 Review
Review

Affiliation:
Department of Infectious Disease, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
ORCID: https://orcid.org/0000-0001-8094-8544
Affiliation:
Department of Infectious Disease, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
ORCID: https://orcid.org/0009-0000-6011-3670
Affiliation:
Department of Infectious Disease, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
ORCID: https://orcid.org/0009-0000-3756-5257
Affiliation:
Department of Infectious Disease, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
ORCID: https://orcid.org/0000-0002-0674-4225
Affiliation:
Department of Infectious Disease, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
Email: xujie@shsmu.edu.cn
ORCID: https://orcid.org/0000-0002-9179-0049
Explor Dig Dis. 2026;5:1005127 DOI: https://doi.org/10.37349/edd.2026.1005127
Received: March 22, 2026 Accepted: May 07, 2026 Published: July 01, 2026
Academic Editor: Jose C. Fernandez-Checa, Institute of Biomedical Research of Barcelona (IIBB), CSIC, Spain
The article belongs to the special issue Viral Hepatitis
Hepatitis E virus (HEV) is a major global health concern, evolving from a self-limited enteric infection to a complex systemic disease with an expanding burden. This narrative review synthesizes current evidence on HEV virology, epidemiology, zoonotic transmission, and clinical manifestations to inform clinicians, researchers, and policymakers. Despite substantial morbidity among pregnant women and immunosuppressed patients, HEV awareness remains limited, and therapeutic options are constrained. Four genotypes (1–4) show distinct epidemiological patterns; chronic infection occurs primarily in immunocompromised hosts, while extrahepatic manifestations, including neurological and renal complications, are increasingly recognized. Treatment remains limited to ribavirin with variable efficacy and contraindications. The HEV-239 vaccine demonstrates sustained efficacy but requires broader implementation. This review integrates recent advances across virology, clinical practice, and public health, offering a unified framework for understanding HEV as a systemic disease requiring enhanced surveillance, targeted antiviral development, and expanded vaccine deployment within a “One Health” framework.
Hepatitis E virus (HEV) was discovered in 1983 during an investigation of an unexplained hepatitis outbreak among Soviet soldiers in Afghanistan [1]. Experimental self-inoculation using pooled fecal extracts from affected individuals led to acute hepatitis, and subsequent immunoelectron microscopy detected viral particles in feces. The HEV genome was later cloned and sequenced from bile samples obtained from experimentally infected cynomolgus macaques [2, 3]. The HEV induces acute-to-chronic hepatic disease chiefly through fecal-oral contamination. WHO surveillance data document roughly twenty million annual infections globally, precipitating 3.3 million clinical cases and seventy thousand mortalities. Specifically, 2021 statistics recorded 19.47 million acute episodes, contributing to 5.4% of acute hepatitis-related disability-adjusted life years. Contemporary expansion of transmission routes and host spectrum stems from enhanced nucleic acid detection methods and characterization of animal-adapted HEV genotypes. Notably, disease endemicity disproportionately affects developing economies, whereas sporadic indigenous infections show upward trajectories in developed settings [4]. This review systematically synthesizes recent progress in molecular biology, epidemiological patterns, clinical diagnosis, pathogenic mechanisms, therapeutic strategies, and preventive measures for HEV infection.
HEV presents as a small, spherical, nonenveloped particle harboring a positive-sense, single-stranded RNA genome of ~7.2 kilobases (kb). Its morphological and biophysical characteristics bear the closest resemblance to caliciviruses. Taxonomically, HEV belongs to the family Hepeviridae, specifically the species Orthohepevirus A. The viral genome spans approximately 7.5 kb and comprises three discrete open reading frames—ORF1, ORF2, and ORF3—predicted to encode nonstructural and structural polypeptides based on conserved consensus motifs and genomic architecture [5, 6]. Genomic size varies among HEV species, spanning 7.2–7.6 kb, with each isolate harboring a minimum of three open reading frames. Positioned at the 5' terminus, ORF1 (~2 kb) directs synthesis of non-structural polypeptides, notably the RNA-dependent RNA polymerase (RdRp) essential for viral replication. At the 3' end, ORF2 (approximately 2 kb) constitutes the primary structural locus encoding the capsid protein. ORF3 (369 bp), overlapping both adjacent reading frames, additionally specifies a structural antigen utilized for serological diagnosis. Functionally, ORF3 proves indispensable for viral fecal excretion and maintenance of persistent infection [7]. The Viral ORF3 Protein Is Required for Hepatitis E Virus Apical Release and Efficient Growth in Polarized Hepatocytes. Species Orthohepevirus A has been isolated from mammals—mostly humans, but also pigs and wild boar, which have been classified into eight genotypes (HEV-1 to HEV-8) differing in nucleotide sequence in the ORF2 region [8–10].
Comprehensive phylogenetic interrogation of full-length genomes and subgenomic fragments from diverse HEV isolates resolved four principal genotypes (HEV-1–HEV-4) [11].
Novel HEV variants exhibiting augmented cross-species transmission capacity have emerged. Viral isolation from unconventional reservoirs—including rodents and dairy cattle—reveals genomic and antigenic hallmarks indicative of enhanced species barrier permeability.
Rocahepevirus ratti (rat HEV) represents an emerging zoonotic hepatotropic agent with global distribution [12]. Clinical manifestations span asymptomatic self-resolution to fulminant hepatic failure and chronic persistence in immunocompromised hosts [13, 14]. To date, human infections remain rare, with documented cases restricted to Hong Kong (China), Spain, France, and Canada [15–17].
Evolutionary adaptation analyses reveal that emerging variants exhibit marked ORF1 codon-usage patterns skewed toward human-preferred triplets relative to pig/rodent lineages, signifying positive Darwinian selection for optimized translational fidelity in the new host—a pivotal molecular determinant underpinning expanded host range [18].
Empirical investigations have established that the bovine-adapted HEV-3 clade (CHN-XJ-SW13-like) maintains infectious virions in mammary secretions and traverses the alimentary epithelium through either experimental gavage or natural nursing, eliciting systemic dissemination in rhesus macaques with extended nephrotropic shedding. These findings implicate dual-route transmission potential encompassing both alimentary and parenteral/secretory pathways [19].
HEV exhibits broad host tropism as shown in Figure 1, infecting humans and diverse mammalian and avian species, including swine, lagomorphs, rodents, cervids, herpestids, and galliformes. Human disease is predominantly attributable to genotypes 1–4, with sporadic cases linked to HEV-7. Geographic segregation characterizes these lineages: HEV-1 and HEV-2 are obligate human pathogens transmitted via fecally contaminated water, precipitating large-scale waterborne epidemics across hyperendemic zones spanning Asia, Africa, and Latin America [20–22]. Conversely, HEV-3 and HEV-4 demonstrate zoonotic ecology, maintaining enzootic circulation in porcine, suid, and cervid reservoirs. Genotype 3 predominates in Western nations alongside Asian and North American regions, whereas genotype 4 exhibits restricted distribution across Asia and Europe. These zoonotic genotypes disproportionately affect high-income populations, with transmission dynamics driven by ingestion of inadequately cooked infected animal products and contaminated water sources—underscoring the indispensability of potable water and sanitary infrastructure [23].
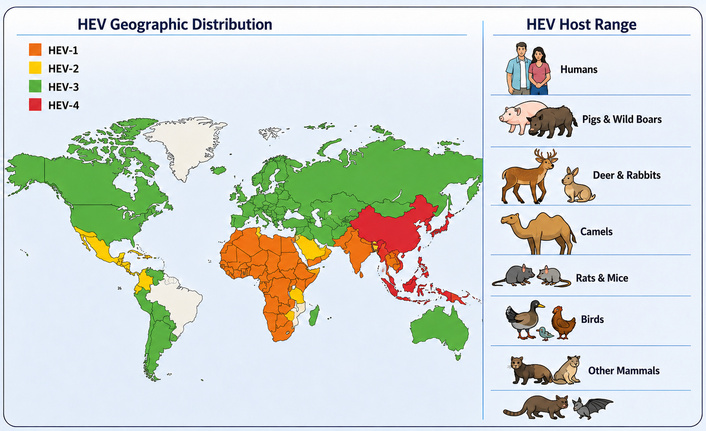
Hepatitis E virus (HEV) geographic distribution and host range. This figure illustrates the global distribution of HEV genotypes alongside their diverse host range, highlighting the virus’s broad cross-species transmission potential and its significance within a “One Health” framework.
Beyond enteric exposure, vertical transmission, transfusion-associated infection, and graft-related transmission have emerged as clinically significant routes. Hematogenous spread via contaminated blood products represents particular concern in endemic settings. A large-scale surveillance initiative screening 225,000 donations identified 79 viremic units harboring HEV-3 RNA. These contaminated donations yielded 129 blood components, of which 62 were administered. Recipient follow-up documented 18 seroconversions among 43 tested individuals [24]. Subsequent North American screening (United States and Canada) revealed differential prevalence: 1:16, 908 US donations contained detectable HEV RNA, with elevated rates observed in Canadian samples [25].
Vertical transmission poses substantial perinatal risk, with documented intrapartum transmission causing significant neonatal morbidity and mortality [26, 27]. Lactogenic transmission remains uncertain, though infectious HEV has been recovered from breast milk at titers comparable to serum, warranting temporary breastfeeding cessation in confirmed cases [28].
China has established a comprehensive research infrastructure spanning HEV basic virology, molecular epidemiology, clinical investigation, vaccine development, and public health implementation. These multifaceted contributions have substantially shaped international research paradigms and control strategies.
In 1999, Chinese scholars reported the complete genomic sequence of a prototype genotype 4 HEV strain, recovered directly from fecal specimens of an acutely infected individual [31]. Further confirmed genotype 4 as the dominant circulating lineage in both human and porcine reservoirs, with principal risk determinants encompassing consumption of untreated water, ingestion of raw or inadequately cooked pork products, and occupational exposures including swine husbandry and abattoir work. Notably, genotype 4 exhibits distinctive genomic architecture: a single nucleotide insertion within the ORF3 region alters translational initiation, with potential downstream effects on ORF2 expression [32].
Pioneering work by domestic epidemiologists and infectious disease specialists—notably Academician Zhuang Hui—encompassed longitudinal population surveillance, epidemiological synthesis, and scientific advocacy. These endeavors progressively elucidated indigenous transmission dynamics (fecal-oral, waterborne, and foodborne routes) and demographic risk profiles [33, 34]. Chinese scholars have proposed policy recommendations to strengthen hepatitis E surveillance and enhance outbreak early warning [35]. They suggest implementing household drinking water chlorination disinfection and reducing disease burden by investing in transportation infrastructure to improve healthcare accessibility in remote areas [36, 37].
In the domain of prophylactic development, Professor Ning-Shao Xia and colleagues at Xiamen University pioneered the recombinant hepatitis E vaccine HEV-239 (trade name Hecolin®), representing the first globally licensed and clinically validated HEV immunization [38, 39]. Phase III efficacy trials and extended longitudinal follow-up documented favorable tolerability and durable protective immunity, with sustained effectiveness demonstrated across multi-year observation periods [40]. They advocate for incorporating the hepatitis E vaccine into similar national immunization program strategies [41] and have identified characteristics of high-risk populations to provide decision-makers in China and other endemic countries with priority intervention targets [42]. Such foundational work directly informed regional surveillance systems for disease control and prevention in hepatitis E patients in China [43].
Accumulating evidence establishes that host immunogenetic responses to distinct HEV genotypes critically govern infection outcomes. HEV subverts innate immunity through antagonism of interferon induction and signal transduction. Cellular immunity—specifically T-lymphocyte responses—drives viral elimination, whereas humoral immunity and neutralizing antibodies confer sterilizing protection and durable immunity against reinfection. Both active and passive immunization strategies demonstrate efficacy in preventing severe acute hepatitis in the majority of cases [44].
Decades of investigation into HEV pathogenesis have been constrained by the absence of robust in vitro culture systems and animal models that faithfully recapitulate human disease pathology. Although fecal-oral transmission represents the principal route, the precise mechanism of viral dissemination from the gastrointestinal tract to hepatic parenchyma remained elusive. Recent advances demonstrate that primary intestinal epithelial cultures support replication of both genotype 1 and genotype 3 HEV, with viral RNA and ORF2 antigen detectable in intestinal crypts of chronically infected patients [45]. These observations identify the intestinal mucosa as the initial replication site prior to hepatocyte invasion and subsequent hepatitis development. The majority of HEV particles undergo apical membrane release (biliary surface) [46]; bile salt-mediated lipid envelope stripping generates naked virions excreted in feces [1].
HEV-induced hepatocellular injury operates through multifactorial mechanisms, integrating direct viral cytopathicity and immune-mediated damage as shown in Figure 2. Viral replication within hepatocytes and extrahepatic tissues—including placental and neural compartments—contributes to direct parenchymal injury. Hepatic damage is additionally attributable to cytotoxic T-lymphocyte and natural killer cell-mediated cytotoxicity [47]. Excessive immune activation—particularly cytotoxic T-cell-mediated apoptosis and proinflammatory cytokine cascades—precipitates hepatocyte necrosis. Recent evidence further implicates non-virus-specific CD8+ T-lymphocytes in hepatic immunopathology [48]. The equilibrium between viral replication kinetics and host immunologic control fundamentally determines disease severity and clinical progression. Specifically, coordinated CD4+ and CD8+ T-cell responses are requisite for preventing chronic viral persistence [49].
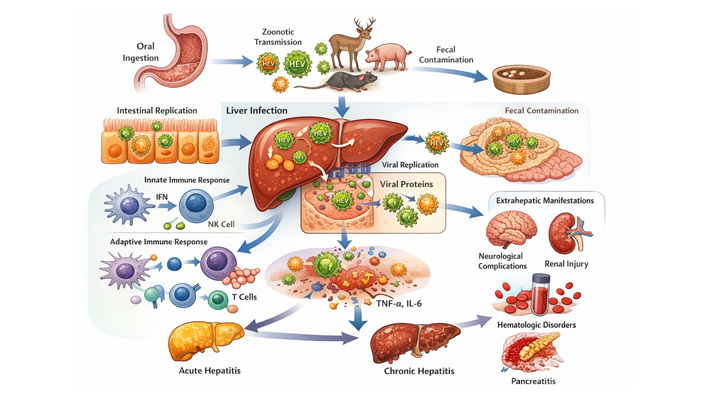
Pathogenesis and extrahepatic manifestations of hepatitis E virus (HEV) Infection. HEV infection begins when the virus is ingested through contaminated food or water, replicates in the intestines, and enters the bloodstream. It then infects the liver, causing inflammation and acute hepatitis, which is typically self-limiting in immunocompetent individuals. However, in immunocompromised populations, the immune response is insufficient, leading to chronic infection. HEV infection can also result in extrahepatic manifestations, including neurological complications, renal issues, hematologic disorders, and, in some cases, pancreatitis. In immunocompromised individuals, chronic HEV infection can progress to cirrhosis if left untreated. Reducing immunosuppressive therapy in some patients has been shown to promote viral clearance.
Although historically classified as non-enveloped, HEV has been demonstrated to egress from infected cells as quasi-enveloped virions (eHEV) [50]. These membrane-associated particles circulating in the bloodstream exhibit resistance to neutralizing antibody-mediated inactivation, thereby facilitating covert dissemination [51]. Relative to fecal non-enveloped virions, eHEV harbors additional structural components, including host-derived lipid membranes and the viral ORF3 protein [52]. Compelling evidence supports the essential function of ORF3 in quasi-enveloped particle biogenesis.
The HEV ORF3 protein exhibits intrinsic secretory capacity, with N-terminal cysteine palmitoylation requisite for both secretion and quasi-enveloped virion formation [53]. Mechanistically, palmitoylated ORF3 selectively hijacks Annexin II for cytoskeletal transport, subsequently routing to multivesicular bodies via the nSMase-ESCRT-III pathway for extracellular release. Furthermore, experimental infection of Mongolian gerbils with ORF3 palmitoylation-deficient mutants demonstrated abolished fecal shedding despite competent hepatic replication [54].
HEV infection manifests across a broad clinical continuum, extending from subclinical or mild self-limited hepatitis to fulminant hepatic failure. Following an incubation period of 2–6 weeks [55], infected individuals typically develop nonspecific prodromal manifestations—including pyrexia, malaise, anorexia, nausea, and abdominal discomfort—subsequently progressing to icterus, darkened urine, and hepatomegaly.
In immunocompetent hosts, acute infection typically follows a self-limited course, with spontaneous resolution within 4–6 weeks and absence of chronic sequelae [4]. However, specific demographic groups and clinical contexts predispose to severe or fulminant disease progression.
Chronic infection is defined by persistent hepatic enzyme elevation coupled with detectable HEV RNA in serum and/or stool for ≥ 3 months. The first documented cases emerged in 2008 among solid organ transplant (SOT) recipients with genotype 3 infection [56], followed by reports in human immunodeficiency virus (HIV)-positive individuals [57]. Chronicity predominantly affects immunosuppressed populations, including transplant recipients [58], patients with hematologic malignancies, individuals receiving chemotherapeutic or immunosuppressive regimens [59], those with autoimmune disorders (e.g., rheumatic conditions) undergoing immunomodulatory therapy [60], and advanced HIV infection. Established predictors of chronic evolution include prolonged immunosuppression, elevated baseline viremia, genotype 3 infection, and reduced CD4+ T-lymphocyte counts [61].
Severe disease evolution is determined by host determinants, viral genotype, and comorbid burden. Biochemical and virologic indices portending hyperbilirubinemia encompass pronounced, high viral load and elevated total bile acids [62, 63]. Previous comorbidities, including chronic liver, lung, and kidney diseases, tumours, and diabetes, were independent risk factors for adverse outcomes in acute HEV infections [64]. Genotypes 1 and 2 typically induce self-limited icteric hepatitis in immunocompetent hosts; however, gravid populations exhibit exceptionally poor prognosis, with maternal case fatality approaching 65% [65–67]. Pregnancy-associated mortality is attributed to gestational hormonal perturbations (elevated estrogen and progesterone) and consequent immunologic reprogramming. These alterations comprise NF-κB p65 subunit downregulation, Th2-skewed T-cell polarization, and human leukocyte antigen (HLA)-mediated susceptibility loci. The intricate interplay among endocrine modulation, compromised cellular immunity, and dysregulated cytokine cascades culminates in extensive hepatocellular necrosis and fulminant hepatic failure [68]. Individuals with preexisting hepatopathy—chronic viral hepatitis (HBV/HCV), alcohol-related liver disease, or metabolic-associated steatosis liver disease—similarly experience severe manifestations attributable to diminished functional hepatic reserve [69].
Cellular immunodeficiency substantially elevates HEV chronicity risk. Quantitative meta-analytic evidence (2021) demonstrates markedly elevated seroprevalence across immunosuppressed cohorts: 26% (SOT), 23% (hematologic malignancies), 19% (HIV), with graded viremia rates (3%, 2%, 1%). Among SOT recipients specifically, active replication (RNA detectability) occurs in 1–2%. Pooled cohort evidence indicates ~66% of HEV-infected transplant recipients progress to chronic hepatitis despite variable progression kinetics across studies [70]. These epidemiologic data support mandatory HEV screening and preventive measures, particularly donor negativity prioritization. Tacrolimus exposure independently predicts chronic evolution, whereas immunosuppressive tapering achieves virologic clearance in approximately one-third of affected patients. SOT recipients manifest a distinctive HEV-associated clinical entity, initially reported in 2008 [56].
Active infection prevalence in this setting is 1–2% (RNA-positive). The pivotal 2011 Kamar et al. [71], a gastroenterology study of 85 SOT recipients, demonstrated 65.9% chronicity (56/85), with 60% persistent infection and 10% cirrhosis development within 2 years. This work defined chronic infection as RNA persistence > 3 months in blood or stool, carrying a significant fibrosis progression risk without treatment. Pathogenesis centers on severe immunosuppression, specifically calcineurin inhibitor-mediated T-cell impairment, preventing viral clearance. All immunosuppressed and chronically immunosuppressed patients share this susceptibility. Variable immunosuppressive regimens differentially modulate immunity and HEV infection through mechanism-specific actions [72].
In symptomatic individuals, hepatitis E classically manifests with icterus accompanied by constitutional symptoms—malaise, anorexia, nausea, emesis, abdominal discomfort, pyrexia, and hepatic enlargement [73]. Less frequently observed features include diarrheal illness, arthralgic complaints, and urticarial eruptions [74–77].
Although traditionally regarded as hepatotropic, accumulating clinical and experimental evidence demonstrates HEV’s expansive tissue tropism and capacity for extrahepatic dissemination across multiple organ systems. Viral replication extends beyond hepatocytes to diverse non-hepatic tissues, as shown in Table 1, including neural parenchyma, renal parenchyma, hematopoietic elements, pancreatic acini, and placental trophoblasts. Such multi-organ involvement constitutes an increasingly recognized hallmark of HEV pathogenesis, particularly among immunosuppressed or chronically infected hosts. Consequently, affected individuals may present with extrahepatic manifestations (EHMs), encompassing neurological dysfunction, renal injury, acute pancreatic inflammation, endocrinopathies, hematologic cytopenia, and placental pathology [78].
Systemic tropism and extrahepatic manifestations of HEV.
| System | Affected tissues/organs | Main clinical manifestations | Mechanisms/Features | Notes |
|---|---|---|---|---|
| Overall (systemic tropism) | Neural tissue, renal parenchyma, hematopoietic system, pancreatic acini, placental trophoblasts | Multisystem extrahepatic manifestations (neurological, renal, hematologic, pancreatic, endocrine, placental, etc.) | Viral replication occurs in non-hepatic tissues; direct cytopathic effects + immune-mediated injury | More common in immunosuppressed or chronically infected patients |
| Neurological system | Central and peripheral nervous systems | Radiculoplexopathy (most common), meningoencephalitis, Guillain-Barré syndrome; also acute transverse myelitis, aseptic meningitis, neurogenic muscular atrophy, pseudotumor cerebri, bilateral pyramidal tract dysfunction | HEV genotype 3 shows a higher propensity for neurological complications; CNS and PNS involvement may occur independently or concurrently | The most common type of extrahepatic manifestation |
| Hematologic system | Red blood cells, platelets, etc. | Hemolytic anemia (especially in G6PD deficiency), autoimmune hemolytic anemia, severe thrombocytopenia (including immune thrombocytopenic purpura) | Oxidative stress-induced hemolysis; molecular mimicry and immune complex-mediated destruction of blood cells | May precede or coincide with hepatic dysfunction |
| Renal system | Glomeruli (mesangium, capillary loops) | MPGN, IgA nephropathy (recurrence or de novo) | Immune complex deposition and complement activation; mucosal immune dysregulation leading to IgA deposition | Cryoglobulinemia influences severity and treatment |
| Pancreatic system | Pancreatic acinar cells | Acute pancreatitis (ranging from mild to necrotizing) | Mechanism not fully defined; temporal relationship with HEV infection varies | May precede jaundice |
| Rheumatologic system | Joints, synovium, blood vessels | Inflammatory arthropathy (from self-limited to erosive polyarthritis), rheumatoid arthritis-like presentation; cryoglobulinemic vasculitis (arthralgia, purpura, peripheral neuropathy) | Molecular mimicry and immune complex deposition | Symptoms may persist after viral clearance |
| Other autoimmune-related | Myocardium, thyroid, etc. | Myocarditis, thyroiditis | Associated with autoimmune mechanisms | Less frequently reported |
| Obstetric/Placental system | Placental trophoblasts, endothelial cells | Fulminant hepatic failure, miscarriage, intrauterine fetal death | Viral replication leads to apoptosis, tissue necrosis, and inflammatory cytokine cascades | High risk in pregnancy |
G6PD: glucose-6-phosphate dehydrogenase; HEV: hepatitis E virus; MPGN: membranoproliferative glomerulonephritis.
Among EHMs, neurological complications predominate. Both peripheral and central nervous system involvement may manifest concurrently or independently. Radiculoplexopathy represents the most frequently reported neural syndromes, followed by meningoencephalitis and Guillain-Barré syndrome [79]. Additional documented conditions include acute meningoencephalitis, acute transverse myelitis, aseptic meningitis, neurogenic muscular atrophy, pseudotumor cerebri, and bilateral pyramidal tract dysfunction. Notably, HEV-3 genotype demonstrates a particular propensity for inducing neurological sequelae [80, 81].
HEV-associated hematologic complications encompass a spectrum of cytopenia and autoimmune phenomena. Glucose-6-phosphate dehydrogenase (G6PD) deficiency-related hemolytic anemia represents a specific vulnerability, wherein oxidative stress induced by HEV infection precipitates acute hemolysis in enzymopathy individuals [77]. Autoimmune hemolytic anemia and severe thrombocytopenia—occasionally manifesting as immune thrombocytopenic purpura—have been documented, with proposed mechanisms involving molecular mimicry and immune complex-mediated destruction of blood cell lineages [60]. These hematologic abnormalities may precede or coincide with hepatic dysfunction, underscoring the necessity for comprehensive blood count surveillance in HEV-infected patients.
HEV infection has emerged as a recognized trigger for immune-mediated renal injury. Membranoproliferative glomerulonephritis (MPGN)—frequently associated with cryoglobulinemic vasculitis—represents the prototypical HEV-related nephropathy, characterized by immune complex deposition and complement activation. Additionally, IgA nephropathy recurrence or de novo presentation has been observed, with HEV infection potentially exacerbating mucosal immune dysregulation and mesangial IgA deposition [77, 82]. The presence or absence of cryoglobulinemia substantially modulates clinical presentation and therapeutic approach, with cryoglobulinemic vasculitis portending more severe systemic involvement [83]. Renal biopsy with immunofluorescence and electron microscopy remains essential for definitive diagnosis and pathogenetic characterization [84].
Acute pancreatitis constitutes an increasingly recognized, though underreported, EHM of HEV infection. Clinical presentation ranges from mild, self-limited pancreatic inflammation to severe necrotizing pancreatitis with systemic complications [85, 86]. The temporal relationship between hepatitis onset and pancreatic symptoms varies, with pancreatitis occasionally preceding icterus [87]. Serum amylase and lipase measurement should be considered in HEV-infected patients presenting with abdominal pain, particularly when disproportionate to hepatic enlargement or when accompanied by characteristic radiation to the back.
HEV infection has been implicated in diverse immune-mediated rheumatic conditions, predominantly manifesting as inflammatory arthropathy. Clinical patterns range from transient, self-limited osteoarthritis to persistent, erosive polyarthritis mimicking rheumatoid arthritis [60, 88]. Additionally, HEV has been associated with cryoglobulinemic vasculitis presenting with arthralgias, cutaneous purpura, and peripheral neuropathy—frequently overlapping with renal involvement [77]. Rheumatologic symptoms may persist beyond viral clearance, suggesting sustained autoimmune activation in susceptible individuals [88]. Rheumatologic evaluation, including inflammatory markers, autoantibody profiling, and synovial fluid analysis, is warranted in HEV-infected patients with persistent musculoskeletal complaints.
And other autoimmune EHMs of HEV, such as myocarditis and thyroiditis, have also been reported [89].
In gravid populations, HEV exhibits pronounced placental affinity. Replication within placental trophoblasts and endothelial cells triggers apoptotic cell death, tissue necrosis, and pro-inflammatory cytokine cascades, precipitating severe maternal-fetal outcomes including fulminant hepatic failure, spontaneous pregnancy loss, and intrauterine fetal demise [90].
The pathophysiologic mechanisms underlying multi-organ involvement encompass both direct cytopathic effects in susceptible tissues and immune-mediated injury secondary to systemic viremia. This pleiotropic tropism positions HEV as a systemic rather than exclusively hepatocentric infection, necessitating comprehensive diagnostic evaluation—particularly in atypical or extrahepatic presentations [91]. Importantly, EHM severity does not invariably correlate with hepatic disease severity; asymptomatic HEV infection may precipitate systemic illness. Patients exhibiting systemic HEV manifestations warrant prioritized antiviral intervention, which may ameliorate or resolve associated extrahepatic pathology [45].
HEV infection diagnosis fundamentally depends on serologic and molecular biological assays. Recent technological advances in antigen detection and multiplex platform development have enhanced early diagnostic sensitivity—particularly critical for immunosuppressed populations [4]—with anti-HEV antigen demonstrating high diagnostic specificity and sensitivity [92].
For acute infection evaluation, initial assessment employs an anti-HEV immunoglobulin M (IgM) immunoassay; serum IgM positivity indicates acute infection, whereas immunoglobulin G (IgG) detection signifies past exposure. Given suboptimal single-platform enzyme immunoassay specificity, positive screening results require confirmatory validation when available. Confirmatory methodologies encompass alternative IgM testing, documentation of rising IgG titers (> 5-fold increase over 14 days), or HEV RNA detection in serum or stool [93]. IgM responses emerge early in clinical illness but wane rapidly within 4–5 months [94]. Although outbreak investigations demonstrate IgM detection in > 90% of cases when sampling occurs within 1–8 weeks of symptom onset, seronegativity persists in substantial acute infection proportions [95].
When initial enzyme immunoassay yields negative results despite strong clinical suspicion, HEV RNA detection remains the diagnostic “gold standard”, implementable through real-time quantitative RT-PCR of blood or stool specimens. For suspected chronic infection, serum HEV RNA detection constitutes the diagnostic mainstay, with chronicity defined as persistent RNA positivity in serum or stool exceeding 3 months. Recent evidence highlights that molecular diagnostics, particularly nucleic acid amplification tests (NAATs), have become indispensable for detecting HEV infection in immunocompromised patients [96]. In these populations—including SOT recipients, patients with hematological malignancies, and those receiving biologics—seroconversion is frequently impaired, rendering anti-HEV IgM/IgG unreliable. HEV RNA detection enables early identification of active infection, often preceding or even replacing serological responses. Importantly, it allows accurate diagnosis of chronic HEV infection, which is now increasingly recognized in immunosuppressed hosts, especially with genotype 3. Chronic HEV infection occurs predominantly in immunocompromised patients, and serological antibody negativity may arise in this population, necessitating concomitant nucleic acid testing (e.g., PCR) for definitive diagnosis [97–100].
HEV antigen (HEV-Ag) testing offers advantages in resource-limited settings. Recent advances include urinary HEV-Ag colloidal gold immunochromatographic assays for non-invasive screening [101]. However, antigen presence does not always correlate with active viral replication, so combined serological and molecular approaches remain recommended for immunocompromised patients [102].
Four genotypes account for the majority of human HEV infections: genotypes 1 and 2 represent obligate human pathogens, whereas genotypes 3 and 4 maintain primarily zoonotic transmission cycles. Historically, HEV was regarded as the principal agent of waterborne hepatitis epidemics in developing regions, driven by fecal contamination of drinking water. However, contemporary recognition increasingly acknowledges HEV endemicity in industrialized nations, where transmission occurs through zoonotic exposure or contaminated blood products, with particular propensity for chronic infection in immunocompromised hosts. Diagnosis relies on the detection of anti-HEV antibodies, viral RNA, or capsid antigen in serum or stool. Despite vaccine availability, licensure remains restricted to China. Acute infection typically follows a self-limited course without specific therapeutic requirements. Immunocompromised patient management involves immunosuppressive dose reduction and/or ribavirin antiviral therapy [4].
Approved therapeutic modalities remain constrained to off-label ribavirin monotherapy and, in select cases, pegylated interferon-α [103]. Among immunosuppressed populations—SOT recipients, hematologic malignancy patients, and HIV-positive individuals—approximately 60–70% of infections progress to chronicity, with hepatic fibrosis or cirrhosis developing within 24–36 months [102]. Ribavirin dosing for HEV treatment varies widely (29–1,200 mg/day), primarily extrapolated from HCV experience with renal adjustment. Treatment duration ranges from 1 to 18 months. It is recommended a 3-month initial course, extending by 3 months if HEV RNA persists; alternatively, monthly RNA monitoring with 3 months of continued therapy after first negativity [104, 105].
Pegylated interferon-α has demonstrated efficacy in limited case series of liver transplant recipients and hemodialysis patients, achieving virologic clearance following 3-month therapy. However, interferon is generally contraindicated in kidney, pancreatic, cardiac, and pulmonary transplant recipients due to immune-stimulatory effects and an elevation in acute rejection risk. Ribavirin-associated adverse events include dose-dependent anemia, dry cough, and dermatologic reactions. Given frequent comorbid renal impairment and anemia in chronic hepatitis E patients, ribavirin requires cautious dosing with hemoglobin and estimated glomerular filtration rate-guided dose adjustments [106]. Additionally, interferon exacerbates rejection risk in transplant populations [107–109].
Recent studies have identified novel direct-acting antivirals targeting the HEV RdRp, as well as host-targeting agents that interfere with viral replication complexes. JNJ-9117, a sugar-modified guanosine analog targeting HEV RdRp, is the most promising candidate. It demonstrates pan-genotype activity (HEV-1, HEV-3) with IC50 of 21–30 nmol/L—300-fold more potent than ribavirin [110]. Other candidates include the cathepsin inhibitor K11777 (blocks viral entry) and METTL3/FTO inhibitors targeting RNA methylation pathways [111].
In vitro investigations demonstrate divergent effects: mammalian target of rapamycin (mTOR) inhibitors enhance HEV replication, whereas mycophenolate mofetil exhibits suppressive activity [112]. Clinical relevance remains incompletely defined. Although mycophenolate use correlated with reduced chronic hepatitis E incidence in one cardiac transplant cohort, treated patients still develop persistent infection [113].
Some patients progress to hepatic decompensation. Corticosteroid therapy has been empirically administered in individual acute liver failure cases retrospectively attributed to HEV, with associated biochemical improvement. However, insufficient evidence currently supports routine corticosteroid use in HEV-related acute liver failure [114].
Suboptimal efficacy, poor tolerability, and adverse effects limit both therapeutic options. Furthermore, antiviral pressure selects for HEV variants. Viral population dynamics critically influence treatment outcomes. Ribavirin, the sole available option for many patients, fails in select cases associated with the emergence of a distinct RdRp mutant (G1634R) [115]. This substitution enhances hepatocyte replicative fitness, increasing viral RNA synthesis and hepatic persistence, thereby attenuating ribavirin antiviral efficacy and promoting therapeutic failure [116]. Although variant emergence may contribute to ribavirin resistance, definitive causal attribution to treatment failure requires additional validation.
China’s domestically developed recombinant HEV vaccine (Hecolin®) received China Food and Drug Administration (CFDA) approval in December 2011. Zhu FC and colleagues [117] conducted a pivotal phase 3 efficacy trial enrolling 11,165 healthy adults (16–65 years), demonstrating > 90% protective efficacy with favorable safety characteristics. The World Health Organization (WHO) subsequently recommended outbreak deployment beginning in 2015. Extended follow-up investigations have confirmed durable protection persisting up to 10 years, with vaccine-induced antibodies detectable for ≥ 8.5 years—findings published in 2024 [38]. Additional milestone achievements include a phase 1 safety and immunogenicity trial in healthy US adults [118] and implementation of a two-dose emergency protocol during the South Sudan outbreak [119], contributing to epidemic containment. These cumulative accomplishments prompted the WHO International Coordination Group’s establishment of Hecolin emergency vaccine stockpiles.
Protection of potable water integrity and sanitation infrastructure enhancement remains fundamental for interrupting waterborne transmission predominantly attributable to genotypes 1 and 2 [120, 121]. Strengthened food safety surveillance and adequate thermal processing of animal-derived products—particularly porcine tissues—are critical for zoonotic genotype 3 and 4 transmission reduction. Appropriate heat treatment substantially diminishes infection risk [122, 123].
Furthermore, HEV RNA nucleic acid screening of blood and blood product donations has been integrated into transfusion safety systems across numerous nations, minimizing transfusion-transmitted infection risk [24, 124]. These multifaceted interventions collectively constitute the foundational framework for primary prevention and comprehensive HEV transmission control.
Although considerable advances have been made in HEV research, a number of scientific issues urgently require resolution.
Recently, the HEV vaccine developed for the prevention of human disease was approved in China, but it is not yet available to the rest of the world. The mechanisms underlying HEV variant emergence and cross-species transmission are not yet fully elucidated, with zoonotic transmission risks remaining a concern. HEV exemplifies how pathogens once categorized as “neglected tropical infections” can evolve into global zoonotic threats. The increasing detection of autochthonous cases in developed countries [24, 74] suggests that HEV surveillance must move beyond outbreak-based paradigms. Climate change, global food trade, and shifting animal husbandry practices may further alter transmission dynamics. Current public health frameworks remain reactive rather than anticipatory. Integrated “One Health” surveillance—linking veterinary, environmental, and human data—is critical to prevent further expansion.
Therefore, the immune evasion mechanisms in HEV infection warrant further investigation.
Recent studies suggest age-related immune modulation influences disease severity [48]. Effector memory CD8+ T-cell responses may contribute to pathogenesis in elderly patients. This raises important questions regarding immunosenescence and HEV outcomes.
The balance between protective and pathogenic immune responses remains incompletely defined [44, 45, 49]. Chronic infection likely reflects insufficient viral clearance, whereas severe acute hepatitis may involve exaggerated immune-mediated injury.
Future mechanistic studies integrating immunology, virology, and clinical phenotyping are essential.
Ribavirin monotherapy is currently the standard treatment for chronic HEV infection [106]. While effective in many patients, treatment failure and relapse occur, particularly in cases with high viral load or prolonged immunosuppression [71, 72]. Ribavirin-associated anemia limits tolerability. Pegylated interferon has shown efficacy but carries risks in transplant recipients [107, 108]. No HEV-specific direct-acting antiviral agents are currently approved [103]. Given increasing recognition of chronic HEV burden [58, 70, 72], the lack of targeted antivirals represents a major therapeutic gap. Drug development has lagged compared to HBV and HCV, possibly reflecting historical underestimation of HEV severity [99].
Meanwhile, notable progress and knowledge have been made and revealed in recent years to better understand HEV biology and infection. Special attention is focused on quasi-enveloped HEV virions and the potential role of the HEV ORF3 product as an antibody-neutralization target on the surface of quasi-enveloped HEV virions [52, 54, 61] to provide new insights for the future development of improved vaccines against zoonotic HEV infection.
The evolving landscape of HEV infection challenges earlier simplifications regarding transmission, pathogenicity, and clinical impact. Persistent uncertainties regarding genotype-specific virulence, mechanisms of chronicity, extrahepatic disease causality, diagnostic standardization, and antiviral development highlight the need for coordinated global research efforts.
Rather than viewing HEV as a solved problem with limited clinical consequence, it should be considered a dynamic and adaptive pathogen with expanding epidemiological relevance. Bridging current knowledge gaps will require multidisciplinary collaboration, improved molecular surveillance, and renewed prioritization in global hepatitis control strategies. Moreover, global vaccine deployment encounters ethical, economic, and policy challenges.
HEV infection represents a paradigm of evolving infectious disease complexity, challenging historical perceptions of a simple, self-limited enteric pathogen. Contemporary evidence establishes HEV as a multifaceted, systemic infection with clinical outcomes governed by the dynamic triad of viral genotype, host immunocompetence, and underlying comorbid conditions. The expanding recognition of EHMs, chronic infection in immunosuppressed populations, and zoonotic transmission in developed nations necessitates a fundamental reconceptualization of disease burden and public health priorities.
Elucidation of mechanisms driving severe acute hepatitis—particularly in pregnancy—and viral persistence in immunocompromised hosts provides critical foundations for risk stratification, early diagnostic algorithms, and personalized therapeutic interventions. The integration of molecular epidemiology, advanced diagnostics, and targeted therapeutics offers transformative potential for reducing HEV-associated morbidity and mortality, especially among vulnerable demographic groups, including gravid women, transplant recipients, and populations in resource-limited settings.
Future research imperatives encompass: (i) longitudinal surveillance of viral molecular evolution and cross-species transmission dynamics; (ii) mechanistic dissection of host-pathogen interactions governing tissue tropism and immune evasion; (iii) discovery and clinical validation of novel therapeutic targets, including direct-acting antivirals and host-directed strategies; (iv) optimization and global deployment of effective vaccines beyond current geographic restrictions; and (v) establishment of integrated, interdisciplinary “One Health” prevention frameworks bridging human, veterinary, and environmental health sectors. Addressing these priorities will be essential for translating scientific advances into tangible reductions in the global burden of hepatitis E.
CFDA: China Food and Drug Administration
EHMs: extrahepatic manifestations
G6PD: glucose-6-phosphate dehydrogenase
HEV: hepatitis E virus
HEV-Ag: hepatitis E virus antigen
HIV: human immunodeficiency virus
HLA: human leukocyte antigen
IgG: immunoglobulin G
IgM: immunoglobulin M
MPGN: membranoproliferative glomerulonephritis
mTOR: mammalian target of rapamycin
RdRp: RNA-dependent RNA polymerase
SOT: solid organ transplant
WHO: World Health Organization
GL: Writing—original draft. EH: Formal analysis. ML: Methodology, Validation. YB: Writing—review & editing. JX: Investigation, Supervision. All authors read and approved the submitted version.
The authors declare that there are no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 301
Download: 29
Times Cited: 0
Hao Xiong, Jinsheng Guo
Laura C. McCoullough ... Peter A. Revill
Chunzheng Li ... Xianguang Yang
Juntian Yao ... Youhua Xie
