Original Article
Original Article

Affiliation:
1Department of Oncology, Hematology, Cancer Prevention Research Center, Isfahan University of Medical Sciences, Isfahan 8158177356, Iran
†These authors contributed equally to this work.
ORCID: https://orcid.org/0000-0003-4867-5683
Affiliation:
1Department of Oncology, Hematology, Cancer Prevention Research Center, Isfahan University of Medical Sciences, Isfahan 8158177356, Iran
†These authors contributed equally to this work.
ORCID: https://orcid.org/0000-0002-9874-298X
Affiliation:
2Cancer Prevention Research Center, Isfahan University of Medical Sciences, Isfahan 8158177356, Iran
ORCID: https://orcid.org/0000-0001-6002-1864
Affiliation:
3Division of General Internal Medicine, Department of Medicine, Toronto General Hospital, Toronto, ON M2G 2C4, Canada
ORCID: https://orcid.org/0000-0003-4901-676X
Affiliation:
3Division of General Internal Medicine, Department of Medicine, Toronto General Hospital, Toronto, ON M2G 2C4, Canada
ORCID: https://orcid.org/0000-0003-4177-4806
Affiliation:
3Division of General Internal Medicine, Department of Medicine, Toronto General Hospital, Toronto, ON M2G 2C4, Canada
ORCID: https://orcid.org/0000-0001-5022-9979
Affiliation:
3Division of General Internal Medicine, Department of Medicine, Toronto General Hospital, Toronto, ON M2G 2C4, Canada
ORCID: https://orcid.org/0000-0003-4663-0537
Affiliation:
1Department of Oncology, Hematology, Cancer Prevention Research Center, Isfahan University of Medical Sciences, Isfahan 8158177356, Iran
Email: drhosseini.forough@gmail.com
ORCID: https://orcid.org/0000-0002-1061-9478
Explor Med. 2023;4:314–322 DOI: https://doi.org/10.37349/emed.2023.00142
Received: October 05, 2022 Accepted: December 18, 2022 Published: May 30, 2023
Academic Editor: Amedeo Lonardo, Azienda Ospedaliero-Universitaria di Modena, Italy
Aim: There is a correlation between the number of resected lymph nodes (LNs) and survival as well as staging in patients with colorectal cancer (CRC). This cohort discussed the effect of the number of dissected LNs on the prognosis [survival, disease-free survival (DFS)] of patients with stage II and III CRC.
Methods: In this historical prospective cohort study, the records of 946 patients with CRC operated in the Seyyed-Al-Shohada hospital in Isfahan from 1998 to 2014 were enrolled. Then the impact of LNs on the overall survival (OS) and DFS were analyzed.
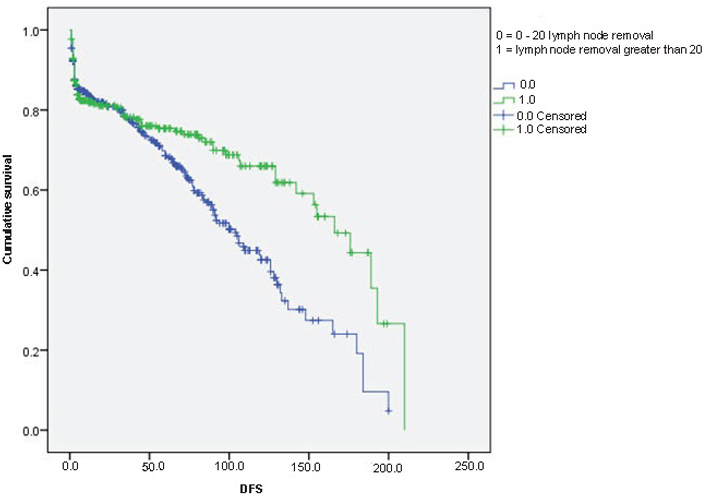
Results: The number of removed LNs was higher among males [mean difference = 1.38, t (944) = 2.232, P-value = 0.02]. The median of the DFS for the patients with 1 to 20 LN removal was 104 months [95% confidence interval (CI): 90.97–117.03], while this number for the patients with more than 20 nodes was 166 months (95% CI: 140.41–191.58). DFS between two groups of CRCs, LN removal 1–20, and greater than 20. Age and number of LN removal were significant predictors of the DFS. There was a strong and statistically significant correlation between DFS and OS among CRC patients.
Conclusions: This study shows that if the number of resected LNs in patients with CRC is more than 20, it will increase in DFS and OS.
Colorectal cancer (CRC) was the fourth most common cancer in 2020 and is currently the second leading cause of cancer-related deaths in the United States [1]. Despite the advances in perioperative radiotherapy and adjuvant chemotherapy, operative intervention plus lymph node (LN) dissection play an important role in the management of CRC [2].
The eighth edition of the American Joint Committee on Cancer staging system (AJCC, AJCC-8th) has defined tumor-node-metastasis (TNM) staging model and cancer stage for optimal treatment guidance based on different classifications [3]. The number of positive dissected LNs is emphasized by AJCC-8th TNM staging system due to their predictive power for overall survival (OS) and disease-free survival (DFS) [4].
American College of Pathologists (ACP) and AJCC recommended the assessment of 12 LNs or more to ensure accurate nodal staging in CRC patients, while some researchers reported that the least number of LN examined was 15 to identify LN metastasis and improve median OS [5–7]. From the surgical perspective, a minimum of 12 LNs was adopted as a quality measure for surgical practice [8]. However, some studies have found no association between increasing LN counts and DFS or OS [8, 9].
Some researchers reported that extensive LN dissection can achieve accurate staging and prolong survival, whereas, others emphasize the considerable risk of understanding, which might negatively impact the efficacy of chemotherapy and patient outcomes [7–10]. There is no consensus on the minimum number of LNs to be resected or examined for accurate staging of CRC and the survival benefit of patients [11]. The aim of this study is to assess the impact of the number of LNs examined on the OS and DFS of patients who underwent surgery for stage II and III CRC.
In this single institute, historical cohort the records of patients with confirmed CRC referring to Seyyed-Al-Shohada hospital in Isfahan from 1998 to 2014 were recruited. The demographic data such as sex, age, weight, and height were extracted from the patient’s files, and the body mass index (BMI) was calculated by dividing weight in kilogram (kg) by the square of height in meters (m2). Moreover, the tumor’s information, including the stage at diagnosis, depth, location and the histopathology of the tumor, grading, lymph vascular invasion, number of extracted LNs and DFS time were obtained. The tumors were staged based on the AJCC staging system, 6th edition, and National Comprehensive Cancer Network guidelines [12, 13]. The ACP and AJCC recommend a four-tiered grading system based on the degree of gland formation. The depth is defined as the local tumor extent which refers to T in the TNM staging system of AJCC-8th, the preferred staging system for CRC [4]. The time between diagnoses of the disease to the dead time or the last evaluation date was considered OS. The study respected the Declaration of Helsinki, and the patients’ information remained secret. The study was approved by the Isfahan University of Medical Sciences Review Board (No. IR.MUI.REC.1395.2.228).
Descriptive statics such as mean and standard deviation (SD) were used for normally distributed data and categorical data were presented as frequency and percentage. Logistic regression analysis was used to calculate the association between several factors such as age, sex, number of removed LNs, and the involvement of the LNs as the dependent variable. The odds ratio (OR) was estimated as the measure of association. Univariate associations were determined for the initial selection of potential variables to be included in the multivariable logistic regression models, and variables with a significance level of P < 0.20 were considered for further analysis.
A Cox regression analysis was performed using the hazard ratio (HR) as a measure of association to study the relationship between different factors and the relapse of the tumor. The time for diagnosis until the relapse of the disease was considered a follow-up time or DFS. The HR in survival analysis approximates the relative risk, expressing the likelihood that a particular risk factor predicts the recurrence of disease relative to the likelihood of recurrence in the absence of this risk factor. The survival curve was drawn for two groups of patients who underwent LN removal. The number of removed LNs as 1 to 20 and greater than 20 was categorized. All data analyses were done using the statistical package for social studies version 22.0 (SPSS Inc, Chicago, Ill), considering the significance level as 0.05.
The characteristics of the 946 patients with CRCs categorized based on the disease stage are noted in Table 1. The mean age of the patients with CRC was 58.5 ± 10.7, with 45.5% were females. There were no statistically significant differences among patients in stages two and three of CRC regarding age, sex, height, number of removed LNs, and cancer grading.
Characteristics of patients based on the stage
| Variable | Total (n = 946) | Stage II (n = 640) | Stage III (n = 306) | P-value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Age (mean ± SD) | 58.5 ± 10.71 | 58.07 ± 10.86 | 59.28 ± 10.35 | 0.102 | |||||
| Female (n, %) | 429 (45.3%) | 282 (44.1%) | 147 (48%) | 0.264 | |||||
| Height (cm, mean ± SD) | 166.3 ± 10.46 | 166.33 ± 10.62 | 166.24 ± 10.15 | 0.90 | |||||
| Removed LNs (mean ± SD) | 15.88 ± 9.49 | 16.06 ± 9.69 | 15.49 ± 9.06 | 0.381 | |||||
| Involved LNs (mean ± SD) | 0.89 ± 2.91 | 1 ± 2.84 | 1 ± 3.04 | 0.10 | |||||
| Grading (n, %) | |||||||||
| 1 | 160 (16.9) | 105 (16.4) | 55 (18.0) | 0.413 | |||||
| 2 | 316 (33.4) | 205 (32.0) | 11 (36.3) | ||||||
| 3 | 282 (29.8) | 197 (30.8) | 85 (27.8) | ||||||
| 4 | 188 (19.9) | 133 (20.8) | 55 (18.0) | ||||||
The results of the univariate logistic regression showed in Table 2. Age, number of removed LNs, and OS were associated with the LNs’ involvement. With an increase in the number of removed LNs, the OR for the involvement decreases [OR = 0.861, 95% confidence interval (CI): 0.84–0.88]. In the final model, age, number of removed LNs, and OS remained significant.
Univariate and multivariable associations between specific demographic and tumor-specific characteristics and LN involvement in CRC
| Variable | Univariate | Multivariable | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | ||||||
| Age | 0.983 | 0.969–0.998 | 0.973 | 0.955–0.992 | |||||
| Female | 1.228 | 0.891–1.694 | - | - | |||||
| Removed LNs | 0.862 | 0.841–0.885 | 0.861 | 0.836–0.883 | |||||
| OS | 0.999 | 0.996–1.003 | 0.996 | 0.991–1.000 | |||||
| DFS | 0.999 | 0.995–1.003 | - | - | |||||
| Colon | 1.282 | 0.918–1.792 | - | - | |||||
| Grading | |||||||||
| 1 | Reference | - | - | - | |||||
| 2 | 0.909 | 0.574–1.440 | - | - | |||||
| 3 | 0.816 | 0.507–1.312 | - | - | |||||
| 4 | 0.654 | 0.382–1.121 | - | - | |||||
-: these variables were not entered in the final model; Reference: reference group
There was a statistically significant difference between males and females regarding the number of removed LNs. The number of removed LNs was higher among males (mean difference = 1.38, t (944) = 2.232, P-value = 0.02).
The median of the DFS for the patients with 1 to 20 LN removal was 104 months (95% CI: 90.97–117.03), while this number for the patients with more than 20 nodes was 166 months (95% CI: 140.41–191.58). The Kaplan-Meier survival function for the DFS among two groups of CRC, LN removal 1–20, and greater than 20 are shown in Figure 1. The stepwise Cox multivariate regression test showed age and the number of LN removal were significant predictors of the DFS (Table 3). There was a strong and statistically significant correlation between DFS and OS among colorectal patients (r = 0.97, P-value < 0.0001).
Univariate and multivariable stepwise Cox regression models of DFS
| Variable | Univariate | Multivariable | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | HR | 95% CI | ||||||
| Age | 1.06 | 1.05–1.07 | 1.06 | 1.05–1.07 | |||||
| Female | 1.15 | 0.91–1.46 | - | - | |||||
| LNs removed > 20 | 0.68 | 0.53–0.88 | 1.51 | 1.17–1.95 | |||||
| Colon | 0.91 | 0.72–1.15 | - | - | |||||
| Grading | |||||||||
| 1 | Reference | - | - | - | |||||
| 2 | 1.08 | 0.75–1.57 | - | - | |||||
| 3 | 1.22 | 0.84–1.77 | - | - | |||||
| 4 | 1.35 | 0.90–2.01 | - | - | |||||
-: these variables were not entered in the final model; Reference: reference group
A growing number of resected LNs in patients with CRC may lead to more accurate staging and better determining the need for adjuvant chemotherapy [14]. The finding of this study showed that DFS and OS were higher in patients with more than 20 removed LNs compare to the control group with less than 20 resected LNs. We also found a remarkable relationship between the number of involved LNs and age and the number of resected LNs, DFS, and OS; the patients with involved LNs had a worse OS and DFS compared to patients without involved LNs. These results support that an increased number of LN resection increases the chance of finding node-positive and helps clinicians accurately evaluate patients’ stages, leading to better survival.
Our findings were in line with the investigation results indicating that the likelihood of identifying a positive node increases as more nodes are examined. Wong et al. [15] findings showed that a higher number of nodes evaluated results in a lower node-negative rate. An increase in node sampling will improve DFS in patients with node-negative in comparison with node-negative patients with fewer nodes evaluated [15]. Berger et al. [16] reported a significant association between the total number of LNs and LN ratio (ratio of metastatic to examined LNs) with OS and DFS while they demonstrated that the LNs ratio of more than 10 was an important prognostic factor for OS and DFS.
Our result did not show any relation between LNs ration and OS or DFS, which might be due to the smaller sample size in our study. A study by Le Voyer et al. [17] showed that the number of LNs is a prognostic factor for survival time among patients with colon cancer. Noteworthy, an Asian retrospective study conducted by Huang et al. [18] indicated that LN distribution had a better predictive value than the TNM system in CRC patients. Another trial by Rausei et al. [19] clarified that nodal involvement is the strongest predictor for CRC. In line with our experience, a trial in Brazil by Jacomo et al. [20] in 2011 on 90 patients with rectal cancer revealed that the number of LNs affected the five-year survival in patients with CRC. Accordingly, in another investigation by Bando et al. [21], 650 patients supported these results and revealed that the number of retrieved LNs affects 5-year survival. Furthermore, some authors have detected that the LNs ratio is the most important prognostic factor for both OS and DFS in patients with CRC [22–24]. In the previous study, with 82,896 patients recruited from a big cancer database, Chen and Bilchik [6] reported that adequate LN resection correlates with improved survival in all stages examined. In 2007, a systematic review conducted by Chang et al. [25] the data of 61,371 patients from 16 studies demonstrated a positive correlation between the number of LNs examined and survival in CRC. Overall, there is general agreement about the prognostic implications of LNs involvement for OS and DFS obtained from several other studies and our study [26–28].
Several authors have investigated the impact of other factors such as demographic and clinicopathological variables on survival and DFS time. To evaluate the LNs preoperatively, Nakai et al. [29] reported that the addition of positron emission tomography (PET) to computed tomography (CT) could be beneficial to confirm LNs metastasis in CRC patients. Several studies have focused on the different surgical strategies in CRC patients. Based on Du et al. [30] meta-analysis, laparoscopic lateral LN dissection (LLND) surgery is recommended to be a better alternative treatment strategy compared to conventional open LLND to lower postoperative morbidity and shorter length of hospital stay for advanced CRC.
These studies indicated that age and sex were prognostic factors for survival in CRC patients [31, 32]. In current practice, we performed multivariate Cox regression analysis and assessed the role of other factors such as sex, age, body surface, location of the tumor, and type of tumor on the prediction of survival time and DFS time. We identified that only age was a significant predictor for OS and DFS in patients with CRC. The relation between the numbers of LNs and the location of the tumor, height, weight, and body surface was significant and the harvested LNs in men were more than in women.
Furthermore, the number of nodes that must be examined to yield a reliable assessment of the patient’s nodal status has been debated in various studies. This study demonstrated that the lowest number of LN for improving DFS is 20. Since we did not have access directly to the patient’s time of death among patients, measurement of HR for death was not possible, but we found a high correlation between DFS and OS. Therefore, we could conclude that DFS is a good indicator of OS among patients with CRC. Different studies indicate different cut-off points for LN resection [33–37]. There is an increase in either OS or DFS if more than 20 LNs are examined because of accurate staging and correct management. In 1990, the Working Party Reports to the World Congress of Gastroenterology suggested that at least 12 LNs should be resected to stage patients accurately [33]. Similarly, Tsai et al. [34] found that an adequate number of examined LNs is at least 12. Wong et al. [35] find that fewer nodes were examined in node-negative patients than node-positive-patients (14 v20), and to reach a nodal positivity rate commensurate with the National Cancer Data Bank, a minimum of 14 LNs should be examined. Wei et al. [36] showed that CRC patients with LN yield 20 and greater were associated with better survival. This study also showed a higher LN yield might be considered a prognostic marker [36]. Therefore, to accurately stage a patient with colon cancer, it is better to examine as many nodes as possible.
A study conducted by Kukreja et al. [37] indicated that retrieving at least 12 LNs as a practical modality appeared to have no foundation. These different findings may suggest that in addition to the number of LNs, some other important factors affect the number of LNs, such as surgical procedures and pathological methods, in evaluating LNs. Moreover, the sample size and research design have an impact on different findings in studies. This study’s strength was a large number of subjects with a historical prospective design at the time of conception.
Some limitations should be considered when interpreting this study’s results, such as the lack of some data in the patients’ files and the patients’ precise time of death. Therefore, to overcome this problem, future clinical trials in CRC should have specific clinical research teams for these evaluations.
In conclusion, this historical cohort proved that LN involvement and the number of resected LNs affect the OS and DFS time, increase the number of LNs improves staging CRC, and better patient management. We recommend that the minimum number of LNs for improving OS and DFS is 20 and more.
AJCC: American Joint Committee on Cancer staging system
AJCC-8th: eighth edition of the American Joint Committee on Cancer staging system
CI: confidence interval
CRC: colorectal cancer
DFS: disease-free survival
HR: hazard ratio
LNs: lymph nodes
OR: odds ratio
OS: overall survival
SD: standard deviation
TNM: tumor-node-metastasis
The authors express their gratitude towards the staff members of Seyyed-Al-Shohada hospital for their valuable assistance in locating and reviewing the patients’ charts throughout the study. The authors also thank Mr. Nariman Khorsandiardebili for his technical assistance (writing service) in editing the manuscript.
RMR and FMR: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. EM and SM: Conceptualization, Data curation, Investigation, Methodology, Resources, Supervision, Validation, Writing—original draft, Writing—review & editing. MT: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing—original draft, Writing—review & editing. AE: Conceptualization, Data curation, Investigation, Methodology, Resources, Supervision, Writing—original draft, Writing—review & editing. AN: Conceptualization, Investigation, Methodology, Resources, Validation, Writing—original draft, Writing—review & editing. SFH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing—original draft, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The Isfahan University of Medical Sciences Review Board granted ethical approval (No. IR.MUI.REC.1395.2.228) for this study, which complied with the Declaration of Helsinki.
Informed consent to participate in the study was obtained from all participants.
Informed consent to publication was obtained from relevant participants.
Data and materials are available upon request from the corresponding author (Sayyideh Forough Hosseini, drhosseini.forough@gmail.com).
Not applicable.
© The Author(s) 2023.
Copyright: © The Author(s) 2023. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 4015
Download: 31
Times Cited: 0