental variables [8, 9].
Perspective reflects a growing consensus that neuronal dysfunction is not an isolated event but rather a consequence of complex cellular cross-talk, systemic inflammation, and external triggers such as toxins, infection, or lifestyle [10, 11]. Such integrative models have redefined our understanding of pathogenesis and broadened the horizon for therapeutic intervention. Among these processes, neuroinflammation has emerged as a central mediator linking acute neuronal injury with chronic neurodegenerative cascades [12–14]. Crucially, neuroinflammation is not a monolithic response; while acute inflammatory signals can be protective and aid in tissue repair, chronic and unresolved inflammation tends to fuel progressive neuronal decay [15]. The failure of inflammatory resolution, often characterized by a deficiency in pro-resolving mediators, is now recognized as a fundamental driver of persistent neurodegeneration [16–18]. Current data suggest that when inflammation fails to resolve in a timely manner, the resulting sustained activation of microglia and astrocytes creates a self-amplifying cycle of neurotoxicity and synaptic failure. This maladaptive process is increasingly being linked to both the prodromal and advanced stages of neurological disease [19].
Activation of microglia and astrocytes initiates a release of pro-inflammatory cytokines and reactive oxygen species, which ultimately destabilizes synaptic homeostasis and triggers neuronal apoptosis [20]. This is further complicated by mitochondrial dysfunction, which heightens oxidative stress and leads to metabolic exhaustion [21]. Furthermore, impaired mitochondria do more than just create energy deficits; they actively modulate innate immune signaling, thereby reinforcing inflammatory pathways. This bidirectional relationship between mitochondrial health and neuroinflammation represents a vital, high-impact nexus in the pathophysiology of these disorders [22].
Seminal investigations have identified overlapping neuroinflammatory signatures between conditions like Alzheimer’s and Parkinson’s disease, yet more recent work emphasizes disease-specific inflammatory profiles, which highlights the inherent heterogeneity of neuroimmune responses [23, 24]. Such diversity suggests that any therapeutic strategy targeting neuroinflammation must be precisely calibrated to the specific disease context, accounting for cellular mediators, temporal changes, and individual patient variables like age or genetic risk. While emerging translational research points toward promising avenues, including AI-enhanced neuroimaging and precision diagnostic approaches, many of these technologies remain in the experimental phase [25]. Significant hurdles remain regarding scalability, regulatory hurdles, and the reproducibility of results [26]. Furthermore, the lack of extensive clinical validation, along with ethical concerns and high costs, continues to slow the transition of these innovations from the lab to routine clinical care, emphasizing the need for continued, rigorous translational evidence.
To enhance methodological transparency and mitigate potential selection bias, this narrative review utilized a structured and reproducible approach to the literature search. We systematically queried primary electronic databases, specifically PubMed, Scopus, and Web of Science, to identify relevant peer-reviewed studies published between January 2000 and March 2026.
The search strategy was constructed using a rigorous combination of controlled vocabulary and free-text terms to ensure both depth and precision. Core search strings focused on “neuroinflammation,” “mitochondrial dysfunction,” “neurodegeneration,” “biomarkers,” “gut-brain axis,” and “artificial intelligence in neurology.” These terms were strategically integrated using Boolean operators (AND, OR, NOT) to maximize the sensitivity of the retrieval process while maintaining specific relevance to the review’s objectives. Beyond these automated database queries, we performed a manual screening of reference lists from seminal articles and high-impact reviews. This secondary search phase was critical for capturing foundational literature and ensuring the comprehensive scope necessary for a high-impact synthesis of the field.
Studies were considered eligible if they met the following criteria:
(i) Original research articles, systematic reviews, or meta-analyses.
(ii) Focus on neuroinflammatory mechanisms, neurodegeneration, or neuroprotective strategies.
(iii) Inclusion of translational, clinical, or mechanistic insights relevant to neurological disorders.
Both seminal foundational studies and recent high-impact publications were included to ensure a balanced representation of the historical evolution and current advancements in the field.
Studies were excluded if they:
(i) Lacked relevance to neuroinflammation or neuroprotection.
(ii) Non-peer-reviewed articles or conference abstracts without full text.
Although this study was designed as a narrative review rather than a formal systematic review, the selection process followed a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-informed framework to improve transparency and reproducibility. Articles were screened based on relevance, methodological rigor, and translational significance. The final selection prioritized studies that provided mechanistic insights, clinical applicability, or emerging therapeutic relevance, enabling a critical synthesis rather than a purely descriptive summary as shown in Figure 1.
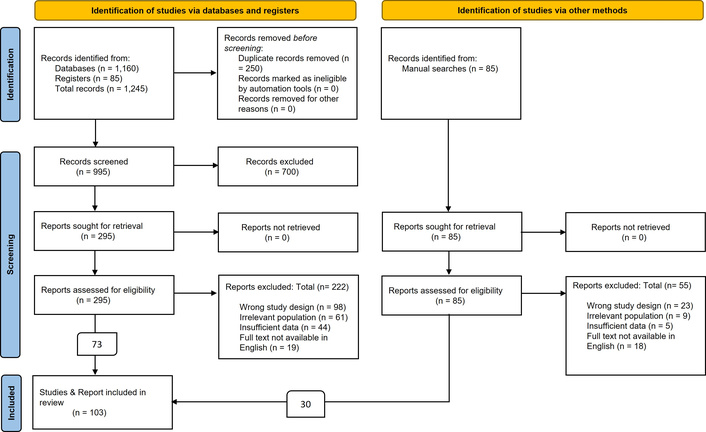
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-informed flow diagram illustrating the identification, screening, eligibility assessment, and inclusion of studies in this narrative review. Adapted from https://www.prisma-statement.org/prisma-2020-flow-diagram. Accessed Feb 22, 2026. Distributed under a Creative Commons Attribution (CC BY 4.0) license.
Neuroinflammation serves as a sophisticated, dynamic biological response characterized by intricate interactions between glial cells, immune mediators, and neuronal signaling pathways, as illustrated in Figure 2. It is vital to recognize that neuroinflammation is not a uniformly detrimental process; indeed, acute and transient inflammatory responses are indispensable for maintaining neural homeostasis, facilitating tissue repair, and clearing cellular debris following an insult. Conversely, chronic and dysregulated neuroinflammation fosters sustained neuronal stress, synaptic impairment, and progressive neurodegeneration [27, 28]. Distinguishing between these states is fundamental to both the understanding of disease pathophysiology and the engineering of targeted therapeutic interventions.
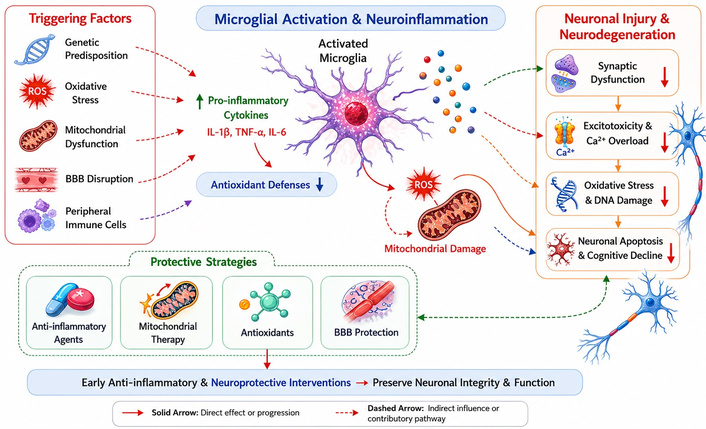
Pathophysiological mechanisms linking neuroinflammation to neuronal injury and neurodegeneration. This figure illustrates the key molecular and cellular pathways through which neuroinflammation contributes to neuronal dysfunction and progressive neurodegeneration, including microglial activation, pro-inflammatory cytokine release, oxidative stress, mitochondrial impairment, and synaptic damage. These interconnected processes highlight neuroinflammation as a central therapeutic target in neurological disorders. BBB: blood-brain barrier; ROS: reactive oxygen species; TNF-α: tumor necrosis factor alpha.
Persistent activation of microglia results in a sustained release of pro-inflammatory cytokines, chemokines, and reactive oxygen species, which collectively destabilize synaptic homeostasis and drive neuronal damage [29]. Experimental and preclinical data have shown that the prolonged elevation of key inflammatory mediators, specifically interleukin-1β and tumor necrosis factor-α impairs synaptic plasticity, alters neurotransmitter signaling, and disrupts memory-related neural circuits [30]. However, emerging evidence also indicates that tightly regulated inflammatory signaling may support synaptic remodeling and neuroplasticity, which highlights the nuanced, context-dependent, and often dual role of neuroinflammation within the central nervous system.
Oxidative stress further compounds neuronal injury through lipid peroxidation, mitochondrial membrane damage, and genomic instability [31]. Furthermore, mitochondrial dysfunction and neuroinflammation are inextricably linked, forming a self-propagating cycle where mitochondrial decay enhances inflammatory signaling, while those same inflammatory mediators further compromise mitochondrial bioenergetics. This bidirectional relationship serves as a central mechanism underlying neuronal vulnerability and the overall progression of the disease [32, 33].
Crucially, the susceptibility to neuroinflammatory damage is not uniform across the brain. Metabolically active regions, such as the hippocampus and cortex, exhibit heightened vulnerability due to their substantial energy requirements and heavy reliance on efficient mitochondrial function [34]. Selective vulnerability helps explain the characteristic patterns of neurodegeneration seen in conditions like Alzheimer’s disease [35]. Moreover, these neuroinflammatory responses are shaped by biological and demographic variables, including age, sex, and developmental stage. Recent findings highlight sex-specific differences in microglial activation and cytokine expression, which may partially account for the variations in disease prevalence between males and females [36]. Similarly, the developmental stage is a critical factor; immature neural systems show an increased sensitivity to inflammatory insults, while the aging process is typically associated with chronic, low-grade inflammation that predisposes the brain to neurodegeneration [37]. Taken together, these observations underscore the profound complexity and heterogeneity of neuroinflammatory processes, emphasizing the necessity for context-specific, precision-based therapeutic strategies that target neuroimmune pathways.
Mitochondria play a central role in neuronal survival, energy metabolism, and cellular homeostasis [38]. However, their function extends beyond adenosine triphosphate (ATP) production, encompassing regulation of apoptosis, calcium signaling, and redox balance, all of which are critical in maintaining neuronal integrity [39]. Beyond bioenergetic failure, alterations in mitochondrial dynamics, including imbalances in fusion and fission processes, have been increasingly implicated in neurodegenerative pathology [40].
Disruptions in these processes impair mitochondrial quality control mechanisms, leading to the accumulation of dysfunctional mitochondria and heightened neuronal vulnerability [41]. Mitochondrial dysfunction leads to reduced ATP production and increased oxidative stress [42]. This bioenergetic deficit, coupled with excessive generation of reactive oxygen species, contributes to lipid peroxidation, DNA damage, and activation of pro-apoptotic pathways, thereby accelerating neuronal degeneration [43]. Importantly, mitochondrial dysfunction is closely linked with neuroinflammatory processes, forming a bidirectional feedback loop that amplifies cellular injury [44]. While mitochondrial transfer has shown promise in preclinical studies, its clinical applicability remains highly constrained due to delivery challenges, immunogenic risks, and a lack of standardized protocols [45].
Although experimental models demonstrate restoration of cellular bioenergetics following mitochondrial transplantation, translation into clinical practice remains limited by technical complexity, safety concerns, and ethical considerations. Notably, no large-scale randomized controlled trials have yet validated its efficacy or long-term safety in human populations [46]. Moreover, heterogeneity in mitochondrial quality and donor-recipient compatibility presents a significant translational barrier. Variability in mitochondrial integrity, along with potential immune incompatibility, further complicates therapeutic standardization and reproducibility across studies [47].
Pharmacological activation of mitochondrial biogenesis pathways offers an alternative strategy [48]. Agents targeting pathways such as peroxisome proliferator-activated receptor gamma coactivator-1 alpha (PGC-1α) activation have shown potential in enhancing mitochondrial function; however, current evidence is derived largely from small-scale or preclinical studies with inconsistent outcomes. Consequently, there remains a critical need for well-designed, large-scale clinical trials to establish efficacy, optimize therapeutic protocols, and determine long-term safety [49, 50]. Collectively, these limitations highlight the gap between experimental promise and clinical applicability in mitochondrial-targeted therapies (Figure 3).
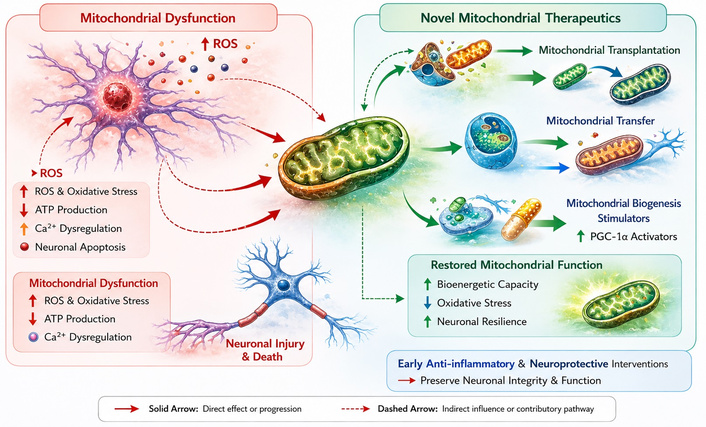
Mitochondrial dysfunction-mediated neuronal injury and emerging mitochondrial-targeted therapeutic strategies. This figure illustrates the central role of mitochondrial dysfunction in neuronal injury. Impaired mitochondrial function results in increased reactive oxygen species (ROS) production and oxidative stress, reduced adenosine triphosphate (ATP) generation, and dysregulation of intracellular calcium (Ca2+), ultimately leading to neuronal apoptosis and neurodegeneration. The left panel depicts these pathological processes contributing to neuronal injury and cell death. The right panel highlights emerging mitochondrial-targeted therapeutic strategies aimed at restoring cellular homeostasis. These include mitochondrial transplantation and mitochondrial transfer to replace or augment damaged mitochondria, as well as stimulation of mitochondrial biogenesis through activation of pathways such as peroxisome proliferator-activated receptor gamma coactivator-1 alpha (PGC-1α). Collectively, these interventions enhance bioenergetic capacity, reduce oxidative stress, and improve neuronal resilience. Overall, the figure emphasizes the potential of early anti-inflammatory and neuroprotective interventions targeting mitochondrial dysfunction to preserve neuronal integrity and function and mitigate disease progression.
Early identification of neurodegenerative processes remains a major challenge in contemporary neurological practice, as clinical symptoms often manifest only after substantial and often irreversible neuronal damage has already occurred [51]. This diagnostic delay highlights a fundamental limitation of symptom-based neurological assessment and underscores the urgent need for reliable, validated, and disease-specific biomarkers capable of detecting preclinical pathological changes [52]. In recent years, advances in biomarker research have provided promising avenues for detecting early pathological alterations and facilitating timely therapeutic intervention. Among the most widely investigated circulating biomarkers is neurofilament light chain, a structural axonal protein released into cerebrospinal fluid and peripheral blood following neuronal injury [53].
Although neurofilament light chain has demonstrated strong sensitivity for axonal damage, its specificity remains limited, as elevated levels have been observed across multiple neurological conditions, including inflammatory, traumatic, and neurodegenerative disorders [54]. This limitation reduces its utility as a standalone diagnostic marker. Elevated levels of inflammatory mediators, including specific cytokine profiles, have also been associated with neuroinflammatory activation and progressive neuronal dysfunction. Moreover, mitochondrial-derived biomarkers such as circulating mitochondrial DNA fragments are gaining recognition as potential indicators of impaired cellular bioenergetics and oxidative stress-related neuronal damage [55]. However, the clinical validity of these mitochondrial biomarkers remains in early stages of investigation, with variability in assay methods and a lack of standardized reference thresholds across populations [56].
Complementing biochemical indicators, neuroimaging biomarkers provide valuable insights into early functional and structural brain alterations. Advanced magnetic resonance imaging (MRI) techniques have demonstrated the ability to detect subtle changes in functional connectivity, cortical thickness, and white matter integrity prior to overt clinical decline [57]. Nevertheless, heterogeneity in imaging protocols, acquisition parameters, and analytical frameworks continues to limit reproducibility and cross-study comparability, posing challenges for clinical translation [58]. The integration of multimodal biomarker platforms combining molecular, genetic, and imaging data may enhance disease risk stratification, enable longitudinal therapeutic monitoring, and support the development of precision neuroprotective strategies [59]. In pediatric populations, early biomarker-based screening holds particular significance, as timely identification of neurodevelopmental vulnerability may facilitate targeted interventions, optimize neurocognitive outcomes, and reduce long-term neurological disability [60]. Overall, while biomarker research represents a rapidly advancing field, substantial gaps remain in validation, standardization, and clinical implementation, necessitating large-scale longitudinal studies and harmonized methodological frameworks.
Emerging evidence underscores the critical and increasingly recognized role of the gut-brain axis in regulating neurological health, with the intestinal microbiota acting as a key modulator of neuroimmune, neuroendocrine, and neuroinflammatory signaling pathways, as shown in Figure 4. This bidirectional communication network between the central nervous system and the gastrointestinal tract has shifted traditional neurobiological paradigms by introducing the microbiome as an active participant in brain function rather than a passive environmental factor [61].
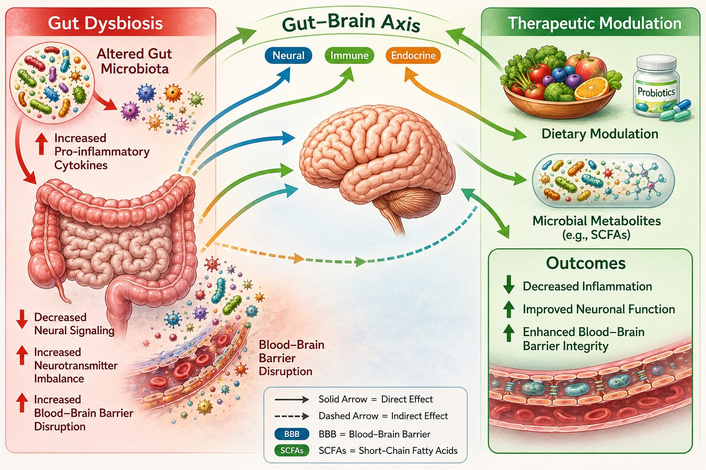
Gut-brain axis and microbiota-driven mechanisms of neuroprotection. This figure demonstrates the bidirectional communication between the gut microbiota and the central nervous system through neural, immune, and endocrine pathways. It highlights the role of microbial metabolites, inflammatory mediators, and blood-brain barrier integrity in regulating neuroinflammation and neuronal health, as well as potential therapeutic interventions including probiotics, prebiotics, and dietary modulation.
Dysbiosis, or imbalance in the microbial ecosystem, has been linked to multiple pathological mechanisms, including altered neurotransmitter synthesis, heightened systemic and central inflammation, and disruption of blood-brain barrier integrity. These alterations contribute to neuronal dysfunction, synaptic impairment, and increased vulnerability to both neurodevelopmental and neurodegenerative disorders [62, 63]. However, it is important to note that much of the current evidence is associative or derived from animal models, limiting direct causal inference in human neurological disease. Variability in microbiome composition across populations further complicates generalizability [64].
Bidirectional communication between the gut and the central nervous system is mediated through neural (vagus nerve signaling), immune, metabolic, and endocrine pathways, highlighting the gut microbiome as an integral component of neurophysiological homeostasis [65]. Recent mechanistic studies have demonstrated that microbial metabolites, including short-chain fatty acids, tryptophan derivatives, and bile acid metabolites, can directly influence microglial activation states, blood-brain barrier permeability, and synaptic plasticity, thereby linking gut-derived signals to central neuroinflammatory processes [66].
Therapeutic modulation of gut microbiota has emerged as a promising neuroprotective strategy. Interventions including dietary modification, prebiotics, probiotics, synbiotics, and supplementation with targeted microbial metabolites such as short-chain fatty acids can restore microbial balance, reduce systemic and neuroinflammation, and support neuronal resilience [67]. Despite encouraging preclinical findings, clinical trials in humans have produced heterogeneous results, with variability in strain selection, dosing regimens, treatment duration, and patient populations contributing to inconsistent outcomes [68]. As a result, standardized therapeutic protocols have not yet been established. These approaches may particularly benefit pediatric populations, as early-life microbiota composition critically influences brain maturation, synaptic plasticity, and cognitive development. Longitudinal cohort studies suggest that early microbial disruption may have long-term consequences on neurodevelopmental trajectories; however, definitive mechanistic pathways remain under investigation. Preclinical studies suggest that microbiota-targeted therapies can attenuate neuroinflammatory cascades, improve behavioral outcomes, and enhance neuroprotective signaling pathways, offering potential translational applications in neurodevelopmental disorders [69].
Moreover, integrating microbiota modulation with other neuroprotective strategies, such as mitochondrial therapies or anti-inflammatory pharmacological agents, may provide synergistic benefits [70]. Integrative therapeutic concept is particularly relevant in complex neurological disorders where multifactorial pathophysiology limits the effectiveness of single-target interventions. However, evidence supporting such combination strategies in clinical settings remains limited and requires rigorous validation [71]. Continued research into microbiome-brain interactions, mechanistic pathways, and longitudinal clinical outcomes is essential to establish evidence-based interventions. Harnessing the gut-brain axis represents a novel frontier in precision neuroprotection, with the potential to improve long-term neurological health across the lifespan [72, 73]. Nevertheless, translational gaps, methodological inconsistencies, and a lack of standardized analytical frameworks remain major barriers to clinical implementation, highlighting the need for large-scale, multicenter, and mechanistically driven human studies.
Recent technological advancements are rapidly transforming the landscape of neurological diagnostics, monitoring, rehabilitation, and therapeutics. Artificial intelligence (AI)-driven neuroimaging analytics has demonstrated substantial potential in detecting subtle structural, functional, and connectivity alterations in the brain that often precede overt clinical symptom manifestation [74, 75]. These developments represent a paradigm shift from conventional diagnostic frameworks, which largely depend on clinical symptomatology, toward data-driven, predictive models capable of identifying preclinical disease states [76].
Machine learning algorithms applied to multimodal imaging data, including MRI, functional MRI, and diffusion tensor imaging, facilitate early identification of at-risk neural networks, offering opportunities for preemptive interventions [77]. However, despite high diagnostic performance in controlled experimental settings, real-world clinical translation remains limited by data heterogeneity, lack of external validation, and variability in imaging acquisition protocols across institutions. In addition, algorithmic bias and limited interpretability of deep learning models pose significant challenges for clinical adoption and regulatory approval [78, 79]. These AI-based tools can enhance diagnostic accuracy, support longitudinal disease monitoring, and optimize individualized treatment planning. Importantly, their true clinical value lies not only in detection but also in their ability to integrate longitudinal patient data, enabling dynamic risk stratification and disease trajectory modeling over time.
Complementing these diagnostic innovations, virtual reality (VR)-assisted neurorehabilitation and digital cognitive monitoring platforms are transforming patient engagement and therapy delivery. VR-based interventions enable immersive, task-specific training that promotes neuroplasticity, motor recovery, and cognitive rehabilitation [80, 81]. Nonetheless, evidence supporting long-term efficacy remains limited, with many studies constrained by small sample sizes, short follow-up durations, and lack of standardized intervention protocols. As a result, clinical guidelines for VR-based neurorehabilitation are still in early stages of development [82].
Simultaneously, wearable sensors and mobile health technologies provide real-time monitoring of cognitive and motor performance, allowing clinicians to tailor interventions to patient-specific needs and dynamically adjust therapeutic intensity [83, 84]. Despite their promise, issues related to data privacy, cybersecurity, patient compliance, and interoperability between digital health platforms remain unresolved and represent key barriers to large-scale implementation. The integration of neurotechnology with biomarker-guided precision medicine represents a promising interdisciplinary approach to neuroprotection. By combining molecular, imaging, and digital data streams, clinicians can develop personalized intervention strategies that target specific pathophysiological mechanisms, optimize therapeutic efficacy, with the potential to improve long-term neurological outcomes [85, 86].
This multimodal integration enables a systems-level understanding of neurological disease, where biological, structural, and behavioral data converge to support precision decision-making. However, standardization of data integration frameworks and validation across diverse populations remain essential prerequisites for clinical translation [87, 88]. Furthermore, these innovations hold particular relevance for populations with neurodevelopmental disorders, pediatric brain injuries, and early-stage neurodegenerative diseases, where timely detection and individualized intervention can significantly alter disease trajectories [89].
Early-life intervention is particularly critical, as neurodevelopmental plasticity offers a unique therapeutic window during which targeted interventions may produce long-lasting functional benefits [90]. Collectively, the convergence of AI, neuroimaging, wearable technologies, and digital therapeutics is shaping the future of precision neuroprotective care, offering unprecedented opportunities for improving functional recovery and quality of life in patients with neurological disorders [91]. Nevertheless, ethical considerations, regulatory challenges, and health system readiness must be addressed to ensure equitable and safe implementation of these technologies across both high-resource and low-resource healthcare settings.
Advancing neuroprotective strategies requires a comprehensive and bidirectional translational framework that effectively bridges mechanistic discoveries in neuroscience with clinically applicable interventions [92]. Despite rapid progress in understanding neuroinflammation, mitochondrial dysfunction, and neuroimmune signaling, a substantial gap persists between experimental findings and their successful translation into evidence-based clinical therapies. This “translational gap” remains one of the major barriers in modern neurotherapeutics [93].
Future investigations should prioritize well-designed longitudinal cohort studies to validate the reliability, reproducibility, and predictive value of emerging biomarkers across diverse ethnic, genetic, and clinical populations. Such studies are critical for establishing early diagnostic thresholds, monitoring disease progression, and guiding individualized interventions [94]. Importantly, biomarker validation must also address inter-individual variability, assay standardization, and cross-platform harmonization to ensure clinical reliability and scalability. Without these methodological refinements, the utility of biomarkers in real-world settings will remain limited [95, 96].
In parallel, randomized controlled trials are essential to evaluate the safety, efficacy, and optimal delivery methods of innovative therapeutic approaches, including experimental strategies such as mitochondrial transfer techniques, mitochondrial biogenesis-enhancing pharmacotherapies, and microbiota-targeted interventions. However, most of these interventions currently remain at preclinical or early-phase clinical stages, with limited high-quality randomized evidence. This highlights the urgent need for multicenter, adequately powered clinical trials with standardized endpoints and long-term follow-up [97, 98].
These trials will provide robust evidence to support clinical translation and inform best-practice guidelines for neuroprotective care. Policy-level initiatives are equally important to facilitate early detection and intervention, particularly in resource-limited settings where the burden of neurological disorders is disproportionately high. In such settings, late presentation, limited diagnostic infrastructure, and lack of specialized neurological services significantly contribute to poor outcomes, underscoring the need for health system strengthening and equitable access to neurodiagnostic tools [99]. Implementation of structured neurodiagnostic screening programs, combined with accessible preventive and rehabilitative services, may significantly reduce long-term disability and improve functional outcomes. Moreover, integrating neurotechnology platforms, such as AI-driven neuroimaging analysis and digital cognitive monitoring, can enhance precision medicine approaches and optimize patient-specific therapeutic strategies [100].
Nevertheless, successful implementation requires addressing key challenges including digital infrastructure disparities, workforce training, data governance, and ethical frameworks for AI deployment in clinical neurology [101, 102]. Collaboration across global research networks, including multidisciplinary teams of neuroscientists, clinicians, bioengineers, data scientists, and health policy experts, will be critical to accelerate the development, validation, and dissemination of neuroprotective interventions. Such collaborative models also enable data sharing, standardization of methodologies, and harmonization of research protocols, which are essential for improving reproducibility and accelerating clinical translation [103]. By combining mechanistic insights, technological innovation, and evidence-based clinical practice, translational research can substantially advance precision neuroprotection. Ultimately, these integrated strategies have the potential to improve neurological health outcomes, mitigate disease progression, and enhance quality of life for patients across the lifespan. However, achieving these goals will require sustained investment in neuroscience research, interdisciplinary integration, and long-term policy commitment to ensure that scientific advances are effectively translated into accessible clinical care.
Neuroinflammation-mediated neuronal injury serves as a central and unifying mechanism underlying a wide spectrum of neurological disorders, ranging from neurodevelopmental conditions to progressive neurodegenerative diseases. However, it is increasingly recognized that neuroinflammation is a context-dependent process, encompassing both adaptive and maladaptive responses, and therefore should not be interpreted as uniformly pathological across all disease stages or conditions. Targeting this fundamental pathway offers a strategic approach for early intervention and disease modification. Recent advances in biomarker discovery enable the detection of preclinical neuronal dysfunction, allowing for timely and personalized therapeutic strategies. Nevertheless, despite promising diagnostic performance, most biomarkers currently lack full clinical validation, standardized thresholds, and disease-specific specificity, limiting their immediate application in routine neurological practice.
Concurrent mitochondrial-based therapies, including mitochondrial transfer and biogenesis-enhancing interventions, provide innovative means to restore cellular bioenergetics and reduce oxidative stress. Although these approaches have demonstrated encouraging results in preclinical models, their translation into clinical practice remains constrained by limited human trials, safety uncertainties, and methodological heterogeneity. Modulation of the gut-brain axis through microbiota-targeted interventions further contributes to neuroprotection by regulating neuroimmune signaling and maintaining synaptic homeostasis. However, variability in microbiome composition, inconsistent clinical trial outcomes, and incomplete mechanistic understanding continue to limit definitive therapeutic conclusions.
Integration of neurotechnology and AI enhances diagnostic precision, enables continuous patient monitoring, and facilitates individualized rehabilitation strategies. Despite rapid technological progress, challenges related to external validation, algorithm transparency, ethical governance, and healthcare system readiness must be addressed before widespread clinical implementation can be achieved. Collectively, these multidisciplinary innovations support a translational framework that combines mechanistic understanding with clinical application. By adopting such an integrated approach, precision neuroprotective strategies have the potential to improve neurological outcomes, reduce disease burden, and transform the future of neuroscientific research and clinical practice. However, realizing this potential will require rigorous clinical validation, interdisciplinary collaboration, and sustained investment in translational neuroscience to bridge the persistent gap between experimental promise and real-world clinical impact.
AI: artificial intelligence
ATP: adenosine triphosphate
BBB: blood-brain barrier
MRI: magnetic resonance imaging
PGC-1α: peroxisome proliferator-activated receptor gamma coactivator-1 alpha
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
ROS: reactive oxygen species
TNF-α: tumor necrosis factor alpha
VR: virtual reality
Author acknowledges the use of generative artificial intelligence-based image creation software (ChatGPT and/or DALL-E, OpenAI, 2026) for developing the figures in this manuscript. All generated images were critically reviewed and validated by the author to ensure scientific accuracy and appropriateness.
MH: Conceptualization, Investigation, Validation, Supervision, Writing—original draft, Writing—review & editing. SF: Writing—original draft, Writing—review & editing. KS: Writing—original draft, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
This research received no external or internal funding or financial support.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 417
Download: 18
Times Cited: 0
Ravi Philip Rajkumar
Dhaara Shah ... Rana Zeine
Mac Dionys Rodrigues da Costa ... Tiago Lima Sampaio
