Systematic Review
Systematic Review

Affiliation:
1Department of Internal Medicine, East Carolina University, Greenville, NC 27834, USA
Email: Alih20@ecu.edu
ORCID: https://orcid.org/0000-0001-5546-9197
Affiliation:
1Department of Internal Medicine, East Carolina University, Greenville, NC 27834, USA
Affiliation:
2Department of Cutaneous Oncology, Moffitt Cancer Center, Tampa, FL 33612, USA
Affiliation:
3Department of Gastroenterology, East Carolina University, Greenville, NC 27834, USA
Affiliation:
4Department of Gastroenterology, University of New Mexico, Albuquerque, NM 87131, USA
Affiliation:
5Department of Gastroenterology, Washington University in St. Louis, St. Louis, MO 63130, USA
Explor Med. 2022;3:317–330 DOI: https://doi.org/10.37349/emed.2022.00096
Received: April 26, 2022 Accepted: May 24, 2022 Published: August 11, 2022
Academic Editor: Amedeo Lonardo, Azienda Ospedaliero-Universitaria di Modena, Italy
Aim: The etiologies, presentation, and management of downhill varices in the era of modern medicine are relatively under-explored and mostly limited to case reports or case series.
Methods: Published case reports/series of patients ≥ 18 years old with proven/probable downhill esophageal varices were searched on Ovid MEDLINE and Ovid EMBASE for all published cases up to January 2021.
Results: The mean age was 50.9 (standard deviation ± 17.6) years old for all downhill variceal cases. End-stage renal disease was the most common comorbidity (43.9%), followed by thyroid disease (12.2%), Behçet’s disease (9.8%), and pulmonary hypertension (7.3%). Dialysis catheters, central venous grafts, or additional catheters were additional risk factors (51.2%). Variceal bleeding presenting as hematemesis, melena, or both was the most common presenting symptom (80.5%).
Conclusions: Dialysis catheter-associated superior vena cava obstruction resulted in an increased risk of downhill varices. Other causes include thyroid malignancies, pulmonary hypertension, and Behçet’s disease.
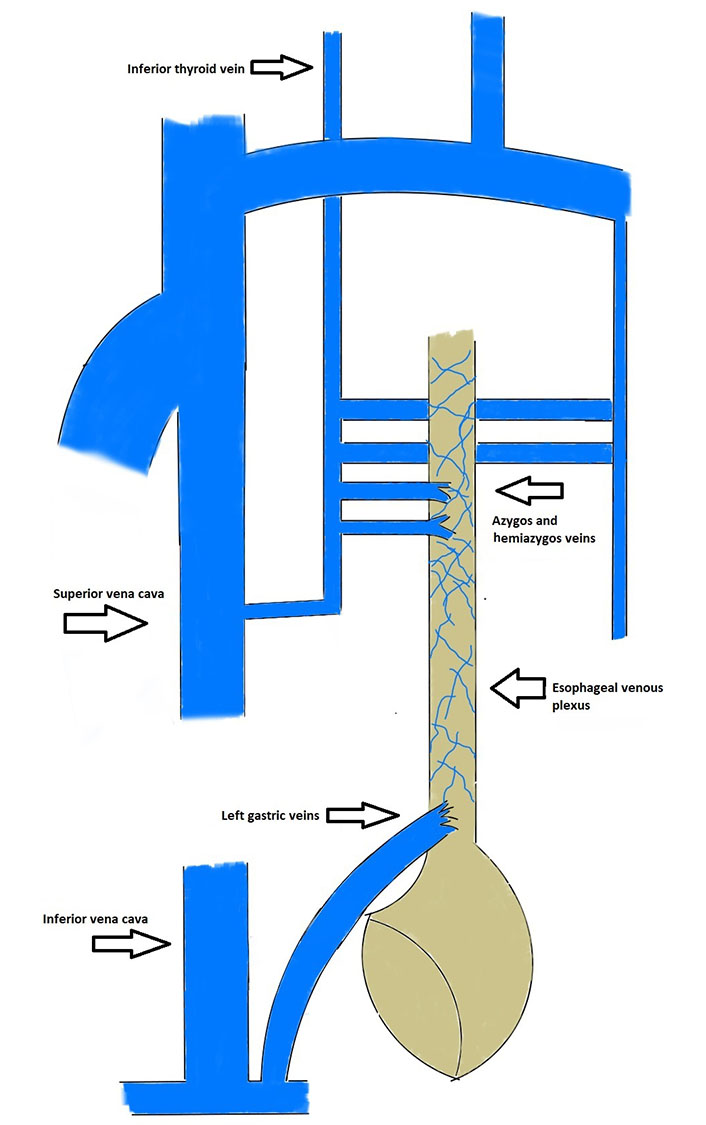
Downhill esophageal varices as an entity independent of portal hypertension were first reported in 1964 by Felson and Lessure [1]. Understanding the esophagus’ venous system is crucial to delineate between etiologies and the pathophysiology of uphill and downhill varices. The venous drainage of the cervical esophagus is via the inferior thyroid vein. In contrast, the thoracic esophagus drains via the azygos vein, the hemiazygos vein, and the bronchial veins, entering the superior vena cava (SVC). The venous drainage of the lower third of the esophagus is via the portal vein [2, 3]. An increase in portal hypertension causes the diversion of blood from the portal system to the SVC via portosystemic anastomosis resulting in “uphill” varices [4]. In contrast, downhill varices develop in the upper two thirds of the esophagus due to increased pressure or obstruction of the SVC in the cervical esophagus. This results in the blood flowing from the SVC to the azygos vein and transmits pressure to the esophageal venous plexus. Esophageal veins, which are typically not visible, can become visible due to obstructions in portal blood flow or of the SVC, leading to dilation of intramural and paraesophageal veins. They work as a collateral circulation between the portal vein, the azygos system, and the vena cava system [2, 3]. Augmented SVC pressures were thought to be the only cause for downhill varices, but recently cases have been reported due to non-obstructive SVC [5–44]. Several causes of downhill varices have been reported in literature, most common of which is SVC syndrome and associated vascular occlusion. Other causes include mediastinal fibrosis, Behçet’s syndrome, catheter manipulation, retrosternal goiter and other thyroid masses, thymomas, bronchial carcinomas, metastases, pulmonary hypertension, and lymphomas.
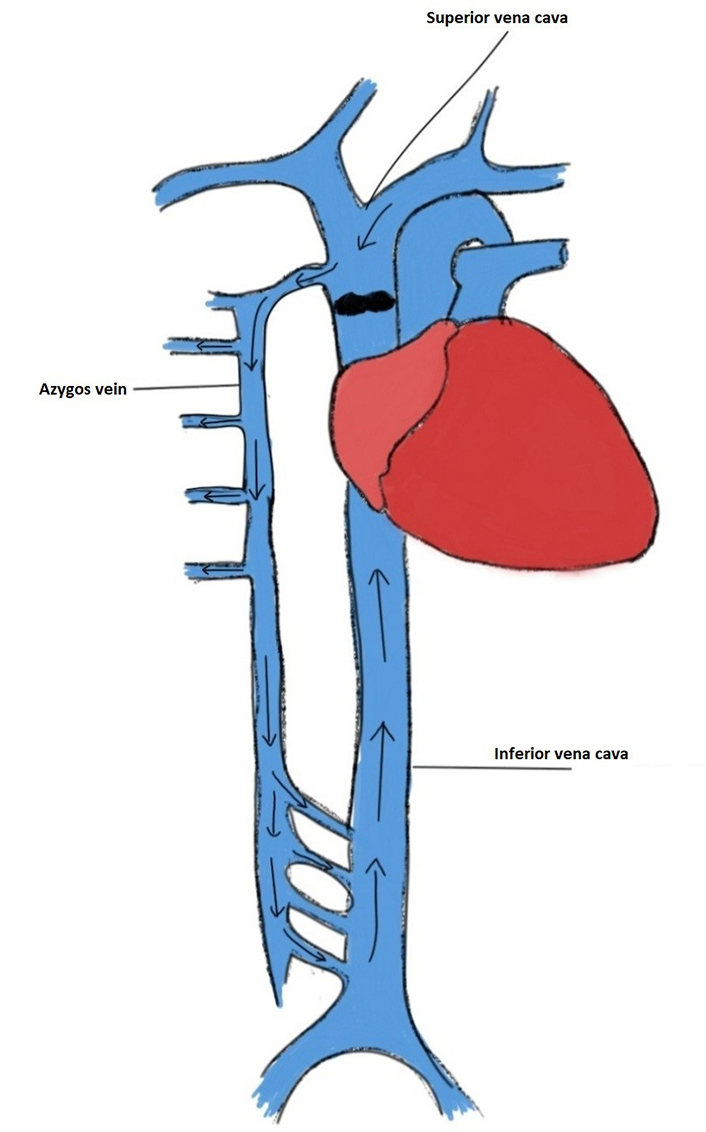
Downhill varices are diagnosed with upper endoscopy and magnetic resonance imaging (MRI) or computed tomography (CT) which are used to visualize underlying etiology [45]. Therapeutic means are directed towards controlling the bleeding via sclerotherapy or banding [22]. Etiology-specific therapies that relieve the pressure in the venous system are employed for definitive treatment. These may include thyroidectomy, balloon angioplasty, vascular stenting, or conservative management [9, 21, 28]. A brief of the esophageal venous system is provided in Figure 1. Previously, augmented SVC pressures were thought to be the only cause for downhill varices (Figure 2).
No previous systematic review or meta-analysis exists per our literature search of the epidemiology, diagnosis, treatment, and outcomes of downhill esophageal varices. Therefore, a systematic review of cases of downhill esophageal varices published from January 1970 to January 2021 was conducted, to explore the contemporary etiologies, clinical manifestations, presenting symptoms, diagnosis, and therapeutic regimens of this phenomenon.
This review was initiated and summarized per the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines [46]. The PRISMA checklist can be seen in the supplementary materials. Published case reports and series of downhill varices, as defined by the International Classification of Diseases-Tenth Revision-Clinical Modification (ICD-10-CM) code I85.00 for esophageal varices in patients ≥ 18 years old were reviewed from January 1970 to January 2021. A systematic search using search strategies that comprised of keywords including “downhill varices”, “SVC syndrome”, “goiter”, and “Behçet’s disease” was carried out in Ovid MEDLINE/PubMed and Ovid EMBASE. The search was limited to studies involving human participants and published in English. The final search was performed on January 2021. Bibliographies of relevant articles were also searched. Inclusion criteria required that the published cases had documentation of (i) presenting symptoms, (ii) predisposing factors or underlying medical conditions, (iii) endoscopic results, and (iv) management. Letters to the editors were included if they met the inclusion criteria. Any editorials, cases with inadequate details, review articles, or case series where the analysis was pooled without the description of individual patient data were excluded.
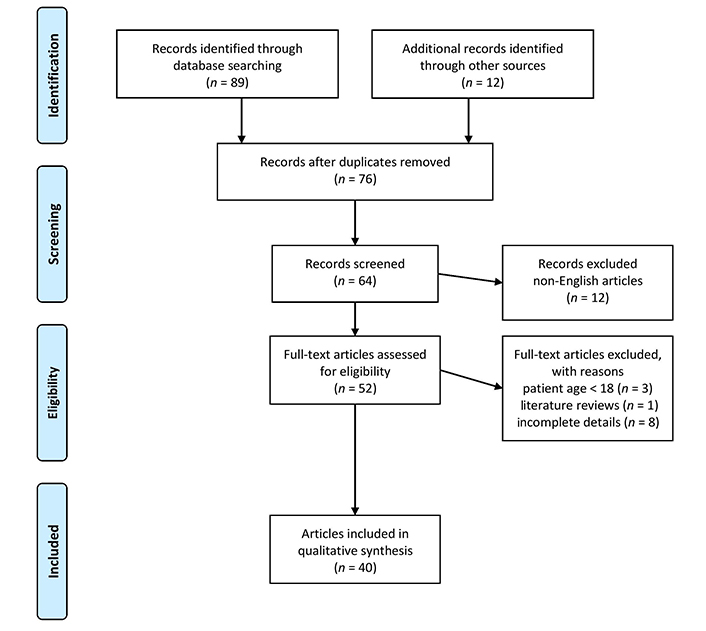
One author implemented search strategies and initial search results revealed 89 texts which were then filtered based on relevance to keywords after reviewing abstracts and titles only. Duplicates were removed and the remaining titles and abstracts were assessed for inclusion. Full texts of relevant articles were retrieved and independently assessed by two authors. Out of 64 articles selected, 12 were excluded due to non-English, and the remaining 52 articles were assessed by full-text review, among which 12 articles were additionally removed as they did not fulfill the inclusion criteria. Forty articles were selected in the final review (Figure 3) (Table 1). Any disagreements over study inclusion were resolved by consensus.
Demographics, presentation, causes and management of patients with downhill varices
| Authors | Age | Sex | Variceal bleeding | Comorbidities | Endoscopic findings | Cause | Management | Follow-up |
|---|---|---|---|---|---|---|---|---|
| Gebreselassie A et al. [5] | 55 | F | Yes | ESRD on HD Hypothyroidism | Moderate sized mid-esophageal varices | SVC syndrome secondary to central venous dialysis catheters | Conservative management | Stable on follow-up with pending vascular appointment |
| Yaşar B & Kılıçoğlu G [6] | 31 | M | Yes | Behçet’s disease | Prominent esophageal varices in the upper half of the esophagus with an overlying clot | SVC syndrome secondary to Behçet’s disease | Conservative management DMARDs Steroids | Follow-up data N/A |
| Gholam S et al. [7] | 87 | F | No | Cameron ulcers Aortic stenosis Pulmonary hypertension | Large varices in the upper third of the esophagus and Cameron lesions | Severe pulmonary hypertension secondary to aortic stenosis | Conservative management | Follow-up data N/A |
| Berkowitz JC et al. [8] | 32 | F | Yes | ESRD MCTD | Esophageal varices in the upper and middle esophagus | SVC syndrome secondary to central venous dialysis catheters | Endoscopic band ligation of a proximal varix | One year follow-up with non-bleeding grade I varices |
| Loudin M et al. [9] | 22 | F | Yes | ESRD Henoch-Schönlein purpura | Large varices in the proximal esophagus with positive red wale sign | SVC syndrome secondary to central venous dialysis catheters | Balloon dilation of the stenotic SVC | One year follow-up without recurrent bleeding |
| Yasar B & Abut E [10] | 45 | M | Yes | Seminoma Pelvic radiotherapy | Varices in the upper third of the esophagus | Bilateral brachiocephalic truncus stenosis due to mediastinal fibrosis | Conservative management | Stable hemoglobin at follow-up visits |
| Gessel L & Alcorn J [11] | 39 | M | Yes | ESRD Cerebral palsy | Mid and upper esophageal varices | Stenosis of the SVC secondary to scoliosis and central venous dialysis catheters | Conservative management | Follow-up data N/A |
| Inoue Y et al. [12] | 66 | M | No | Thymoma SVC and BCV resection | Mid and upper esophageal varices | Postoperative SVC graft occlusion | Conservative management | Stable at 3, 6, 18 months follow-ups |
| Pillai U et al. [13] | 73 | M | Yes | ESRD Hypertension CAD PAD Diastolic heart failure | Extensive mid esophageal varices | SVC stenosis from HeRO graft placement | Endoscopic band ligation | No recurrent bleeding at follow-ups |
| Basar N et al. [14] | 54 | M | No | AV block Epicardiac pacemaker | Upper esophageal varices | Bilateral subclavian veins DVTs secondary to pacemaker | Patient refused treatment | Patient demise at 4 months due to hospitalization refusal |
| Lim EJ et al. [15] | 68 | M | Yes | Small and large bowel resection Short gut syndrome Total parenteral nutrition via right subclavian vein Hickman’s catheter | Upper esophageal varices | SVC syndrome secondary to bilateral brachiocephalic vein stenosis | Endoscopic variceal band ligation Hickman’s catheter removal | Follow-up data N/A |
| Mönkemüller K et al. [16] | 82 | M | No | Diabetes mellitus type II Hyperlipidemia Parkinson’s disease Retrosternal goiter | Upper esophageal downhill varices | Obstruction of the thyroid veins secondary to retrosternal goiter | Conservative management (patient preferred) | Follow-up data N/A |
| Vorlop E et al. [17] | 42 | F | Yes | Multiple myeloma Antiphospholipid syndrome | Upper esophageal downhill varices | SVC occlusion secondary to a central venous port | Angioplasty and stenting of the SVC Removal of the indwelling catheter | Normal endoscopy at 4 weeks follow-up |
| Froilán C et al. [18] | 49 | M | Yes | Hypertension Diabetes mellitus ESRD | Mid to upper esophageal varices | Stenosis of the SVC secondary to central venous dialysis catheters | Proximal sclerotherapy Angiographic metal stenting | Follow-up data N/A |
| Calderwood AH & Mishkin DS [19] | 55 | F | Yes | ESRD Ischemic cardiomyopathy Left upper-extremity deep vein thrombosis | Proximal esophagus varices | Stenosis of the SVC secondary to central venous dialysis catheters | Endoscopic variceal ligation with band placement Angiographic balloon dilation and stent placement | Symptom resolution at 3 months follow-up |
| Greenwell MW et al. [20] | 55 | F | Yes | ESRD Hypertension | Mid to upper esophageal varices | SVC stenosis/stricture secondary to previous venous catheterizations | Esophageal band ligation Angioplasty with stenting of the SVC stricture | No recurrent GI bleeding at follow-ups |
| Ibis M et al. [21] | 35 | F | Yes | History of subtotal thyroidectomy and multinodular goiter | Upper esophageal varices | Downhill varices secondary to recurrent multinodular goiter | Esophageal band ligation Inferior thyroid artery embolization Repeat subtotal thyroidectomy | Follow-up data N/A |
| Tavakkoli H et al. [22] | 42 | M | Yes | Behçet’s disease | Upper esophageal varices | SVC obstruction secondary to Behçet’s disease | Esophageal band ligation | Variceal eradication at 1 and 6 months interval on follow up |
| van der Veldt AA et al. [23] | 77 | F | Yes | COPD Multinodular goiter | Grade II–III upper esophageal varices | Right internal jugular vein compression secondary to multinodular goiter | Subtotal thyroidectomy | Stable at 20 months follow-up |
| Areia M et al. [24] | 89 | M | Yes | Diabetes mellitus Pulmonary embolism on warfarin Severe pulmonary hypertension | Grade II upper esophageal varices | Pulmonary hypertension and oral anticoagulant use | Conservative management | Stable at 3 months follow-up |
| Bédard EL et al. [25] | 68 | F | Yes | Retrosternal goiter | Upper esophageal varices | Extrinsic compression of the right innominate vein secondary to retrosternal goiter | Thyroidectomy | Follow-up data N/A |
| Serin E et al. [26] | 60 | F | No | None | Upper esophageal varices | Increase blood drainage from the tumor into the esophageal veins | Tumor removal | Resolution of varices at 15 months follow-up |
| Blam ME et al. [27] | 42 | F | No | Pulmonary sarcoidosis Uveitis ESRD | Grade II varices in the mid to distal esophagus | SVC syndrome secondary to central venous dialysis catheters | Conservative management | Follow-up data N/A |
| Chakinala RC et al. [28] Case 1 | 56 | M | Yes | ESRD Rheumatoid arthritis PAD Esophageal varices | Upper and middle esophageal varices | Chronic SVC and right brachiocephalic vein occlusion secondary to venous catheters | Esophageal band ligation Failed SVC stenting | Follow-up data N/A |
| Chakinala RC et al. [28] Case 2 | 56 | M | Yes | Gastroparesis Diabetes mellitus type II ESRD on HD Atrial flutter on warfarin | Upper and middle esophageal varices | Chronic SVC and right brachiocephalic vein occlusion secondary to venous catheters | Conservative management | Follow-up data N/A |
| Hussein FA et al. [29] | 43 | F | Yes | ESRD on HD Hypertension PAD | Upper esophageal varices | SVC stenosis/occlusion secondary to SVC catheter later replaced by graft | Variceal banding Refused SVC angioplasty | Resolution of varices at follow-ups |
| Chandra A et al. [30] | 55 | M | Yes | Diabetes mellitus type II ESRD on HD | Middle and upper esophageal varices | SVC syndrome secondary to thrombosis from HD catheter | Balloon angioplasty with stenting | Follow-up data N/A |
| Pratap et al. [31] | 26 | M | Yes | ESRD on HD | Upper third esophageal varices | Left brachiocephalic vein and SVC obstruction secondary to HD catheter | Venous angioplasty with balloon dilation | No GI bleeding at 7 months follow-up |
| Ennaifer R et al. [32] | 31 | M | Yes | Behçet’s disease | Upper esophageal varices | SVC syndrome secondary to Behçet’s disease | Conservative management DMARDs Steroids | Follow-up data N/A |
| Muthyala U et al. [33] | 31 | F | Yes | Interstitial nephritis ESRD | Proximal esophageal varices | SVC stenosis/obstruction due to multiple central venous accesses | Angioplasty | No GI bleeding at 9 months follow-up |
| Harwani YP et al. [34] | 55 | F | yes | Liver cirrhosis Chronic rheumatic heart disease, severe mitral and tricuspid regurgitation Pulmonary hypertension | Upper and lower esophageal varices | Dilated SVC due to pulmonary hypertension | Variceal banding | Follow-up data N/A |
| Rhoades DP et al. [35] | 57 | M | Yes | Hepatitis C cirrhosis Human immunodeficiency virus infection Hemophilia A | Upper esophageal varices | Idiopathic | Variceal banding | Stable hemoglobin at 1, 3 months follow-ups |
| Nguyen LP et al. [36] | 39 | F | Yes | Diabetes Hypertension ESRD on HD Recurrent AV fistula thrombosis | Large esophageal varices 25 cm to the distal esophagus just above the gastroesophageal junction | SVC thrombosis secondary to catheter | Angioplasty with stenting | Subsequent EGD showed variceal resolution |
| Nayudu SK et al. [37] | 48 | M | Yes | ESRD on HD Seizure disorder Dyslipidemia Hypertension | Upper esophageal varices | SVC occlusion secondary to dialysis catheter | Angioplasty | Stable hemoglobin at follow-ups |
| Shirakusa T et al. [38] | 26 | M | No | Hepatitis | Upper esophageal varices | Excessive blood flow into the esophageal wall from a giant lymphoma | Thoracotomy | Follow-up data N/A |
| Pop A et al. [39] | 52 | F | Yes | Hypertension, diabetes mellitus type II, PAD ESRD | Proximal to mid-esophageal varices | SVC thrombosis secondary to thrombosis from HD catheter | Failed balloon angioplasty Gore-Tex graft bypass with an end-to-side anastomosis | No recurrent GI bleeding at 5 months follow-up |
| Sorokin JJ et al. [40] | 46 | F | No | Subtotal thyroidectomy | Upper esophagus and gastroesophageal junction varices | SVC obstruction secondary to mediastinum fibrosis | Conservative management | Follow-up data N/A |
| Johnson LS et al. [41] | 85 | F | Yes | None | Upper esophageal varices | SVC obstruction due to retrosternal thyroid | Total thyroidectomy | Resolution of varices at 2 and 24 months follow-ups |
| Orikasa H et al. [42] | 59 | M | No | Behçet’s disease | Four upper esophageal varices | SVC syndrome secondary to Behçet’s disease | Conservative management | Follow-up data N/A |
| Maton PN et al. [43] | 34 | F | Yes | Idiopathic vasculitis | Upper esophageal varices | Vasculitis | Conservative management | Hemoglobin improvement over next 18 months |
| Basaranoglu M et al. [44] | 34 | F | Yes | Asthma | Grade II upper esophageal varices | SVC obstruction secondary to fibrosing mediastinitis | Conservative management | Persistent grade II varices on follow-up imaging |
M: male; F: female; ESRD: end-stage renal disease; HD: hemodialysis; N/A: not available; DMARDs: disease-modifying antirheumatic drugs; DVT: deep venous thrombosis; MCTD: mixed connective tissue disease; BCV: brachiocephalic vein; AV: atrioventricular; GI: gastrointestinal; COPD: chronic obstructive pulmonary disease; PAD: peripheral arterial disease; EGD: esogastroduodenoscopy; CAD: coronary artery disease; HeRO: HD reliable outflow
Using standardized data extraction forms, data were extracted independently by the two authors and compared. Discrepancies were discussed with the third author as adjudicator. Data extracted included patient demographics, underlying conditions/comorbidities, presenting symptoms, diagnosis or endoscopic findings, predisposing etiologies, probable causes, and interventions during the hospitalization for downhill varices. The authors reviewed each case report to deduce whether other causes of variceal bleeding in each case were sufficiently excluded. Potentially overlapping causes, for example, patients with goiter and ESRD/dialysis catheter placement, both, etc. were also looked at and no such cases were reported or included in present study.
Underlying conditions that may predispose to downhill variceal bleeding were extracted and include the following: central venous catheter placements, grafts, ESRD, vasculitis, tumors, and goiter. All reported cases were also screened for duplication to ensure unique cases. Recently, Murad et al. [47] proposed a tool to evaluate the methodological quality of case reports and case series in systematic reviews. They proposed explanatory questions to assess ascertainment, casualty, and reporting. This is quite similar to our search strategy, and therefore, a separate risk of bias evaluation was not conducted. Additionally, as the data were derived from case reports, the data of interest were not subject to bias.
Data analysis was conducted using STATA statistical software. Patient demographics, predisposing factors, endoscopic findings, and therapeutic regimens were summarized descriptively. Illustrations were generated electronically.
Out of the 41 patients, the mean age was 50.9 [standard deviation (SD) ± 17.6]. The mean age for males was 53 (n = 19, SD ± 17.8) and for females 49.05 (n = 22, SD ± 17.6). ESRD was the most common comorbidity 18/41 (43.9%) followed by retrosternal goiter or thyroid malignancies 5/41 (12.2%), Behçet’s disease 4/41 (9.8%), and pulmonary hypertension 3/41 (7.3%). Other causes were 26.8% (n = 11) (Table 2). Dialysis catheters, central venous grafts, or additional catheters were additional risk factors 21/41 (51.2%). SVC syndrome (SVC) was a direct cause of downhill varices in 29/41 cases (68.3%) either due to dialysis catheters or other comorbidities. 100% of patients with underlying ESRD had either a dialysis catheter or bypass graft as a predisposing factor compared to only 13% of non-ESRD patients who had underlying catheters as the possible etiology (3/23).
Comorbidities or predisposing factors in downhill varices
| Variables | n | |
|---|---|---|
| ESRD | 18 | |
| Retrosternal goiter or thyroid malignancies | 5 | |
| Behçet’s disease | 4 | |
| Pulmonary hypertension | 3 | |
| Miscellaneous conditions/comorbidities | Castleman disease | 1 |
| Mediastinal fibrosis | 3 | |
| Total parenteral nutrition catheter | 1 | |
| Idiopathic | 1 | |
| Thymoma | 1 | |
| Upper extremity deep venous thrombosis | 1 | |
| Forgotten port | 1 | |
| Lymphoma | 1 | |
| Vasculitis | 1 | |
In the present study, hematemesis and melena were the most common presenting symptoms 33/41 (80.5%). Other presenting symptoms included symptomatic anemia, dysphagia, abdominal pain, hematochezia, and symptoms of SVC obstruction 8/41 (19.5%). Variceal bleeding was the most common presentation in ESRD patients 17/18 (94.4%) followed by retrosternal thyroids and Behçet’s disease patients respectively (80% and 75%). Variceal bleeding in patients with a catheter 12/21 (90.5%) or SVC obstruction 24/29 (82.8%) was calculated separately. When calculated separately, variceal bleeding on presentation was most common in patients with ESRD 17/18 (94.4%) versus non-ESRD patients 16/23 (69.6%).
The majority of cases underwent management based on the etiology. Patients not undergoing any invasive interventions other than medications were defined as conservative therapy. Among all cases, there were twelve angioplasties with or without stent placement, eleven esophageal bandings for variceal bleeding, one sclerotherapy and four thyroidectomies. Fourteen patients underwent conservative management. While a total of 21 cases had SVC obstruction as reported earlier, all patients who underwent angioplasty had underlying SVC obstruction secondary to dialysis catheters 12/21 (57.14%). About 3/21 (14.9%) cases of variceal bleeding underwent banding and angioplasties, 3/21 (14.9%) cases of variceal bleeding underwent banding only, 1/21 (4.8%) underwent sclerotherapy with angioplasty, and 4/21 (19%) of the patients were managed conservatively. In the present study, 9/21(42.8%) cases had angioplasties only. Three fifth (60%) patients with underlying etiology of retrosternal thyroid underwent thyroidectomies and only 1/5 (20%) underwent conservative treatment. Concurrently, only 1/5 (20%) patient underwent variceal banding and thyroidectomy. All four cases of Behçet’s disease underwent conservative management with steroids and tumor necrosis factor (TNF) inhibitors. One patient also underwent variceal banding. Pulmonary hypertension was managed conservatively except for one case for which esophageal variceal banding was performed.
This is a contemporary systematic review of downhill esophageal varices providing an insight into presenting symptoms and an increasing spectrum of etiologies of downhill varices. The current review was undertaken and reported using the PRISMA guidelines. Downhill varices bleeding has been reported to bleed less than uphill varices. This could be explained by the fact that variceal bleeding secondary to portal hypertension is associated with coagulopathy in decompensated stages of cirrhosis and due to the squamous lining of the distal esophagus having an increased gastric acid reflux exposure. Additionally, the veins in the distal part of the esophagus run in the mucosal layer whereas those in the upper esophagus are deeper and run in the submucosa [9].
There was an increased incidence of downhill esophageal varices in ESRD patients. This could be secondary to patients having underlying SVC obstruction besides dialysis catheters (Table 1). Variceal bleeding presenting as hematemesis or melena was the most common presenting symptom in downhill varices. Possible mechanisms by which the catheters contribute to the development of SVC obstruction include endothelial damage during insertion, blood turbulence due to a catheter, decreased limb movement, and other overlapping comorbidities [48]. Anticoagulant prophylaxis may be used to reduce the risk of symptomatic and asymptomatic catheter-associated thrombosis and obstruction [48]. Previous prophylactic treatments that have been studied include heparin infusions, vitamin K antagonists and low molecular weight heparin. A recent meta-analysis comparing prophylactic modalities did not include patients with ESRD or dialysis catheters and the implications of prophylactic anticoagulation in patients with ESRD is not widely studied [49, 50]. However, a systematic review of individuals with atrial fibrillation receiving dialysis found similar efficacy in preventing venous thromboembolic events with direct oral anticoagulants (DOACs) versus warfarin [51]. Some of the other predisposing factors that are found less happened included retrosternal thyroids [16, 21, 23, 40, 41], Behçet’s disease [6, 22, 32, 42] and pulmonary hypertension [7, 24, 25, 34].
Downhill varices in retrosternal goiter develop due to a similar obstruction in the thyroid veins resulting in the blood re-routing via the deep esophageal veins [16]. In the absence of any obstruction, blood from the thyroid plexus passes within the inferior thyroid veins into the brachiocephalic vein [23]. Imaging reveals that there could be obstruction of blood flow to the thyroid veins due to excessive pressure of retrosternal thyroid growth and improvement in varices after thyroidectomy [16, 21, 23, 40]. The definitive diagnosis is made via neck imaging and management mainly involves thyroidectomy to relieve the obstruction and resume normal blood flow. In addition, a mechanical obstructive mechanism increased blood drainage in the esophageal veins due to malignancy as well as pulmonary hypertension leading to venous backflow have also been proposed as etiologies for downhill varices [26, 34, 38].
The establishment of a diagnosis almost always includes an endoscopic evaluation which may or may not include endoscopic management. However, a diagnostic workup is required to identify the etiology. Patients can undergo imaging studies including x-rays, barium swallows, CT angiograms, and/or MRIs. While esophageal banding or sclerotherapy can be temporizing for acute variceal bleeding definitive treatment, which alleviates the underlying SVC obstruction. Based on the etiology, some of the management strategies were catheter removal, angioplasty with or without stenting, thyroidectomy, tumor resection, or conservative therapy. Conservative therapy involves DMARDs or steroids is most used in Behçet’s disease or vasculitis [6, 7, 20, 22, 24, 25, 32, 34, 42]. The impact of dialysis catheters on the incidence of downhill varices is a preventable cause and further comparative data are required to avert unwanted complications.
The current review provides the most recent and most extensive overview of the predisposing factors, diagnoses, and causes of downhill varices. Cases covered in this systematic review were identified from a thorough search of databases using a well-organized search strategy. Despite having stringent inclusion criteria, authors cannot rule out the possibility of missing cases given that some individual patient data were unavailable. Publication bias is a limiting factor in the present study as case reports often represent rare observations that are more likely to be published which potentially excludes some of the more common cases.
Although rare, downhill esophageal varices are an established cause of upper gastrointestinal hemorrhage. This review revealed that ESRD patients might be at an increased risk of downhill variceal bleeding compared to other etiologies. Dialysis catheter-associated SVC obstruction remains the most known cause in ESRD patients. It would be helpful for prospective future trials to study novel precautionary measures to avoid SVC obstruction in ESRD patients. No data are currently available regarding the use of anticoagulation to prevent SVC thrombosis and downhill varices in ESRD patients.
DMARDs: disease-modifying antirheumatic drugs
ESRD: end-stage renal disease
PRISMA: preferred reporting items for systematic reviews and meta-analyses
SD: standard deviation
SVC: superior vena cava
The supplementary material for this article is available at: https://www.explorationpub.com/uploads/Article/file/100196_sup_1.pdf.
HA, RP and EA contributed conception and design of the study; HA organized the database; HA and RP performed the statistical analysis; HA wrote the first draft of the manuscript; HA, RP, EA, SP and DK wrote sections of the manuscript. NLB edited the manuscript. All authors contributed to manuscript revision, read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
The datasets analyzed for this study can be found at Ali, Hassam (2021), “Downhill varices extracted variables from case reports”, Mendeley Data, V2, doi: 10.17632/t3mhc497c2.2.
Not applicable.
© The Author(s) 2022.
Copyright: © The Author(s) 2022. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.