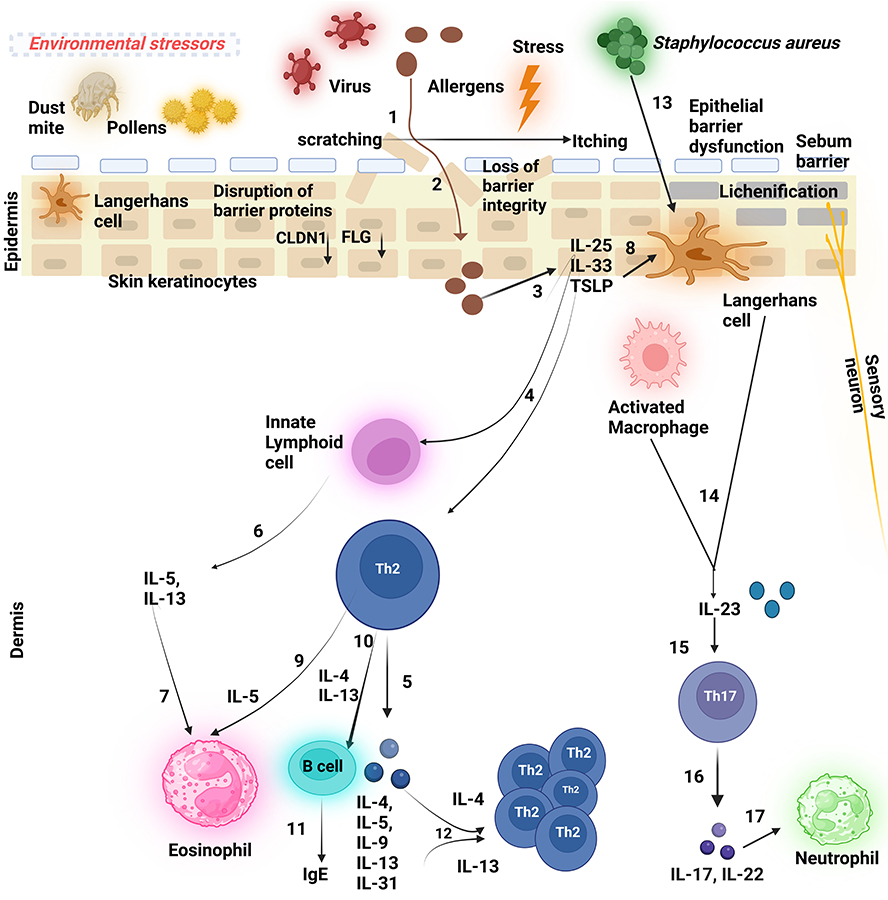
The schematic figure depicts the pathogenesis of atopic dermatitis (AD). (1) A persistent ‘itch-scratch cycle’ occurs due to the disruption of the essential epidermal proteins such as filaggrin (FLG) and claudin 1 (CLDN1) that results in a compromised epidermal barrier, facilitating allergen penetration (2) into the skin and inflicting damage on keratinocytes (KCs), (3) These damaged KCs release ‘alarmins’, interleukin-25 (IL-25), interleukin-33 (IL-33), and thymic stromal lymphopoietin (TSLP), which (4) activate Th2 cells and innate lymphoid cells (ILC2s) at the site of the inflamed lesion, (5) leading to the production of Th2 cytokines (6) ILCs, primarily ILC2s, secrete interleukin-5 (IL-5) and interleukin-13 (IL-13), (7) with IL-5 subsequently attracting eosinophils. Additionally, (8) TSLP triggers the development of Langerhans cells (LCs) (9) which, in turn, promotes Th2 cell activation. (10 and 11) Th2 cells secrete Th2 cytokines such as interleukin-4 (IL-4) and IL-13 that drive B cells to generate immunoglobulin E (IgE), contributing to hypersensitivity type 1 reaction. (12) Th2 cytokines further stimulate Th2 cells in an autocrine manner. (13 and 14) Upon bacterial infection, most commonly by Staphylococcus aureus, LCs rapidly produce interleukin-23 (IL-23) at the site of infection, (15) thereby activating local Th17/ThIL-17 cells. (16) These cells secrete the Th17 cytokines (17) that are potent chemoattractants for neutrophils. Created in BioRender. Baidya, A. (2024). BioRender.com/d04p354
Declarations
Author contributions
AB: Writing—original draft, Writing—review & editing. UM: Validation, Conceptualization, Writing—original draft, Writing—review & editing, Supervision. Both authors read and approved the submitted version.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent to publication
Not applicable.
Availability of data and materials
Not applicable.
Funding
We would like to acknowledge the funds provided by CSIR [MLP137-MISSION LUNG] and DST SERB [GAP-432]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
References
Bhattacharya T, Strom MA, Lio PA. Historical Perspectives on Atopic Dermatitis: Eczema Through the Ages.Pediatr Dermatol. 2016;33:375–9. [DOI] [PubMed]
Kramer ON, Strom MA, Ladizinski B, Lio PA. The history of atopic dermatitis.Clin Dermatol. 2017;35:344–8. [DOI] [PubMed]
Mier. Earliest Description Of The Atopic Syndrome?Br J Dermatol. 1975;92:359. [DOI]
Jaworek A, Wojas-Pelc A. History of atopic dermatitis – a short review from ancient to modern medicine.Dermatol. 2017;104:636–47. [DOI]
Wilson E. Lectures on Dermatology.Br Med J. 1871;1:163–4. [DOI] [PubMed] [PMC]
Rudikoff D, Cohen S, Scheinfeld N. Atopic Dermatitis and Eczematous Disorders. 1st ed. London: CRC Press; 2014. [DOI]
Arents BWM, van Zuuren EJ, Hughes O, Fedorowicz, Z, Flohr, C. Global Report on Atopic Dermatitis 2022. International League of Dermatological Societies; 2022.
Chiricozzi A, Maurelli M, Calabrese L, Peris K, Girolomoni G. Overview of Atopic Dermatitis in Different Ethnic Groups.J Clin Med. 2023;12:2701. [DOI] [PubMed] [PMC]
Girolomoni G, de Bruin-Weller M, Aoki V, Kabashima K, Deleuran M, Puig L, et al. Nomenclature and clinical phenotypes of atopic dermatitis.Ther Adv Chronic Dis. 2021;12:20406223211002979. [DOI] [PubMed] [PMC]
Yew YW, Thyssen JP, Silverberg JI. A systematic review and meta-analysis of the regional and age-related differences in atopic dermatitis clinical characteristics.J Am Acad Dermatol. 2019;80:390–401. [DOI] [PubMed]
Oliveira R, Ferreira J, Azevedo LF, Almeida IF. An Overview of Methods to Characterize Skin Type: Focus on Visual Rating Scales and Self-Report Instruments.Cosmetics. 2023;10:14. [DOI]
Bhattacharya N, Sato WJ, Kelly A, Ganguli-Indra G, Indra AK. Epidermal Lipids: Key Mediators of Atopic Dermatitis Pathogenesis.Trends Mol Med. 2019;25:551–62. [DOI] [PubMed] [PMC]
Paller AS, Spergel JM, Mina-Osorio P, Irvine AD. The atopic march and atopic multimorbidity: Many trajectories, many pathways.J Allergy Clin Immunol. 2019;143:46–55. [DOI] [PubMed]
Suárez-Fariñas M, Dhingra N, Gittler J, Shemer A, Cardinale I, de Guzman Strong C, et al. Intrinsic atopic dermatitis shows similar TH2 and higher TH17 immune activation compared with extrinsic atopic dermatitis.J Allergy Clin Immunol. 2013;132:361–70. [DOI] [PubMed] [PMC]
Werfel T, Allam JP, Biedermann T, Eyerich K, Gilles S, Guttman-Yassky E, et al. Cellular and molecular immunologic mechanisms in patients with atopic dermatitis.J Allergy Clin Immunol. 2016;138:336–49. [DOI] [PubMed]
Gittler JK, Krueger JG, Guttman-Yassky E. Atopic dermatitis results in intrinsic barrier and immune abnormalities: implications for contact dermatitis.J Allergy Clin Immunol. 2013;131:300–13. [DOI] [PubMed] [PMC]
Möbus L, Weidinger S, Emmert H. Epigenetic factors involved in the pathophysiology of inflammatory skin diseases.J Allergy Clin Immunol. 2020;145:1049–60. [DOI] [PubMed]
Weidinger S, Illig T, Baurecht H, Irvine AD, Rodriguez E, Diaz-Lacava A, et al. Loss-of-function variations within the filaggrin gene predispose for atopic dermatitis with allergic sensitizations.J Allergy Clin Immunol. 2006;118:214–9. [DOI] [PubMed]
Clausen ML, Agner T, Thomsen SF. Skin Barrier Dysfunction and the Atopic March.Curr Treat Options Allergy. 2015;2:218–27. [DOI]
Janssens M, van Smeden J, Gooris GS, Bras W, Portale G, Caspers PJ, et al. Increase in short-chain ceramides correlates with an altered lipid organization and decreased barrier function in atopic eczema patients.J Lipid Res. 2012;53:2755–66. [DOI] [PubMed] [PMC]
Li W, Sandhoff R, Kono M, Zerfas P, Hoffmann V, Ding BC, et al. Depletion of ceramides with very long chain fatty acids causes defective skin permeability barrier function, and neonatal lethality in ELOVL4 deficient mice.Int J Biol Sci. 2007;3:120–8. [DOI] [PubMed] [PMC]
Blunder S, Kõks S, Kõks G, Reimann E, Hackl H, Gruber R, et al. Enhanced Expression of Genes Related to Xenobiotic Metabolism in the Skin of Patients with Atopic Dermatitis but Not with Ichthyosis Vulgaris.J Invest Dermatol. 2018;138:98–108. [DOI] [PubMed]
Peroni DG, Bodini A, Corradi M, Coghi A, Boner AL, Piacentini GL. Markers of oxidative stress are increased in exhaled breath condensates of children with atopic dermatitis.Br J Dermatol. 2012;166:839–43. [DOI] [PubMed]
Bhatti JS, Bhatti GK, Reddy PH. Mitochondrial dysfunction and oxidative stress in metabolic disorders — A step towards mitochondria based therapeutic strategies.Biochim Biophys Acta Mol Basis Dis. 2017;1863:1066–77. [DOI] [PubMed] [PMC]
Zorov DB, Juhaszova M, Sollott SJ. Mitochondrial reactive oxygen species (ROS) and ROS-induced ROS release.Physiol Rev. 2014;94:909–50. [DOI] [PubMed] [PMC]
Hamanaka RB, Glasauer A, Hoover P, Yang S, Blatt H, Mullen AR, et al. Mitochondrial reactive oxygen species promote epidermal differentiation and hair follicle development.Sci Signal. 2013;6:ra8. [DOI] [PubMed] [PMC]
Tamari M, Hirota T. Genome-wide association studies of atopic dermatitis.J Dermatol. 2014;41:213–20. [DOI] [PubMed]
Engebretsen KA, Johansen JD, Kezic S, Linneberg A, Thyssen JP. The effect of environmental humidity and temperature on skin barrier function and dermatitis.J Eur Acad Dermatol Venereol. 2016;30:223–49. [DOI] [PubMed]
Guan J, Li Y, Lu F, Feng J. Adipose-derived stem cells ameliorate atopic dermatitis by suppressing the IL-17 expression of Th17 cells in an ovalbumin-induced mouse model.Stem Cell Res Ther. 2022;13:98. [DOI] [PubMed] [PMC]
Pang QQ, Noh BW, Park HS, Kim YS, Kim JH, Cho EJ. Improvement Effect of Membrane-Free Stem Cell Extract on Atopic Dermatitis in NC/Nga Mice.Appl Sci. 2023;13:4542. [DOI]
Leman G, Pavel P, Hermann M, Crumrine D, Elias PM, Minzaghi D, et al. Mitochondrial Activity Is Upregulated in Nonlesional Atopic Dermatitis and Amenable to Therapeutic Intervention.J Invest Dermatol. 2022;142:2623–34.e12. [DOI] [PubMed]
Dudek RP, Ma Z. CAR T Cells for Treating Severe Atopic Allergic Diseases.Dela J Public Health. 2023;9:12–5. [DOI] [PubMed] [PMC]
Nahm DH. Regulatory T Cell-Targeted Immunomodulatory Therapy for Long-Term Clinical Improvement of Atopic Dermatitis: Hypotheses and Perspectives.Life (Basel). 2023;13:1674. [DOI] [PubMed] [PMC]
Tian J, Zhang D, Yang Y, Huang Y, Wang L, Yao X, et al. 2023. Global epidemiology of atopic dermatitis: a comprehensive systematic analysis and modelling study.British Journal of Dermatology. 2024;190:55–61. [DOI]
Katoh N, Saeki H, Kataoka Y, Etoh T, Teramukai S, Takagi H, et al.; ADDRESS-J Investigators. Atopic dermatitis disease registry in Japanese adult patients with moderate to severe atopic dermatitis (ADDRESS-J): Baseline characteristics, treatment history and disease burden.J Dermatol. 2019;46:290–300. [DOI] [PubMed] [PMC]
Piipponen M, Li D, Landén NX. The Immune Functions of Keratinocytes in Skin Wound Healing.Int J Mol Sci. 2020;21:8790. [DOI] [PubMed] [PMC]
Çetinarslan T, Kümper L, Fölster-Holst R. The immunological and structural epidermal barrier dysfunction and skin microbiome in atopic dermatitis-an update.Front Mol Biosci. 2023;10:1159404. [DOI] [PubMed] [PMC]
Nguyen HLT, Trujillo-Paez JV, Umehara Y, Yue H, Peng G, Kiatsurayanon C, et al. Role of Antimicrobial Peptides in Skin Barrier Repair in Individuals with Atopic Dermatitis.Int J Mol Sci. 2020;21:7607. [DOI] [PubMed] [PMC]
Akiyama T, Niyonsaba F, Kiatsurayanon C, Nguyen TT, Ushio H, Fujimura T, et al. The human cathelicidin LL-37 host defense peptide upregulates tight junction-related proteins and increases human epidermal keratinocyte barrier function.J Innate Immun. 2014;6:739–53. [DOI] [PubMed] [PMC]
Goto H, Hongo M, Ohshima H, Kurasawa M, Hirakawa S, Kitajima Y. Human beta defensin-1 regulates the development of tight junctions in cultured human epidermal keratinocytes.J Dermatol Sci. 2013;71:145–8. [DOI] [PubMed]
Kiatsurayanon C, Niyonsaba F, Smithrithee R, Akiyama T, Ushio H, Hara M, et al. Host defense (Antimicrobial) peptide, human β-defensin-3, improves the function of the epithelial tight-junction barrier in human keratinocytes.J Invest Dermatol. 2014;134:2163–73. [DOI] [PubMed]
Hattori F, Kiatsurayanon C, Okumura K, Ogawa H, Ikeda S, Okamoto K, et al. The antimicrobial protein S100A7/psoriasin enhances the expression of keratinocyte differentiation markers and strengthens the skin’s tight junction barrier.Br J Dermatol. 2014;171:742–53. [DOI] [PubMed]
Sandilands A, Sutherland C, Irvine AD, McLean WH. Filaggrin in the frontline: role in skin barrier function and disease.J Cell Sci. 2009;122:1285–94. [DOI] [PubMed] [PMC]
Quiroz FG, Fiore VF, Levorse J, Polak L, Wong E, Pasolli HA, et al. Liquid-liquid phase separation drives skin barrier formation.Science. 2020;367:eaax9554. [DOI] [PubMed] [PMC]
Kim BS, Siracusa MC, Saenz SA, Noti M, Monticelli LA, Sonnenberg GF, et al. TSLP elicits IL-33-independent innate lymphoid cell responses to promote skin inflammation.Sci Transl Med. 2013;5:170ra16. [DOI] [PubMed] [PMC]
Kubo A, Nagao K, Yokouchi M, Sasaki H, Amagai M. External antigen uptake by Langerhans cells with reorganization of epidermal tight junction barriers.J Exp Med. 2009;206:2937–46. [DOI] [PubMed] [PMC]
Morita K, Miyachi Y, Furuse M. Tight junctions in epidermis: from barrier to keratinization.Eur J Dermatol. 2011;21:12–7. [DOI] [PubMed]
Egawa G, Kabashima K. Barrier dysfunction in the skin allergy.Allergol Int. 2018;67:3–11. [DOI] [PubMed]
Leyvraz C, Charles RP, Rubera I, Guitard M, Rotman S, Breiden B, et al. The epidermal barrier function is dependent on the serine protease CAP1/Prss8.J Cell Biol. 2005;170:487–96. [DOI] [PubMed] [PMC]
Matsui T, Miyamoto K, Kubo A, Kawasaki H, Ebihara T, Hata K, et al. SASPase regulates stratum corneum hydration through profilaggrin-to-filaggrin processing.EMBO Mol Med. 2011;3:320–33. [DOI] [PubMed] [PMC]
Nachat R, Méchin MC, Takahara H, Chavanas S, Charveron M, Serre G, et al. Peptidylarginine deiminase isoforms 1-3 are expressed in the epidermis and involved in the deimination of K1 and filaggrin.J Invest Dermatol. 2005;124:384–93. [DOI] [PubMed]
Hoste E, Kemperman P, Devos M, Denecker G, Kezic S, Yau N, et al. Caspase-14 is required for filaggrin degradation to natural moisturizing factors in the skin.J Invest Dermatol. 2011;131:2233–41. [DOI] [PubMed]
Leitch CS, Natafji E, Yu C, Abdul-Ghaffar S, Madarasingha N, Venables ZC, et al. Filaggrin-null mutations are associated with increased maturation markers on Langerhans cells.J Allergy Clin Immunol. 2016;138:482–90.e7. [DOI] [PubMed] [PMC]
Kawasaki H, Nagao K, Kubo A, Hata T, Shimizu A, Mizuno H, et al. Altered stratum corneum barrier and enhanced percutaneous immune responses in filaggrin-null mice.J Allergy Clin Immunol. 2012;129:1538–46.e6. [DOI] [PubMed]
Saunders SP, Moran T, Floudas A, Wurlod F, Kaszlikowska A, Salimi M, et al. Spontaneous atopic dermatitis is mediated by innate immunity, with the secondary lung inflammation of the atopic march requiring adaptive immunity.J Allergy Clin Immunol. 2016;137:482–91. [DOI] [PubMed] [PMC]
Wan J, Mitra N, Hoffstad OJ, Yan AC, Margolis DJ. Longitudinal atopic dermatitis control and persistence vary with timing of disease onset in children: A cohort study.J Am Acad Dermatol. 2019;81:1292–99. [DOI] [PubMed] [PMC]
Miraglia del Giudice M, Decimo F, Leonardi S, Maioello N, Amelio R, Capasso A, et al. Immune dysregulation in atopic dermatitis.Allergy Asthma Proc. 2006;27:451–5. [DOI] [PubMed]
Tokura Y. Extrinsic and intrinsic types of atopic dermatitis.J Dermatol Sci. 2010;58:1–7. [DOI] [PubMed]
Park JH, Choi YL, Namkung JH, Kim WS, Lee JH, Park HJ, et al. Characteristics of extrinsic vs. intrinsic atopic dermatitis in infancy: correlations with laboratory variables.Br J Dermatol. 2006;155:778–83. [DOI] [PubMed]
Liu L, Song G, Song Z. Intrinsic Atopic Dermatitis and Extrinsic Atopic Dermatitis: Similarities and Differences.Clin Cosmet Investig Dermatol. 2022;15:2621–8. [DOI]
Wang IJ, Hsieh WS, Guo YL, Jee SH, Hsieh CJ, Hwang YH, et al. Neuro-mediators as predictors of paediatric atopic dermatitis.Clin Exp Allergy. 2008;38:1302–8. [DOI] [PubMed]
Howell MD, Boguniewicz M, Pastore S, Novak N, Bieber T, Girolomoni G, et al. Mechanism of HBD-3 deficiency in atopic dermatitis.Clin Immunol. 2006;121:332–8. [DOI] [PubMed]
Raap U, Werfel T, Goltz C, Deneka N, Langer K, Bruder M, et al. Circulating levels of brain-derived neurotrophic factor correlate with disease severity in the intrinsic type of atopic dermatitis.Allergy. 2006;61:1416–8. [DOI] [PubMed]
Wang SP, Stefanovic N, Orfali RL, Aoki V, Brown SJ, Dhar S, et al. Impact of climate change on atopic dermatitis: A review by the International Eczema Council.Allergy. 2024;79:1455–69. [DOI] [PubMed]
Huang HJ, Sarzsinszky E, Vrtala S. House dust mite allergy: The importance of house dust mite allergens for diagnosis and immunotherapy.Mol Immunol. 2023;158:54–67. [DOI] [PubMed]
Tong SY, Davis JS, Eichenberger E, Holland TL, Fowler VG Jr. Staphylococcus aureus Infections: Epidemiology, Pathophysiology, Clinical Manifestations, and Management.Clin Microbiol Rev. 2015;28:603–61. [DOI] [PubMed] [PMC]
Tyurin YA, Shamsutdinov AF, Kalinin NN, Sharifullina AA, Reshetnikova ID. Association of Toll-Like Cell Receptors TLR2 (p.Arg753GLN) and TLR4 (p.Asp299GLY) Polymorphisms with Indicators of General and Local Immunity in Patients with Atopic Dermatitis.J Immunol Res. 2017;2017:8493545. [DOI] [PubMed] [PMC]
Bantel H, Sinha B, Domschke W, Peters G, Schulze-Osthoff K, Jänicke RU. α-Toxin is a mediator of Staphylococcus aureus-induced cell death and activates caspases via the intrinsic death pathway independently of death receptor signaling.J Cell Biol. 2001;155:637–48. [DOI] [PubMed] [PMC]
Ezepchuk YV, Leung DY, Middleton MH, Bina P, Reiser R, Norris DA. Staphylococcal Toxins and Protein A Differentially Induce Cytotoxicity and Release of Tumor Necrosis Factor-α From Human Keratinocytes.J Invest Dermatol. 1996;107:603–9. [DOI] [PubMed]
Kim KH, Han JH, Chung JH, Cho KH, Eun HC. Role of staphylococcal superantigen in atopic dermatitis: influence on keratinocytes.J Korean Med Sci. 2006;21:315–23. [DOI] [PubMed] [PMC]
Damour A, Robin B, Deroche L, Broutin L, Bellin N, Verdon J, et al. Phenol-soluble modulins α are major virulence factors of Staphylococcus aureus secretome promoting inflammatory response in human epidermis.Virulence. 2021;12:2474–92. [DOI] [PubMed] [PMC]
Syed AK, Reed TJ, Clark KL, Boles BR, Kahlenberg JM. Staphlyococcus aureus phenol-soluble modulins stimulate the release of proinflammatory cytokines from keratinocytes and are required for induction of skin inflammation.Infect Immun. 2015;83:3428–37. [DOI] [PubMed] [PMC]
Chi CY, Lin CC, Liao IC, Yao YC, Shen FC, Liu CC, et al. Panton-Valentine leukocidin facilitates the escape of Staphylococcus aureus from human keratinocyte endosomes and induces apoptosis.J Infect Dis. 2014;209:224–35. [DOI] [PubMed]
Mariutti RB, Tartaglia NR, Seyffert N, Castro TLP, Arni RK, Azevedo VA, et al. Exfoliative Toxins of Staphylococcus Aureus. In: Enany S, Crotty Alexander LE, editors. The Rise of Virulence and Antibiotic Resistance in Staphylococcus Aureus. London: InTech; 2017. [DOI]
Hanakawa Y, Selwood T, Woo D, Lin C, Schechter NM, Stanley JR. Calcium-dependent conformation of desmoglein 1 is required for its cleavage by exfoliative toxin.J Invest Dermatol. 2003;121:383–9. [DOI] [PubMed]
Williams MR, Nakatsuji T, Sanford JA, Vrbanac AF, Gallo RL. Staphylococcus aureus Induces Increased Serine Protease Activity in Keratinocytes.J Invest Dermatol. 2017;137:377–84. [DOI] [PubMed] [PMC]
Sugaya M. The Role of Th17-Related Cytokines in Atopic Dermatitis.Int J Mol Sci. 2020;21:1314. [DOI] [PubMed] [PMC]
Liu T, Li S, Ying S, Tang S, Ding Y, Li Y, et al. The IL-23/IL-17 Pathway in Inflammatory Skin Diseases: From Bench to Bedside.Front Immunol. 2020;11:594735. [DOI] [PubMed] [PMC]
Traidl S, Roesner L, Zeitvogel J, Werfel T. Eczema herpeticum in atopic dermatitis.Allergy. 2021;76:3017–27. [DOI] [PubMed]
Courtney A, Su JC. The Psychology of Atopic Dermatitis.J Clin Med. 2024;13:1602. [DOI] [PubMed] [PMC]
Kim BE, Hui-Beckman J, Lyubchenko T, Hall CF, Fallahi S, Brull A, et al. Transient receptor potential vanilloid 1 plays a major role in low temperature-mediated skin barrier dysfunction.J Allergy Clin Immunol. 2022;150:362–72.e7. [DOI] [PubMed]
Rueter K, Jones AP, Siafarikas A, Lim EM, Bear N, Noakes PS, et al. Direct infant UV light exposure is associated with eczema and immune development.J Allergy Clin Immunol. 2019;143:1012–20.e2. [DOI] [PubMed]
Ferrara F, Pambianchi E, Woodby B, Messano N, Therrien JP, Pecorelli A, et al. Evaluating the effect of ozone in UV induced skin damage.Toxicol Lett. 2021;338:40–50. [DOI] [PubMed]
Hendricks AJ, Eichenfield LF, Shi VY. The impact of airborne pollution on atopic dermatitis: a literature review.Br J Dermatol. 2020;183:16–23. [DOI] [PubMed]
Pan Z, Dai Y, Akar-Ghibril N, Simpson J, Ren H, Zhang L, et al. Impact of Air Pollution on Atopic Dermatitis: A Comprehensive Review.Clin Rev Allergy Immunol. 2023;65:121–35. [DOI] [PubMed]
Green M, Kashetsky N, Feschuk A, Maibach HI. Transepidermal water loss (TEWL): Environment and pollution-A systematic review.Skin Health Dis. 2022;2:e104. [DOI] [PubMed] [PMC]
Kim BE, Kim J, Goleva E, Berdyshev E, Lee J, Vang KA, et al. Particulate matter causes skin barrier dysfunction.JCI Insight. 2021;6:e145185. [DOI] [PubMed] [PMC]
Chao L, Feng B, Liang H, Zhao X, Song J. Particulate matter and inflammatory skin diseases: From epidemiological and mechanistic studies.Sci Total Environ. 2023;905:167111. [DOI] [PubMed]
Dijkhoff IM, Drasler B, Karakocak BB, Petri-Fink A, Valacchi G, Eeman M, et al. Impact of airborne particulate matter on skin: a systematic review from epidemiology to in vitro studies.Part Fibre Toxicol. 2020;17:35. [DOI] [PubMed] [PMC]
Piao MJ, Ahn MJ, Kang KA, Ryu YS, Hyun YJ, Shilnikova K, et al. Particulate matter 2.5 damages skin cells by inducing oxidative stress, subcellular organelle dysfunction, and apoptosis.Arch Toxicol. 2018;92:2077–91. [DOI] [PubMed] [PMC]
Park SY, Byun EJ, Lee JD, Kim S, Kim HS. Air Pollution, Autophagy, and Skin Aging: Impact of Particulate Matter (PM10) on Human Dermal Fibroblasts.Int J Mol Sci. 2018;19:2727. [DOI] [PubMed] [PMC]
Wang Z, Zhang M. Smoking and the risk of atopic dermatitis: A two-sample mendelian randomization study.Medicine (Baltimore). 2023;102:e36050. [DOI] [PubMed] [PMC]
Xu C, Bailly-Maitre B, Reed JC. Endoplasmic reticulum stress: cell life and death decisions.J Clin Invest. 2005;115:2656–64. [DOI] [PubMed] [PMC]
Akhtar S, Alsayed RKME, Ahmad F, AlHammadi A, Al-Khawaga S, AlHarami SMAM, et al. Epigenetic control of inflammation in Atopic Dermatitis.Semin Cell Dev Biol. 2024;154:199–207. [DOI] [PubMed]
Kim JE, Kim JS, Cho DH, Park HJ. Molecular Mechanisms of Cutaneous Inflammatory Disorder: Atopic Dermatitis.Int J Mol Sci. 2016;17:1234. [DOI] [PubMed] [PMC]
Surace AEA, Hedrich CM. The Role of Epigenetics in Autoimmune/Inflammatory Disease.Front Immunol. 2019;10:1525. [DOI] [PubMed] [PMC]
Olisova OY, Kochergin NG, Kayumova LN, Zavarykina TM, Dmitriev AA, Asanov AY. Skin DNA methylation profile in atopic dermatitis patients: A case-control study.Exp Dermatol. 2020;29:184–9. [DOI] [PubMed]
Schmidt AD, de Guzman Strong C. Current understanding of epigenetics in atopic dermatitis.Exp Dermatol. 2021;30:1150–5. [DOI] [PubMed] [PMC]
Rodríguez E, Baurecht H, Wahn AF, Kretschmer A, Hotze M, Zeilinger S, et al. An integrated epigenetic and transcriptomic analysis reveals distinct tissue-specific patterns of DNA methylation associated with atopic dermatitis.J Invest Dermatol. 2014;134:1873–83. [DOI] [PubMed]
Nedoszytko B, Reszka E, Gutowska-Owsiak D, Trzeciak M, Lange M, Jarczak J, et al. Genetic and Epigenetic Aspects of Atopic Dermatitis.Int J Mol Sci. 2020;21:6484. [DOI] [PubMed] [PMC]
Tay SS, Roediger B, Tong PL, Tikoo S, Weninger W. The Skin-Resident Immune Network.Curr Dermatol Rep. 2013;3:13–22. [DOI] [PubMed] [PMC]
Weninger W, Biro M, Jain R. Leukocyte migration in the interstitial space of non-lymphoid organs.Nat Rev Immunol. 2014;14:232–46. [DOI] [PubMed]
Wan YY. Multi‐tasking of Helper T Cells.Immunology. 2010;130:166–71. [DOI]
Grewe M, Bruijnzeel-Koomen CA, Schöpf E, Thepen T, Langeveld-Wildschut AG, Ruzicka T, et al. A role for Th1 and Th2 cells in the immunopathogenesis of atopic dermatitis.Immunol Today. 1998;19:359–61. [DOI] [PubMed]
Hamid Q, Naseer T, Minshall EM, Song YL, Boguniewicz M, Leung DY. In vivo expression of IL-12 and IL-13 in atopic dermatitis.J Allergy Clin Immunol. 1996;98:225–31. [DOI] [PubMed]
Koga C, Kabashima K, Shiraishi N, Kobayashi M, Tokura Y. Possible pathogenic role of Th17 cells for atopic dermatitis.J Invest Dermatol. 2008;128:2625–30. [DOI] [PubMed]
Teunissen MB, Koomen CW, de Waal Malefyt R, Wierenga EA, Bos JD. Interleukin-17 and interferon-gamma synergize in the enhancement of proinflammatory cytokine production by human keratinocytes.J Invest Dermatol. 1998;111:645–9. [DOI] [PubMed]
Kolls JK, Lindén A. Interleukin-17 family members and inflammation.Immunity. 2004;21:467–76. [DOI] [PubMed]
Ito Y, Adachi Y, Makino T, Higashiyama H, Fuchizawa T, Shimizu T, et al. Expansion of FOXP3-positive CD4+CD25+ T cells associated with disease activity in atopic dermatitis.Ann Allergy Asthma Immunol. 2009;103:160–5. [DOI] [PubMed]
Samochocki Z, Alifier M, Bodera P, Jeziorkowska R, Rosiak E, Jurkiewicz B, et al. T-regulatory cells in severe atopic dermatitis: alterations related to cytokines and other lymphocyte subpopulations.Arch Dermatol Res. 2012;304:795–801. [DOI] [PubMed] [PMC]
Szegedi A, Baráth S, Nagy G, Szodoray P, Gál M, Sipka S, et al. Regulatory T cells in atopic dermatitis: epidermal dendritic cell clusters may contribute to their local expansion.Br J Dermatol. 2009;160:984–93. [DOI] [PubMed]
Ou LS, Goleva E, Hall C, Leung DY. T regulatory cells in atopic dermatitis and subversion of their activity by superantigens.J Allergy Clin Immunol. 2004;113:756–63. [DOI] [PubMed]
Roediger B, Kyle R, Le Gros G, Weninger W. Dermal group 2 innate lymphoid cells in atopic dermatitis and allergy.Curr Opin Immunol. 2014;31:108–14. [DOI] [PubMed]
Jia H, Wan H, Zhang D. Innate lymphoid cells: a new key player in atopic dermatitis.Frontiers in Immunology. 2023;14:1277120. [DOI]
Salimi M, Barlow JL, Saunders SP, Xue L, Gutowska-Owsiak D, Wang X, et al. A role for IL-25 and IL-33-driven type-2 innate lymphoid cells in atopic dermatitis.J Exp Med. 2013;210:2939–50. [DOI] [PubMed] [PMC]
Roediger B, Kyle R, Yip KH, Sumaria N, Guy TV, Kim BS, et al. Cutaneous immunosurveillance and regulation of inflammation by group 2 innate lymphoid cells.Nat Immunol. 2013;14:564–73. [DOI] [PubMed] [PMC]
Monticelli LA, Sonnenberg GF, Artis D. Innate lymphoid cells: critical regulators of allergic inflammation and tissue repair in the lung.Curr Opin Immunol. 2012;24:284–9. [DOI] [PubMed] [PMC]
Johnson-Huang LM, McNutt NS, Krueger JG, Lowes MA. Cytokine-producing dendritic cells in the pathogenesis of inflammatory skin diseases.J Clin Immunol. 2009;29:247–56. [DOI] [PubMed] [PMC]
Nakajima S, Igyártó BZ, Honda T, Egawa G, Otsuka A, Hara-Chikuma M, et al. Langerhans cells are critical in epicutaneous sensitization with protein antigen via thymic stromal lymphopoietin receptor signaling.J Allergy Clin Immunol. 2012;129:1048–55.e6. [DOI] [PubMed] [PMC]
Elentner A, Finke D, Schmuth M, Chappaz S, Ebner S, Malissen B, et al. Langerhans cells are critical in the development of atopic dermatitis-like inflammation and symptoms in mice.J Cell Mol Med. 2009;13:2658–72. [DOI] [PubMed] [PMC]
Wollenberg A, Wagner M, Günther S, Towarowski A, Tuma E, Moderer M, et al. Plasmacytoid dendritic cells: a new cutaneous dendritic cell subset with distinct role in inflammatory skin diseases.J Invest Dermatol. 2002;119:1096–2. [DOI] [PubMed]
Hossny E, Aboul-Magd M, Bakr S. Increased plasma eotaxin in atopic dermatitis and acute urticaria in infants and children.Allergy. 2001;56:996–1002. [DOI] [PubMed]
Kay AB, Barata L, Meng Q, Durham SR, Ying S. Eosinophils and eosinophil-associated cytokines in allergic inflammation.Int Arch Allergy Immunol. 1997;113:196–9. [DOI] [PubMed]
Imai Y, Yasuda K, Sakaguchi Y, Haneda T, Mizutani H, Yoshimoto T, et al. Skin-specific expression of IL-33 activates group 2 innate lymphoid cells and elicits atopic dermatitis-like inflammation in mice.Proc Natl Acad Sci U S A. 2013;110:13921–6. [DOI] [PubMed] [PMC]
Soter NA. Morphology of atopic eczema.Allergy. 1989;44:16–9. [DOI]
Irani AM, Sampson HA, Schwartz LB. Mast cells in atopic dermatitis.Allergy. 1989;44:31–4. [PubMed]
Ring J, Thomas P. Histamine and atopic eczema.Acta Derm Venereol Suppl (Stockh). 1989;144:70–7. [DOI] [PubMed]
Obara W, Kawa Y, Ra C, Nishioka K, Soma Y, Mizoguchi M. T cells and mast cells as a major source of interleukin-13 in atopic dermatitis.Dermatology. 2002;205:11–7. [DOI] [PubMed]
Horsmanheimo L, Harvima IT, Järvikallio A, Harvima RJ, Naukkarinen A, Horsmanheimo M. Mast cells are one major source of interleukin-4 in atopic dermatitis.Br J Dermatol. 1994;131:348–53. [DOI] [PubMed]
Spergel JM, Mizoguchi E, Oettgen H, Bhan AK, Geha RS. Roles of TH1 and TH2 cytokines in a murine model of allergic dermatitis.J Clin Invest. 1999;103:1103–11. [DOI] [PubMed] [PMC]
Groneberg DA, Bester C, Grützkau A, Serowka F, Fischer A, Henz BM, et al. Mast cells and vasculature in atopic dermatitis--potential stimulus of neoangiogenesis.Allergy. 2005;60:90–7. [DOI] [PubMed]
Al-Shobaili HA, Ahmed AA, Alnomair N, Alobead ZA, Rasheed Z. Molecular Genetic of Atopic dermatitis: An Update.Int J Health Sci (Qassim). 2016;10:96–120. [PubMed] [PMC]
Badertscher K, Brönnimann M, Karlen S, Braathen LR, Yawalkar N. Mast cell chymase is increased in chronic atopic dermatitis but not in psoriasis.Arch Dermatol Res. 2005;296:503–6. [DOI] [PubMed]
Mao XQ, Shirakawa T, Yoshikawa T, Yoshikawa K, Kawai M, Sasaki S, et al. Association between genetic variants of mast-cell chymase and eczema.Lancet. 1996;348:581–3. [DOI] [PubMed]
Bratu D, Boda D, Caruntu C. Genomic, Epigenomic, Transcriptomic, Proteomic and Metabolomic Approaches in Atopic Dermatitis.Curr Issues Mol Biol. 2023;45:5215–31. [DOI] [PubMed] [PMC]
Sroka-Tomaszewska J, Trzeciak M. Molecular Mechanisms of Atopic Dermatitis Pathogenesis.Int J Mol Sci. 2021;22:4130. [DOI] [PubMed] [PMC]
Egawa G, Wolfgang W. Pathogenesis of atopic dermatitis: A short review.Cogent Biology. 2015;1:1103459. [DOI]
Palmer CN, Irvine AD, Terron-Kwiatkowski A, Zhao Y, Liao H, Lee SP, et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis.Nat Genet. 2006;38:441–6. [DOI] [PubMed]
Smith FJ, Irvine AD, Terron-Kwiatkowski A, Sandilands A, Campbell LE, Zhao Y, et al. Loss-of-function mutations in the gene encoding filaggrin cause ichthyosis vulgaris.Nat Genet. 2006;38:337–42. [DOI] [PubMed]
Irvine AD, McLean WH, Leung DY. Filaggrin mutations associated with skin and allergic diseases.N Engl J Med. 2011;365:1315–27. [DOI] [PubMed]
McAleer MA, Irvine AD. The multifunctional role of filaggrin in allergic skin disease.J Allergy Clin Immunol. 2013;131:280–91. [DOI] [PubMed]
Park KD, Pak SC, Park KK. The Pathogenetic Effect of Natural and Bacterial Toxins on Atopic Dermatitis.Toxins (Basel). 2016;9:3. [DOI] [PubMed] [PMC]
Sahle FF, Gebre-Mariam T, Dobner B, Wohlrab J, Neubert RH. Skin diseases associated with the depletion of stratum corneum lipids and stratum corneum lipid substitution therapy.Skin Pharmacol Physiol. 2015;28:42–55. [DOI] [PubMed]
Kahraman E, Melis K, Şahin Bektay H, Güngör S. Recent Advances on Topical Application of Ceramides to Restore Barrier Function of Skin.Cosmetics. 2019;6:52. [DOI]
Wickett RR, Visscher MO. Structure and function of the epidermal barrier.Am J Infect Control. 2006;34:S98–110. [DOI]
Lee AY. Molecular Mechanism of Epidermal Barrier Dysfunction as Primary Abnormalities.Int J Mol Sci. 2020;21:1194. [DOI] [PubMed] [PMC]
Vávrová K, Kováčik A, Opálka L. Ceramides in the Skin Barrier.Eur J Pharm. 2017;64:28–35. [DOI]
Murphy B, Grimshaw S, Hoptroff M, Paterson S, Arnold D, Cawley A, et al. Alteration of barrier properties, stratum corneum ceramides and microbiome composition in response to lotion application on cosmetic dry skin.Sci Rep. 2022;12:5223. [DOI] [PubMed] [PMC]
Fujii M. The Pathogenic and Therapeutic Implications of Ceramide Abnormalities in Atopic Dermatitis.Cells. 2021;10:2386. [DOI] [PubMed] [PMC]
Lampe MA, Burlingame AL, Whitney J, Williams ML, Brown BE, Roitman E, et al. Human stratum corneum lipids: characterization and regional variations.J Lipid Res. 1983;24:120–30. [PubMed]
Imokawa G, Abe A, Jin K, Higaki Y, Kawashima M, Hidano A. Decreased level of ceramides in stratum corneum of atopic dermatitis: an etiologic factor in atopic dry skin?J Invest Dermatol. 1991;96:523–6. [DOI] [PubMed]
Cui CY, Kusuda S, Seguchi T, Takahashi M, Aisu K, Tezuka T. Decreased level of prosaposin in atopic skin.J Invest Dermatol. 1997;109:319–23. [DOI] [PubMed]
Jin K, Higaki Y, Takagi Y, Higuchi K, Yada Y, Kawashima M, et al. Analysis of beta-glucocerebrosidase and ceramidase activities in atopic and aged dry skin.Acta Derm Venereol. 1994;74:337–40. [DOI] [PubMed]
Boer DEC, van Smeden J, Al-Khakany H, Melnik E, van Dijk R, Absalah S, et al. Skin of atopic dermatitis patients shows disturbed β-glucocerebrosidase and acid sphingomyelinase activity that relates to changes in stratum corneum lipid composition.Biochim Biophys Acta Mol Cell Biol Lipids. 2020;1865:158673. [DOI] [PubMed]
Berdyshev E, Goleva E, Bronova I, Dyjack N, Rios C, Jung J, et al. Lipid abnormalities in atopic skin are driven by type 2 cytokines.JCI Insight. 2018;3:e98006. [DOI] [PubMed] [PMC]
Beck LA, Cork MJ, Amagai M, Benedetto A, Kabashima K, Hamilton JD, et al. Type 2 Inflammation Contributes to Skin Barrier Dysfunction in Atopic Dermatitis.JID Innov. 2022;2:100131. [DOI] [PubMed] [PMC]
Berdyshev E, Goleva E, Bissonnette R, Bronova I, Bronoff AS, Richers BN, et al. Dupilumab significantly improves skin barrier function in patients with moderate-to-severe atopic dermatitis.Allergy. 2022;77:3388–97. [DOI] [PubMed]
Hatano Y, Terashi H, Arakawa S, Katagiri K. Interleukin-4 suppresses the enhancement of ceramide synthesis and cutaneous permeability barrier functions induced by tumor necrosis factor-alpha and interferon-gamma in human epidermis.J Invest Dermatol. 2005;124:786–92. [DOI] [PubMed]
Upadhyay PR, Seminario-Vidal L, Abe B, Ghobadi C, Sims JT. Cytokines and Epidermal Lipid Abnormalities in Atopic Dermatitis: A Systematic Review.Cells. 2023;12:2793. [DOI] [PubMed] [PMC]
Pareek A, Kumari L, Pareek A, Chaudhary S, Ratan Y, Janmeda P, et al. Unraveling Atopic Dermatitis: Insights into Pathophysiology, Therapeutic Advances, and Future Perspectives.Cells. 2024;13:425. [DOI] [PubMed] [PMC]
Sawada E, Yoshida N, Sugiura A, Imokawa G. Th1 cytokines accentuate but Th2 cytokines attenuate ceramide production in the stratum corneum of human epidermal equivalents: an implication for the disrupted barrier mechanism in atopic dermatitis.J Dermatol Sci. 2012;68:25–35. [DOI] [PubMed]
Nickoloff BJ, Naidu Y. Perturbation of epidermal barrier function correlates with initiation of cytokine cascade in human skin.J Am Acad Dermatol. 1994;30:535–46. [DOI] [PubMed]
Del Rosso JQ. Repair and maintenance of the epidermal barrier in patients diagnosed with atopic dermatitis: an evaluation of the components of a body wash-moisturizer skin care regimen directed at management of atopic skin.J Clin Aesthet Dermatol. 2011;4:45–55. [PubMed] [PMC]
Nakajima K, Terao M, Takaishi M, Kataoka S, Goto-Inoue N, Setou M, et al. Barrier abnormality due to ceramide deficiency leads to psoriasiform inflammation in a mouse model.J Invest Dermatol. 2013;133:2555–65. [DOI] [PubMed]
Kurahashi R, Hatano Y, Katagiri K. IL-4 suppresses the recovery of cutaneous permeability barrier functions in vivo.J Invest Dermatol. 2008;128:1329–31. [DOI] [PubMed]
Park YH, Jang WH, Seo JA, Park M, Lee TR, Park Y, et al. Decrease of ceramides with very long-chain fatty acids and downregulation of elongases in a murine atopic dermatitis model.J Invest Dermatol. 2012;132:476–9. [DOI] [PubMed]
Danso MO, van Drongelen V, Mulder A, van Esch J, Scott H, van Smeden J, et al. TNF-α and Th2 cytokines induce atopic dermatitis-like features on epidermal differentiation proteins and stratum corneum lipids in human skin equivalents.J Invest Dermatol. 2014;134:1941–50. [DOI] [PubMed]
Danso M, Boiten W, van Drongelen V, Gmelig Meijling K, Gooris G, EI Ghalbzouri A, et al. Altered expression of epidermal lipid bio-synthesis enzymes in atopic dermatitis skin is accompanied by changes in stratum corneum lipid composition.J Dermatol Sci. 2017;88:57–66. [DOI] [PubMed]
Cork MJ, Danby SG, Vasilopoulos Y, Hadgraft J, Lane ME, Moustafa M, et al. Epidermal barrier dysfunction in atopic dermatitis.J Invest Dermatol. 2009;129:1892–908. [DOI] [PubMed]
Moffatt MF. SPINK5: a gene for atopic dermatitis and asthma.Clin Exp Allergy. 2004;34:325–7. [DOI] [PubMed]
Nemeth V, Syed HA, Evans J. Eczema. Eczema. Treasure Island (FL): StatPearls Publishing; 2024. [PubMed]
Ansotegui IJ, Melioli G, Canonica GW, Caraballo L, Villa E, Ebisawa M, et al. IgE allergy diagnostics and other relevant tests in allergy, a World Allergy Organization position paper.World Allergy Organ J. 2020;13:100080. [DOI] [PubMed] [PMC]
Chiriac AE, Popescu R, Butnariu L, Murgu A, Foia L, Azoicai D. Mutations of filament-aggregating protein gene in Romanian children diagnosed with atopic dermatitis.Exp Ther Med. 2020;20:212. [DOI] [PubMed] [PMC]
Kim BE, Goleva E, Kim PS, Norquest K, Bronchick C, Taylor P, et al. Side-by-Side Comparison of Skin Biopsies and Skin Tape Stripping Highlights Abnormal Stratum Corneum in Atopic Dermatitis.J Invest Dermatol. 2019;139:2387–9.e1. [DOI] [PubMed] [PMC]
Leung DY, Guttman-Yassky E. Deciphering the complexities of atopic dermatitis: shifting paradigms in treatment approaches.J Allergy Clin Immunol. 2014;134:769–79. [DOI] [PubMed] [PMC]
Purnamawati S, Indrastuti N, Danarti R, Saefudin T. The Role of Moisturizers in Addressing Various Kinds of Dermatitis: A Review.Clin Med Res. 2017;15:75–87. [DOI] [PubMed] [PMC]
Myles IA, Williams KW, Reckhow JD, Jammeh ML, Pincus NB, Sastalla I, et al. Transplantation of human skin microbiota in models of atopic dermatitis.JCI Insight. 2016;1:e86955. [DOI] [PubMed] [PMC]
Myles IA, Castillo CR, Barbian KD, Kanakabandi K, Virtaneva K, Fitzmeyer E, et al. Therapeutic responses to Roseomonas mucosa in atopic dermatitis may involve lipid-mediated TNF-related epithelial repair.Sci Transl Med. 2020;12:eaaz8631. [DOI] [PubMed] [PMC]
Nakatsuji T, Hata TR, Tong Y, Cheng JY, Shafiq F, Butcher AM, et al. Development of a human skin commensal microbe for bacteriotherapy of atopic dermatitis and use in a phase 1 randomized clinical trial.Nat Med. 2021;27:700–9. [DOI] [PubMed] [PMC]
Weiss A, Delavenne E, Matias C, Lagler H, Simon D, Li P, et al. Topical niclosamide (ATx201) reduces Staphylococcus aureus colonization and increases Shannon diversity of the skin microbiome in atopic dermatitis patients in a randomized, double-blind, placebo-controlled Phase 2 trial.Clin Transl Med. 2022;12:e790. [DOI] [PubMed] [PMC]
Bieber T. Atopic dermatitis: an expanding therapeutic pipeline for a complex disease.Nat Rev Drug Discov. 2022;21:21–40. [DOI] [PubMed] [PMC]
Cully M. Microbiome therapeutics go small molecule.Nat Rev Drug Discov. 2019;18:569–72. [DOI] [PubMed]
Zapotoczna M, Forde E, Hogan S, Humphreys H, O’Gara JP, Fitzgerald-Hughes D, et al. Eradication of Staphylococcus aureus Biofilm Infections Using Synthetic Antimicrobial Peptides.J Infect Dis. 2017;215:975–83. [DOI]
Menzies-Gow A, Ponnarambil S, Downie J, Bowen K, Hellqvist Å, Colice G. DESTINATION: a Phase 3, multicentre, randomized, double-Blind, placebo-controlled, parallel-group trial to evaluate the long-term safety and tolerability of tezepelumab in adults and adolescents with severe, uncontrolled asthma.Respir Res. 2020;21:279. [DOI]
Mullard A. Tezepelumab prepares to enter the asthma antibody fray.Nat Rev Drug Discov. 2021;20:91. [DOI] [PubMed]
Simpson EL, Parnes JR, She D, Crouch S, Rees W, Mo M, et al. Tezepelumab, an anti-thymic stromal lymphopoietin monoclonal antibody, in the treatment of moderate to severe atopic dermatitis: A randomized phase 2a clinical trial.J Am Acad Dermatol. 2019;80:1013–21. [DOI] [PubMed]
Gottlieb A, Natsis NE, Kerdel F, Forman S, Gonzalez E, Jimenez G, et al. A Phase II Open-Label Study of Bermekimab in Patients with Hidradenitis Suppurativa Shows Resolution of Inflammatory Lesions and Pain.J Invest Dermatol. 2020;140:1538–45.e2. [DOI] [PubMed]
Lipa K, Zając N, Witkowski G, Ciechanowicz P, Wiszniewski K, Szymańska E, et al. Hidradenitis suppurativa - biologic therapy and other available treatment options.Postepy Dermatol Alergol. 2023;40:518–28. [DOI] [PubMed] [PMC]
Bachelez H, Choon SE, Marrakchi S, Burden AD, Tsai TF, Morita A, et al. Inhibition of the Interleukin-36 Pathway for the Treatment of Generalized Pustular Psoriasis.N Engl J Med. 2019;380:981–3. [DOI] [PubMed]
Gandhi NA, Bennett BL, Graham NM, Pirozzi G, Stahl N, Yancopoulos GD. Targeting key proximal drivers of type 2 inflammation in disease.Nat Rev Drug Discov. 2016;15:35–50. [DOI] [PubMed]
Gandhi NA, Pirozzi G, Graham NMH. Commonality of the IL-4/IL-13 pathway in atopic diseases.Expert Rev Clin Immunol. 2017;13:425–37. [DOI] [PubMed]
Tollenaere MAX, Mølck C, Henderson I, Pollack S, Addis P, Petersen HH, et al. Tralokinumab Effectively Disrupts the IL-13/IL-13Rα1/IL-4Rα Signaling Complex but Not the IL-13/IL-13Rα2 Complex.JID Innov. 2023;3:100214. [DOI] [PubMed] [PMC]
Ultsch M, Bevers J, Nakamura G, Vandlen R, Kelley RF, Wu LC, et al. Structural basis of signaling blockade by anti-IL-13 antibody Lebrikizumab.J Mol Biol. 2013;425:1330–9. [DOI] [PubMed]
Liour SS, Tom A, Chan YH, Chang TW. Treating IgE-mediated diseases via targeting IgE-expressing B cells using an anti-CεmX antibody.Pediatr Allergy Immunol. 2016;27:446–51. [DOI] [PubMed]
Grewe SR, Chan SC, Hanifin JM. Elevated leukocyte cyclic AMP-phosphodiesterase in atopic disease: a possible mechanism for cyclic AMP-agonist hyporesponsiveness.J Allergy Clin Immunol. 1982;70:452–7. [DOI] [PubMed]
Felding J, Sørensen MD, Poulsen TD, Larsen J, Andersson C, Refer P, et al. Discovery and early clinical development of 2-{6-[2-(3,5-dichloro-4-pyridyl)acetyl]-2,3-dimethoxyphenoxy}-N-propylacetamide (LEO 29102), a soft-drug inhibitor of phosphodiesterase 4 for topical treatment of atopic dermatitis.J Med Chem. 2014;57:5893–903. [DOI] [PubMed]
Tsiogka A, Kyriazopoulou M, Kontochristopoulos G, Nicolaidou E, Stratigos A, Rigopoulos D, et al. The JAK/STAT Pathway and Its Selective Inhibition in the Treatment of Atopic Dermatitis: A Systematic Review.J Clin Med. 2022;11:4431. [DOI] [PubMed] [PMC]
Cotter DG, Schairer D, Eichenfield L. Emerging therapies for atopic dermatitis: JAK inhibitors.J Am Acad Dermatol. 2018;78:S53–62. [DOI] [PubMed]
Liu H, Archer NK, Dillen CA, Wang Y, Ashbaugh AG, Ortines RV, et al. Staphylococcus aureus Epicutaneous Exposure Drives Skin Inflammation via IL-36-Mediated T Cell Responses.Cell Host Microbe. 2017;22:653–66.e5. [DOI] [PubMed] [PMC]
Esaki H, Brunner PM, Renert-Yuval Y, Czarnowicki T, Huynh T, Tran G, et al. Early-onset pediatric atopic dermatitis is TH2 but also TH17 polarized in skin.J Allergy Clin Immunol. 2016;138:1639–51. [DOI] [PubMed]
Noda S, Suárez-Fariñas M, Ungar B, Kim SJ, de Guzman Strong C, Xu H, et al. The Asian atopic dermatitis phenotype combines features of atopic dermatitis and psoriasis with increased TH17 polarization.J Allergy Clin Immunol. 2015;136:1254–64. [DOI] [PubMed]
Renert-Yuval Y, Del Duca E, Pavel AB, Fang M, Lefferdink R, Wu J, et al. The molecular features of normal and atopic dermatitis skin in infants, children, adolescents, and adults.J Allergy Clin Immunol. 2021;148:148–63. [DOI] [PubMed] [PMC]
Czarnowicki T, He H, Canter T, Han J, Lefferdink R, Erickson T, et al. Evolution of pathologic T-cell subsets in patients with atopic dermatitis from infancy to adulthood.J Allergy Clin Immunol. 2020;145:215–28. [DOI] [PubMed] [PMC]
Ungar B, Pavel AB, Li R, Kimmel G, Nia J, Hashim P, et al. Phase 2 randomized, double-blind study of IL-17 targeting with secukinumab in atopic dermatitis.J Allergy Clin Immunol. 2021;147:394–7. [DOI] [PubMed]
Naji A, Eitoku M, Favier B, Deschaseaux F, Rouas-Freiss N, Suganuma N. Biological functions of mesenchymal stem cells and clinical implications.Cell Mol Life Sci. 2019;76:3323–48. [DOI] [PubMed] [PMC]
Venkatarame Gowda Saralamma V, Vetrivel P, Kim SM, Ha SE, Lee HJ, Lee SJ, et al. Proteome Profiling of Membrane-Free Stem Cell Components by Nano-LS/MS Analysis and Its Anti-Inflammatory Activity.Evid Based Complement Alternat Med. 2019;2019:4683272. [DOI] [PubMed] [PMC]
He MT, Park HS, Kim YS, Lee AY, Cho EJ. Protective Effect of Membrane-Free Stem Cells against Lipopolysaccharide and Interferon-Gamma-Stimulated Inflammatory Responses in RAW 264.7 Macrophages.Int J Mol Sci. 2021;22:6894. [DOI] [PubMed] [PMC]
Park HS, Pang QQ, Kim YS, Kim JH, Cho EJ. Neuroprotective Effect of Membrane-Free Stem Cell Extract against Amyloid Beta 25–35-Induced Neurotoxicity in SH-SY5Y Cells.Appl Sci. 2021;11:2219. [DOI]