 Perspective
Perspective

Affiliation:
School of Psychology, University of Plymouth, PL4 8AA Plymouth, UK
Email: m.hyland@plymouth.ac.uk
ORCID: https://orcid.org/0000-0003-3879-0469
Explor Neuroprot Ther. 2026;6:1004152 DOI: https://doi.org/10.37349/ent.2026.1004152
Received: October 27, 2025 Accepted: April 09, 2026 Published: May 12, 2026
Academic Editor: Aurel Popa-Wagner, University of Duisburg-Essen, Germany
Explanations and treatment of fibromyalgia syndrome (FMS) and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are controversial, and outcomes are poor. This paper describes sensation-suppression theory, a theory modelled on self-organizing control systems that are capable of adaptation in response to inputs and used in applications of artificial intelligence. The theory shows how the need to suppress inflammatory and other causes of pain or fatigue due to challenging circumstances sensitizes the neurological processing of pain and fatigue, thereby creating the amplified sensations and abnormal cognitions of central sensitivity syndromes. These syndromes are caused by errors in an evolutionarily early behavior-control mechanism of animals that comes into conflict with the later cognitive behavior-control mechanism of humans. Unlike the cognitive and current biological theories, the sensation-suppression theory explains both the personality and biological risk factors for central sensitivity syndromes and why onset is sometimes gradual and sometimes sudden. A specific form of autonomic dysregulation that could act as a new empirical test of the theory is suggested. Recovery is achieved by reversing the biological homeostatic dysregulation through a specific form of pacing where the person changes from one short, non-stressful activity to another, and where activity is calibrated to the level of illness and the patient’s current biological state. Recovery is hampered or prevented by systemic inflammation and lifestyle obligations. The theory provides a sympathetic narrative for the cause and treatment of FMS and ME/CFS and promotes a recovery lifestyle that prioritizes the needs of the patient. Prevention requires hearing what the body is saying.
In the healthy person, sensations (e.g., pain, fatigue) have an adaptive function mediated through behavior. Pain prevents damage and promotes tissue healing through pain-avoiding behaviors. Fatigue inhibits activity, thereby promoting recovery from infection, injury, or overactivity. Each mental state inhibits behavior that is maladaptive. Sometimes these helpful sensations become amplified and become maladaptive symptoms. Fibromyalgia syndrome (FMS) (prevalence 2%) [1] is defined and diagnosed by widespread pain that cannot be explained by tissue damage. Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) (prevalence 0.76%) [2] is defined and diagnosed by fatigue that cannot be explained by known biological mechanisms. Diagnosis is based on the most severe symptom of a polysymptomatic spectrum of overlapping symptoms that vary in severity, with central sensitivity syndrome as a shared label applied to both FMS and ME/CFS [3–6].
Explanations and treatment of FMS and ME/CFS are controversial. Opinions differ over whether these functional somatic syndromes are caused by a biological error and should be treated biologically or by a psychological error and treated psychologically. FMS treatment guidelines recommend the use of multi-disciplinary teams that include psychologists, and where nonopioid pharmacological control of pain plays a primary role, though with limited effectiveness and unwanted side effects. A survey of physicians found that fewer than half agreed that any of the recommended interventions were effective [7], and physicians’ opinions vary as to whether FMS should be considered a biological or physical illness [8]. Psychologists vary as to whether their aim is adaptation to a chronic illness or cure [9]. An observational study of patients attending a FMS clinic over a period of five years found little overall improvement, and only 5% no longer met the criteria for FMS [10].
ME/CFS is a combination of two terms that separately imply either biological or psychological cause, reflecting a history of controversy and changing terminology [11]. There are no effective pharmacological treatments for ME/CFS. Psychological interventions and graded exercise therapy have a history of controversy [12–14]. Reviews of clinical trials of cognitive behavior therapy (CBT) for ME/CFS have consistently found CBT to be superior to control conditions. A recent meta-analysis of clinical trials found CBT to be effective in the short term, but long-term evidence was limited [15]. Clinical trials have been criticized because of selection bias and differential drop-out rates [16]. CBT was a recommended form of treatment in the 2007 evidence-based treatment guidelines for ME/CFS provided by the National Institute of Care Excellence (NICE) in the UK [17], but this recommendation was downgraded in the 2021 guidelines on the basis that evidence from clinical trials of CBT showing improvement was unreliable [18], this change being criticized as being “more ideology than science” [19] with a response that it was based on “robust evidence” [20] and that CBT can be “harmful” [14, 21]. CBT provides a rationale for recovery and hope [22], and some but by no means all patients find it helpful. Spontaneous recovery is estimated to occur in 6–8% of cases for short-term ME/CFS [23].
Not only are the cause and treatment of FMS and ME/CFS controversial, but there is disagreement over the interpretation of data, and outcomes are poor. Most psychologists support a psychological explanation for the cause and treatment of both types of illness. There are a few psychologists who have published papers that are critical of this perspective [13]. By contrast, most patients reject a psychological interpretation of their illness, and the relationship between ME/CFS patient support groups and psychologists is sometimes toxic [12]. Psychological terminology used with FMS patients frequently offends [24]. Dropout rates from psychological treatment are high, and many patients with both types of illness remain with a disabling chronic condition and feel unvalidated and unsupported by health professionals [25, 26]. Despite this, complete recovery can occur with or without treatment, and therefore, a recovery mechanism must exist. The history of science shows that solutions to difficult problems sometimes require a paradigm shift, though paradigm shifts are seldom welcomed initially, particularly where existing views are strongly supported [27]. In the case of FMS and ME/CFS, the two conflicting paradigms, psychological versus biological, are strongly supported and strongly criticized.
FMS and ME/CFS are defined as functional somatic syndromes because they lack the agreed specific pathophysiology that is required for disease definition and diagnosis. People with FMS and ME/CFS exhibit biological abnormalities that are shared with long-term stress and long COVID [28, 29], but none have been shown to be specific or useful for diagnosis. Both syndromes are described as central sensitivity syndromes [3–6]. Central sensitivity refers to the over-amplification of sensory signals by the central nervous system so that innocuous stimuli such as touch and movement are experienced as pain, subliminal levels of fatigue are experienced as fatigue, and other sensory inputs become amplified and aversive. Table 1 shows the frequency of symptoms indicative of central sensitivity in people with a diagnosis of FMS and ME/CFS. Although symptom frequency is similar, the severity of symptoms differs between different diagnostic categories. The overlap in symptom frequency and comorbidity is inconsistent with the nosological requirement for diagnostic separation, and cluster analysis shows FMS and ME/CFS to be variations of the same illness without a defining boundary [30].
Percentage of patients reporting a symptom indicative of central sensitivity on at least a weekly basis as a function of having an FMS or ME/CFS diagnosis.
| Symptom | FMS(n = 1,127*) | ME/CFS(n = 619*) |
|---|---|---|
| Fatigue for no reason | 97.1 | 97.3 |
| Fatigue increases the day after you are active | 95.7 | 97.3 |
| Pain in arms and legs that is not due to hard exercise | 94.9 | 84.0 |
| Pain increases the day after you are active | 94.9 | 90.2 |
| Pain moving from one part of the body to another on different days | 90.7 | 78.6 |
| Sensitive or tender skin | 86.0 | 72.2 |
| Sensitivity to bright lights | 78.8 | 83.8 |
| Sensitivity to noise | 83.0 | 83.8 |
| Easily feel too hot/sweating | 85.0 | 82.4 |
| Very cold hands or feet | 82.8 | 80.6 |
| Numbness, tingling, pins and needles | 79.3 | 72.1 |
| Thirsty all the time | 76.7 | 71.1 |
| Stomach pain | 70.9 | 68.0 |
| Jittery, easily startled, often worried | 74.5 | 68.4 |
| Feeling out of breath for no reason | 65.6 | 69.8 |
| Racing heart | 61.0 | 63.2 |
Source: Data from an online survey of FMS and ME/CFS patient support groups [31]. *: of whom 365 patients reported a diagnosis of FMS and ME/CFS. FMS: fibromyalgia syndrome; ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome.
Central sensitivity is a description of the functioning of the nervous system rather than an explanation of why the nervous system behaves in the way it does. The theory does not explain the cause of this error, it does not explain the type of neurological error, it does not provide a rationale for treatment, and, as the description applies equally to FMS and ME/CFS, it does not explain why some people have severe pain and some stronger fatigue symptoms, and some have both.
The pain experienced by FMS patients is described as nociplastic pain. The term nociplastic describes the cause as an alteration in the functioning of the nervous system, in contrast to nociceptive pain (caused by tissue damage) and neuropathic pain (caused by neurological damage). The term nociplastic draws attention to the plasticity of the network structure of the brain and is consistent with the functional description of FMS as a central sensitivity syndrome, though the latter term draws attention to the many other and variable symptoms associated with FMS and ME/CFS (see Table 1).
The cognitive model explains FMS in terms of hypervigilance. Hypervigilance describes a process of perceptual amplification where innocuous somatosensory stimuli are experienced as aversive [32]. Hypervigilance provides an explanation where the error of central sensitivity occurs at the distal end of the causal sequence: it occurs where biological events are interpreted and become sensations and therefore comprises a cognitive error. The error of FMS is therefore psychological rather than a biological error. The cause of hypervigilance is explained by a cognitive style of catastrophizing, a personality disposition that would predispose a person to be more aware of pain sensations [33]. In the cognitive model, there is a presumption that cognitive change will reduce catastrophizing and hypervigilance and therefore achieve a cure.
Biological explanations for the central sensitivity of ME/CFS include altered immune and metabolic activity [34], autonomic dysfunction [29, 35], and an undetected persisting virus [36].
The cognitive model of ME/CFS was developed in the early 1990s using the same concept of erroneous cognitions used previously for depression and anxiety [37, 38]. It proposes that people suffering from ME/CFS have the erroneous cognition that they are fatigued. This erroneous cognition then produces inactivity that, over time, causes a downward cycle of physical deterioration and yet more fatigue, leading to a state where the erroneous cognition of fatigue is applied to normal biological states. Recovery requires a gradual increase in activity that, over time, corrects the erroneous cognitions.
In sum, both FMS and ME/CFS can be explained as a kind of cognitive error, an explanation not always welcomed by patients who feel that their symptoms must have a biological basis despite the absence of an accepted biological explanation. CBT can be provided by psychologists, but CBT is rejected by many patients who feel misunderstood and neglected by the medical profession. Data has not provided a solution to this controversy; a new type of theory might.
A therapy can be effective for reasons other than the theory on which the therapy is based [39], so evidence of CBT effectiveness, whether accepted or not, provides a limited test of the cognitive model. An alternative way of testing a theory of illness is to deduce the factors that should increase the likelihood of illness developing and then observe whether those risk factors occur.
According to the cognitive model, people who are prone to developing FMS or ME/CFS pay too much attention and respond too strongly to the sensations of pain or fatigue. Personality factors that predispose towards attention of aversive states should therefore be predictive of illness, and this is confirmed with evidence that hypervigilance and catastrophizing are predisposing factors [33]. In addition, neuroticism will predispose towards recognition of aversive states and is a predisposing factor [40, 41], and the comorbidities of depression and anxiety, both associated with neuroticism, all point to a psychological cause.
However, not all personality predictors are consistent with the cognitive model. People who respond strongly to sensations of pain or fatigue should be high in awareness of internal states, and therefore, they should be low in alexithymia. Additionally, people prone to FMS and ME/CFS, according to the cognitive model, should desist from action when negative sensations arise, and so should be low in perfectionism. For the same reason, they should prioritize their need to reduce unpleasant sensations over the needs of others, and so should be low in self-sacrifice.
Contrary to the above predictions, a meta-analysis found the average prevalence of alexithymia in FMS was 48% compared to 10–13% in the general population [42], and other studies have shown that alexithymia has a prevalence of about 30% in ME/CFS patients [43, 44].
There are two components of perfectionism, typically labelled perfectionistic concerns (correlating with negative affectivity) and perfectionistic strivings (unrelated to negative affectivity) [45, 46]. Both perfectionist concerns and strivings are higher in people with FMS [47, 48] and ME/CFS [49] compared to healthy controls. Perfectionism is linked to conscientiousness, which has been found to be higher in people with ME/CFS [40].
Silencing the self is a personality trait describing self-sacrificing behavior. In one study, all four subscales of the silencing-the-self questionnaire were significantly higher in people with FMS compared to healthy controls, and self-silencing mediated the effect between adverse childhood experiences and symptoms in the group of people diagnosed with FMS but not in healthy controls [50]. In another study, compared to healthy controls, people with ME/CFS had higher levels of self-silencing and reported greater suppression of their emotions and needs [51].
In sum, although some personality risk factors of FMS and ME/CFS are consistent with the cognitive model, others are not. The logic of science requires that all data must be consistent with a theory for the theory to be true.
The personality characteristics that are found to predict risk according to the cognitive model (e.g., hypervigilance, neuroticism) support a public stereotype that people with FMS and ME/CFS are lazy [52, 53]. However, other risk data (perfectionism, conscientiousness, self-sacrifice) support the opposite stereotype, that people with these illnesses are overworking. The similarity between ME/CFS and burnout is recognized [54], and overactivity is a premorbid state of both FMS and ME/CFS [55], consistent with it having a causal role. However, many hardworking perfectionists do not become ill, so the explanation must be more complex.
Current explanations are either exclusively psychological or exclusively biological, each citing relevant psychological or biological evidence. A solution to the controversy could be provided by a functional explanation that has both biological and psychological content. This new theory should explain the variety of symptoms of central sensitivity and why central sensitivity sometimes presents as FMS, sometimes as ME/CFS, and sometimes as both.
Psychological theories are needed to explain the emergent properties of biological systems [56], and psychological theories provide a functional description of biological events [57]. Sensation-suppression theory is a functional theory that has psychological and biological content. The biological content comprises emergent properties of a biological system that are outside the normally prescribed discipline of psychology but can be described in terms of information and how that information functions with other types of information.
In addition to its content, a theory is defined by its form. Sensation-suppression theory is modelled on self-organizational control, a mechanism used in applications of artificial intelligence in robotics. Self-organization improves the functioning of control systems by changing the control system parameters when the control system makes errors according to a specific criterion [58–60]. Sensation-suppression theory assumes that central sensitivity syndromes are formed by errors in self-organizing control systems that integrate biological and psychological information and, by doing so, provide better functioning of both systems. However, under specific circumstances, this normally adaptive system ‘goes wrong’ and creates pathology [61]. The hypothesis that ME/CFS is a homeostatic error has been suggested before, but without explaining how this error comes about [62]. Sensation-suppression theory explains the formation of homeostatic error in a system that has both psychological and biological content.
Pain and fatigue are caused by a variety of biological events (e.g., infection, injury) and behavioral events (e.g., over-activity, behavioral persistence) that will be summarized by the functional label of challenges (see Figure 1). The challenges are detected in different ways (e.g., sensory nerves, neurological response to systemic inflammation, and endocrine changes), and together they provide a sensory input. All animals exhibit behavioral avoidance in response to aversive sensory inputs, so there must be an early-evolved biological mechanism for processing the sensory input. In animals, the sensory input is processed to form a stop signal. The stop signal increases with the duration and intensity of the challenges until it reaches a critical level and elicits behavior that avoids the challenge. Stop signals are produced to protect against any kind of threat to the body, irrespective of whether the threat is the result of an internal event or behavior. A sick or injured animal stops behaving. An animal avoids pain-causing behaviors and stops running when it becomes fatigued. Sensation-suppression theory assumes that this early-evolved mechanism exists in humans, and the stop signal is unavailable to consciousness. In humans, stop signals above the critical level contribute to sensations that are experienced as pain and fatigue or other sensations that inhibit behavior. Sensory inputs that form stop signals below the critical level do not create sensations.
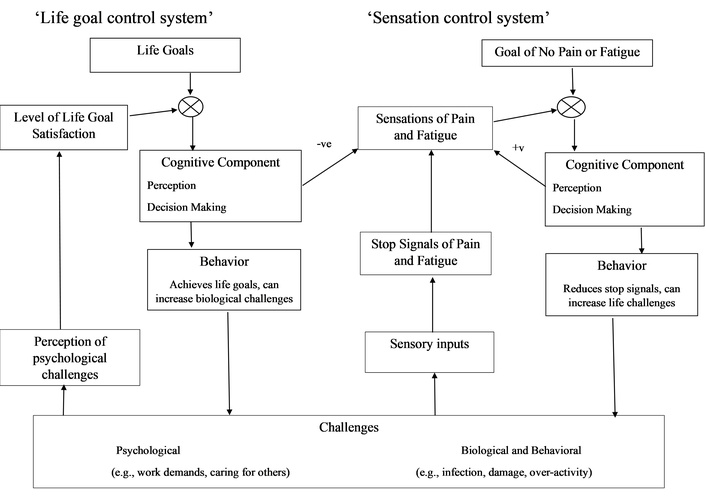
This figure shows two interacting control systems. The amplification (not shown) is a property of the whole control system and represents sensitivity to goal error. The control system with the greater amplification determines behavior. Key: +ve = perception increases pain or fatigue, -ve = perception decreases pain or fatigue.
The sensations of pain and fatigue are compared with the goal of no pain and fatigue, and the difference acts as input to a cognitive component. The cognitive component alters behavior to avoid the sensations of pain or fatigue using decision processes [63]. In addition, the cognitive component can change the strength of the sensation through attention [64]. By becoming hypervigilant, the increased attention on pain or fatigue sensations creates avoidant behavior. The strength of a sensation and the intensity of behavioral avoidance are influenced by two factors: the strength of the stop signal (a biological component) and the direction of attention (a psychological component). Sensory inputs, stop signals, sensations, cognition, and behavior act as a sensation control system, a control system that elicits self-protective behaviors to avoid challenges (see Figure 1).
The term amplification describes the relation between the level of detected error and the level of response in a control system and, together with the lag (the time elapsed), determines how the control system functions. If the amplification is too low, the system fails to respond sufficiently to disturbances. Too high amplification in relation to lag causes the system to overreact to error and can cause oscillation (an illustration is provided by temperature control in a shower). Amplification describes the sensitivity of a control system to error.
Because it is a property of the whole control loop, amplification is not commonly represented in control theory diagrams, but its importance is recognized [65, 66]. Control engineers use mathematical formulae that include amplification and lag to design a well-functioning control system [66]. Self-organizing control systems arrive at the same result using a specified criterion for how a well-functioning system should behave [58–60]. Sensation-suppression theory is predicated on the assumption that the correct amplification of sensations is achieved by self-organizing control systems using a criterion for correct functioning.
The optimum amplification level is one that is high enough to alter behavior to reduce pain and fatigue but not so high as to prevent these sensations from being overridden when an emergency requires it. An optimum level of this kind would have an evolutionary advantage and would be achieved by a criterion based on the relative frequency of self-protective behaviors that reduce adverse sensations versus the frequency and duration of those behaviors that do not. Sometimes it is necessary to ignore pain or fatigue to avoid a saber-toothed tiger, but these occasions will be infrequent and not last long. The criterion that creates optimum functioning would occur at a point where aversive sensations mostly alter behavior, but sometimes they do not, and only for a short duration. If behavior produces insufficient self-protective behaviors according to the criterion, then a self-organizing control system will increase amplification. If behavior produces too many self-protective behaviors according to the criterion, then the system decreases amplification.
Sometimes it becomes necessary to persist in an activity because psychological challenges (left side of Figure 1) have a greater priority over sensation control (right side of Figure 1). Prioritization of life goals occurs if the amplification (sensitivity to detected error) for life goals is greater than sensation control. People prioritize life goals for a variety of reasons: social and work obligations, caring for others, achieving personal goals, or avoiding negative consequences. Prioritization of life goals over sensations can reduce the perception of pain and fatigue. People do not notice negative sensations when their attention is elsewhere [64]. People can also decide to persist in an activity that maintains the sensations of pain and fatigue because of the importance of the activity. Sensation-suppression occurs if the person decides not to act on a sensation, does not notice the sensation due to attention elsewhere, or any combination of these two. Sensation-suppressive behavior occurs whenever behavior fails to respond to biological inputs in a timely manner.
Sensation-suppression does not by itself cause pathology, but if the proportion of sensation-suppressing behaviors is greater than self-protective behaviors according to the criterion, then the sensation control system will self-organize to correct the detected error.
There are two ways that a sensation control system can change the parameters of the sensation control system and therefore increase the frequency of self-protective behaviors. First, it can change the processing between the sensory inputs and the stop signal, and so cause an amplified stop signal. Sensory inputs that would have produced stop signals below the critical level now produce a stop signal above that level, thereby eliciting pain and fatigue where previously the sensory input would have been subliminal. The amplified stop signal creates the central sensitivity that is the defining feature of central sensitivity syndromes [3–6]. Second, it can produce cognitive changes that increase awareness and motivation to challenges, thereby switching attention away from life goals towards the sensation control system (see Figure 1). This will create the hypervigilance and cognitive abnormalities featured in the cognitive model [32].
The pain and fatigue produced by amplification cause inactivity, but activity fails to reduce the amplification. The reason is that once the amplification has reached a sufficiently high level, inactivity fails to reduce the previously subliminal biological challenges that are now causing stop signals and the symptoms of pain and fatigue. As a result, self-protective behaviors are not produced, and the system becomes ‘stuck’ in the new amplified mode of increased sensitivity to biological sensory inputs.
Pain and fatigue are caused by internal or external challenges or some combination of the two, but the type of amplification depends on whether the challenge causes pain or fatigue. Pain sensation-suppressive behaviors amplify pain and fatigue sensation-suppressive behaviors amplify fatigue. However, symptoms form symptom clusters because of a shared biology that has a variable network structure [67, 68], so, irrespective of cause, patients often experience both pain and fatigue and other symptoms associated with central sensitivity. The exact combination and severity of symptoms experienced by the patient depend on the sensation-suppressive behavior (how much pain or fatigue) and the biology of the patient.
Lifetime stress creates a generalized state of high alert to challenges, and so lifetime stress will increase the body’s sensitivity to pain and fatigue sensory inputs and therefore increase sensitivity to sensation-suppression. Lifetime stress has a bidirectional causal relationship with neuroticism [69], and both neuroticism and lifetime stress are risk factors for FMS [70] and ME/CFS [71]. Lifetime stress would act as a risk factor by lowering the criterion for sensation-suppressive versus self-protective behaviors, thereby making the sensation control system detect control error with lower frequencies of sensation-suppressive behaviors.
Long-term stress creates epigenetic changes, and there should therefore be genetic predisposing factors for FMS and ME/CFS. Genetic variants are associated with FMS [72] and ME/CFS [73] and are consistent with stress-related biological changes associated with FMS and ME/CFS [73]. However, according to the sensation-suppression theory, neither genetic factors nor lifetime stress has an independent causal role. Instead, they make central sensitivity more likely by altering the criterion and therefore making a person more vulnerable to the effects of frequent sensation-suppressive behaviors.
Sensation-suppression theory is a functional theory and does not attempt to explain specific biological events. Biological challenges are mediated through peripheral nerves, the autonomic nervous system, and the immune system, all of which can be altered by sensory amplification. In addition, because the body’s control systems are part of a biological network, homeostatic error in any one control system will tend to create error in other control systems. The consequence is that biological error and associated symptoms appear throughout the body and not only the symptoms associated with central sensitivity, including atopy (itchy eyes, runny nose), small fibre neuropathy (numbness, pins and needles), gastric abnormalities (diarrhoea, constipation), and cognitive and mood disturbance (anxiety, mental fog) [31, 67]. The symptoms of FMS and ME/CFS are not only pain; they are not only the symptoms of central sensitivity. They are symptoms caused by dysregulation in multiple biological control systems.
In summary, sensation-suppression theory describes a mechanism where a long-term imbalance between sensation-suppressing and self-protecting behaviors causes central sensitivity, but where sensitivity to this imbalance is increased by stress-related biopsychosocial factors. An injured cat hides and rests; humans have evolved greater cognitive capacity and can suppress the evolutionarily earlier response. When the proportion of sensation-suppressing behaviors versus self-protective behaviors increases above a criterion influenced by environmental and genetic predisposing factors, then the system adapts and gradually forms the amplified sensations of central sensitivity syndromes. Biological error is formed by lifestyle imbalance between over-activity in activities deemed important versus those inconsequential, pleasant, relaxing activities that can make life enjoyable.
The onset of FMS and ME/CFS is sometimes rapid and sometimes gradual. Sensation-suppressing behaviors lead to a gradual increase in the pathology of central sensitivity. However, if a person focuses attention away from sensations (e.g., a person is working hard but fails to notice feeling tired), then symptoms will not appear until the amplified stop signal becomes sufficiently strong to overcome the attentional focus away from the sensation. The person will experience pain or fatigue only once the stop signal has achieved some critical level when attention and priority switch away from the life goal to sensation control, and the amplified sensation is now perceived at a high level. The switch in attentional focus will be sudden and may be precipitated by an event that causes an increase in pain or fatigue (e.g., infection). By contrast, if amplification occurs without perceptual reduction of sensations (e.g., a person continues working but feels very tired when doing so), then the stop signal and sensation will increase together, and symptom onset will be gradual. The sudden versus gradual onset of FMS and ME/CFS is consistent with a catastrophe theory model [74] (see Figure 2). The greater the ability of the person to ignore pain or fatigue through inattention, the more suddenly they will appear, sometimes with a trigger (e.g., infection, injury) that acts as a catalyst. If a person persists in behavior despite experiencing pain or fatigue, then symptoms increase gradually.
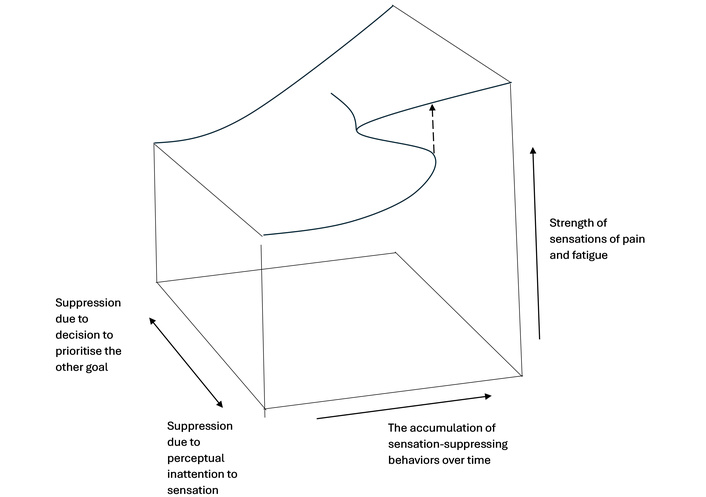
A catastrophe theory model of the gradual and rapid onset of symptoms. If a person experiences sensations of pain and fatigue but decides to ignore them, then over time, pain and fatigue increase gradually (back of the figure). However, if the person is unaware of pain and fatigue because the effect of the stop signal on sensation is suppressed through perceptual inattention, then, after sufficient accumulation of sensation-suppressing behaviors, there will be a catastrophic increase in symptoms as shown by the dotted arrow.
In summary, the pathology of central sensitivity develops slowly over time. When FMS and ME/CFS emerge suddenly, this is due to a trigger that can be mistaken for the cause of the illness. Because the pathology develops slowly, pain and fatigue can be experienced at low levels of central sensitivity pain but of insufficient intensity to attract a diagnosis of FMS and ME/CFS.
Sensation-suppression theory predicts that central sensitivity develops through a combination of two kinds of events: (a) a behavioral disposition to persist in an activity despite adverse sensations and (b) challenges that produce stop signals. These two events should, according to the theory, be risk factors. A risk factor, such as stress, can be explained by sensation-suppression theory, the cognitive theory, and possible biological theories, and is therefore not a good discriminator between theories. Other risk factors discriminate between these three types of theory.
The personality risk factors of alexithymia, perfectionism, and self-sacrifice are inconsistent with the cognitive theory (as shown above), as this theory suggests that pathology is caused by over-attention to pain or fatigue. By contrast, the sensation-suppression theory predicts that people prone to central sensitivity should have personality characteristics that make them prone to sensation-suppressive behavior. People high in alexithymia have low awareness of internal states and therefore fail to recognize pain or fatigue. People high in perfectionism are more likely to persist despite negative sensations, and people high in self-sacrifice are more likely to ignore negative sensations to satisfy the needs of others. All these risk factors are consistent with overactivity, which is a known premorbid state of FMS and ME/CFS [55]. Neuroticism is also a predictor of risk, and this predictor is consistent with the cognitive model. In terms of the sensation-suppression theory, neuroticism is associated with lifetime stress, which, according to the theory, is also a predictor of central sensitivity by altering the criterion. The theory is therefore consistent with known personality risk factors. All the personality risk factors are consistent with the sensation-suppression theory. Except for neuroticism and stress, none are consistent with the cognitive model or current biological models.
Diseases that cause pain and fatigue amplify stop signals and, if combined with activity, will cause sensation-suppression. Diseases that cause musculoskeletal pain make movement painful and, because movement is part of daily living, will associate activity and pain stop signals. Ehlers-Danlos syndromes (EDS) are inherited conditions, the most common being hypermobility EDS (hEDS), where looseness of connective tissue in the joints causes pain. A review found that the concomitant diagnosis of hEDS and FMS ranged between 68–89% [75].
Arthritis is a group of diseases causing inflammation and joint pain. One meta-analysis reported the prevalence of FMS in rheumatoid arthritis patients to vary between 4.9–52.4%, with a pooled estimate of 21% in contrast to 2% in the general population [76]. A review of the prevalence of FMS in patients with psoriatic arthritis reported that the prevalence varies between 8–30% [77].
Infection causes fatigue through nonspecific proinflammatory cytokines that affect the brain [78] and, if combined with continued activity, should increase the risk of ME/CFS. The herpes class of viruses (e.g., Epstein-Barr, causing glandular fever) is a well-known risk factor for ME/CFS [79–81]. Non-herpes viruses are also risk factors, including Ross River virus [82], pneumonia [83], and COVID [84]. A very large 17-year follow-up study found that the risk of developing ME/CFS after any virus was approximately the same as the risk of bacterial or fungal infection [85]. These results show that infection, rather than a particular type of infection, is the risk factor for ME/CFS. There is no evidence that an immunological abnormality caused by infection is a risk factor, as vaccination does not increase the risk of ME/CFS [86].
Further evidence of the inflammatory-fatigue effect comes from evidence that burn injury causes inflammation and fatigue [87] and increases the risk of ME/CFS [88]. Asthma exhibits both specific and systemic inflammation. FMS is a comorbidity of severe asthma [89], and severe fatigue is common [90], though severity varies between patients. A survey of severe asthma patients found that 45% reported waking feeling tired every day and 27% reported feeling tired for no reason every day [91].
There is limited evidence that the causal factor of ME/CFS is a combination of biologically caused fatigue and behavioral persistence. Research shows that after infection with glandular fever, those with a high level of motivation and whose fathers were overachievers had a greater risk of developing ME/CFS [92], as did those who responded to glandular fever with “all-or-nothing” behavior [93]. Infection increases the risk of ME/CFS by approximately one and a half times compared with non-infection [85], but the absolute risk of ME/CFS is low, as shown by a population prevalence of only 0.76% [2]. In some cases, infection could act as a catalyst that disinhibits perceptual suppression of fatigue and switches priority from life goal control systems to the sensation control system, see Figure 2. Infections are episodic, and the risk of ME/CFS following infection can be contrasted with the much greater risk of FMS associated with chronic pain disease.
In summary, sensation-suppression theory is consistent with known personality and biological risk factors for FMS and ME/CFS, whereas the cognitive theory and biological theories are consistent with only some of these risk factors (see Table 2). In addition, sensation-suppression theory explains why the emergence of symptoms is sometimes gradual and sometimes sudden. The psychological risk factors are those that lead to perseveration of behavior, and the biological risk factors are those that contribute to inflammation.
Risk factors are explained or not explained by three types of theory.
| Risk factor | Sensation-suppression theory (biology and psychology combined) | Cognitive theory (psychology only) | An unknown biological mechanism (biology only) |
|---|---|---|---|
| Stress | Yes | Yes | Yes |
| Neuroticism | Yes | Yes | No |
| Hypervigilance | Yes | Yes | No |
| Alexithymia | Yes | No | No |
| Perfectionism | Yes | No | No |
| Self-sacrifice | Yes | No | No |
| Diseases causing pain and FMS | Yes | No | Yes |
| Diseases causing fatigue and ME/CFS | Yes | No | Yes |
FMS: fibromyalgia syndrome; ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome.
Although the sensation-suppression theory is consistent with known risk factors, the theory can be evaluated further by testing new predictions from the theory. Sensation-suppression theory cannot explain the biological structures that cause central sensitivity, but it can predict how a biological system functions once the pathology has developed. The theory describes how two control systems operate at the same time and are in conflict. The function of the sensation control loop is to reduce sensation-causing activities and is therefore associated with parasympathetic activation. The life control loop functions to achieve some external goal and will therefore be associated with sympathetic arousal. Sensation-suppression, therefore, creates simultaneous parasympathetic and sympathetic activation. By analogy, the brakes of the car are on at the same time as the person is trying to accelerate.
The Hebbian rule (“cells that fire together, wire together”) describes how the neurological system functions; it is also the basis of associative learning in artificial intelligence. If parasympathetic and sympathetic activation is simultaneous, then, because of the Hebbian rule, this will lead over time to a neurological change so that parasympathetic and sympathetic activation occur simultaneously in situations where normally there would either be sympathetic activation and parasympathetic suppression or parasympathetic activation and sympathetic suppression. The theory, therefore, predicts that sensation-suppression should lead to an uncoupling of the normal reciprocal relationship between the parasympathetic and sympathetic nervous systems.
It is known that there are autonomic abnormalities in FMS and ME/CFS [35], but these abnormalities can be found in other conditions. Sensation-suppression theory provides a more precise prediction of that abnormality and, therefore, a test of the theory. The theory predicts that if the person with FMS or ME/CFS is exposed to a stressful event, then this will lead to an increase in both parasympathetic and sympathetic activation, at least in relation to a healthy person. Additionally, if the person tries to relax, this will also lead to an increase in both parasympathetic and sympathetic activation. By analogy, when the person with FMS or ME/CFS tries to do something, this produces simultaneous acceleration and braking.
Note that this is a functional test about how autonomic activity changes in response to events. It may be that in people with FMS and ME/CFS, there is both raised parasympathetic and sympathetic activation, but a better test of the theory is to examine the effect of environmental change on the change in parasympathetic and sympathetic activation caused by an intervention.
Sensation-suppression theory predicts that there is a specific autonomic abnormality associated with FMS and ME/CFS. Because central sensitivity can be present at subclinical levels, the autonomic abnormality should also be detectable in people who are experiencing sensation-suppression but are not yet ill. A further test would be whether the uncoupling of sympathetic and parasympathetic function is associated with alexithymia, perfectionism, and self-sacrifice.
Self-organization is a reversal process. Central sensitivity can be reversed by frequent self-protective behaviors and an absence of sensation-suppressing behaviors. This can be achieved by repeated behaviors that are of sufficient duration and intensity to cause a small increase in the stop signal, but then the behavior rapidly stops. Recovery requires activities that produce stop signals of low intensity but continue only for a short time. If the activity persists for too long or the intensity is too great, then the increase in the stop signal will persist for too long, and sensation-suppression will be detected. Because stop signals are amplified for people with central sensitivity, stop signals are formed sooner and with less vigorous activity for patients compared to healthy people. The more severe the patient, the more rapidly stop signals are formed.
Inactivity does not produce the behaviors needed for recovery and has two negative consequences. Pain sensitivity decreases with exercise, and inactivity increases pain sensation [94, 95]. Inactivity can further sensitize the sensation control system to pain and fatigue, causing sensory inputs, thereby increasing illness severity. Additionally, inactivity has biological effects that negatively impact the functioning of the body, making it less resilient to stress. Prolonged inactivity can result in the patient becoming bedbound. By contrast, any attempt to maintain the previous lifestyle can be counter-productive by contributing further to sensation-suppression, which was the original cause of illness and creates further deterioration.
According to the sensation-suppression theory, stress reduces the criterion and makes the system more sensitive to sensation-suppressive behaviors. Activities and lifestyle changes that reduce stress will make the system less sensitive to sensation-suppression and therefore promote recovery, as sensation-suppression is difficult to avoid. In addition, stress increases systemic inflammation, which acts to increase stop signals. Relaxing, positive experiences counteract the effects of stress. Reversal theory [96] shows that under conditions of stress, non-goal-oriented activities create a more positive mood, so short episodes of non-goal-oriented activity are likely to be helpful in these illnesses where stress is often a contributing factor.
The optimal duration, intensity, and type of activity will vary between patients. Any activity will increase a stop signal as a function of duration, but the increases will be greater in people with more severe central sensitivity syndrome because of the greater amplification between the sensory input and stop signal. Consequently, very ill people will tolerate less intense activity for shorter periods of time compared to people with mild central sensitivity syndromes.
Because the stop signal is formed from a precognitive mechanism, animal research provides useful insight. If a rat is always rewarded for turning right in a T-maze, then, according to Thorndike’s two laws, the rat should always turn right. In fact, the rat sometimes turns left, a phenomenon known as spontaneous alternation in a maze and explained by “reactive inhibition”. Reactive inhibition is a biological stop signal: it increases over time and is dissipated over time with a change of activity [97]. This little-known animal research is important in showing that there is a third cause to stop signals in addition to biological and behavioral causes of pain and fatigue referred to above (see Figure 3). The third cause is behavioral persistence, irrespective of the type of behavior. For people with central sensitivity syndrome, the amplification of the stop signal is so great that stop signals will be caused by persistence over a relatively short period of time for any activity. Therefore, changing to a different type of activity (e.g., mental versus physical) over shorter times than normal is needed to produce behavior that is responsive to stop signals, that is, the type of behavior that leads to a gradual reduction in central sensitivity. For patients with less severe illness, a change to an entirely different type of activity is likely to be as effective as resting, and the principle of changing rather than resting is one that should have merit except for very severe illness. Long rests are not advised based on this theory because resting does not provide information that there is a timely and appropriate response to stop signals.
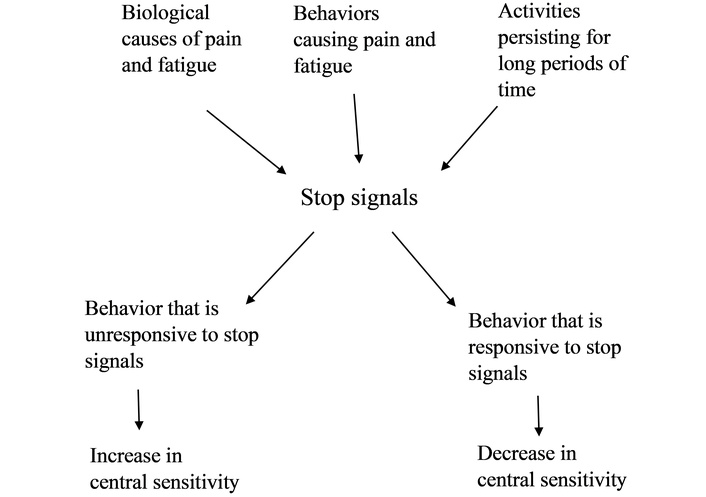
Flow diagram of events causing or preventing central sensitivity. Behavior that responds to an increase in stop signals in a timely manner decreases central sensitivity. Behavior that does not respond to an increase in stop signals in a timely manner increases central sensitivity. When central sensitivity is present, stop signals are amplified in relation to their antecedents.
Injury and infection are challenges that cause sensory inputs for pain and fatigue, so when they occur, activity levels should be reduced substantially, and activity levels should be reduced if the person experiences a psychological stressor. Reduction in activity under these circumstances teaches the body that correct responses are being made to stop signals. By contrast, ‘all or nothing’ behavior when ill is pathogenic [93].
Sensation-suppression theory is a functional theory and does not provide predictions about biological factors that aid recovery. However, lifestyle or pharmacological changes that reduce inflammation could be helpful because inflammation is a cause of stop signals experienced as pain and fatigue. There is insufficient evidence to conclude whether dietary interventions and supplements are helpful or not [98], but healthy and enjoyable eating can promote positive activity and better well-being, and improved diet and vitamin and mineral supplements could support the overall functioning of a stressed body and act synergistically when combined with behavioral adaptations described above. Long-term pharmacological suppression of symptoms will be counterproductive because doing so promotes sensation-suppression. Opioid hyperalgesia is a condition of increased pain sensitivity induced by frequent opioid use [99].
In summary, the behaviors needed for recovery can be described as neither too great nor too little and, like Goldilocks’s porridge, are ‘just right’. These Goldilocks behaviors will vary between people and are experienced as pleasant, relaxing, of short duration, and low intensity. They should be followed by a short rest or a change in activity, and they should be repeated on a regular basis. Recovery is a slow process requiring years, not months. High levels of activity are not themselves pathogenic but only when they are not balanced by sufficient self-protective behaviors. These self-protective behaviors vary with motivation and interest and are experienced as inconsequential, positive, and relaxing. Positive experiences of this kind are protective against future illness in those whose lives are characterised by hard work. The theory provides a rationale for illness prevention: if you must work hard or push through pain, make sure you also have time when you can rest and have fun.
Sensation-suppression theory provides a rationale for treating nociplastic pain and fatigue only if they are caused by the mechanism of sensation-suppression. There may be other possible mechanisms, in which case the theoretical rationale for treatment presented here may not apply.
Recovery requires activity rather than rest, but the therapeutic window between over-activity and under-activity is narrow and varies between patients and over time. Over-activity (i.e., too long or too intense) causes ‘boom-and-bust’ or post-exertional malaise, a phenomenon indicative of FMS and ME/CFS [100] where pain and fatigue symptoms increase substantially 24 hours after an activity rather than immediately after the activity [101, 102] (see Table 1). The delay in the boom-and-bust phenomenon is inconsistent with energy depletion or tissue damage but is consistent with a process of adaptation where over-activity creates sensation-suppression and increases central sensitivity. Boom-and-bust can be a useful indicator that the level of activity was too great, and the person should modify behavior accordingly.
Pacing of activity can help avoid the post-exertional malaise of overactivity. Despite initial doubts over the value of pacing [103], current clinical consensus supported by reviews is that pacing is helpful at least to some degree [104, 105]. A common form of pacing is to tell patients to achieve only 70% of what they feel they can achieve. While this advice can be helpful, a more precise guide about pacing could produce better results.
Because of reactive inhibition (see Figure 3), work, leisure, and mental activities create stop signals after a while, and therefore any form of mental or physical activity should be of short duration, followed by a short rest or another activity. For example, a two-hour film should be watched in separate episodes. Taking breaks during work is shown to be helpful in healthy individuals [106]. Physical activity causes a rapid increase in stop signals and should be limited initially to short episodes of low-intensity exercise. A clinical trial found that tai chi produced superior outcomes compared to aerobic exercise for FMS patients [107, 108], a finding consistent with low-intensity physical exercise being helpful. Some patients find graded exercise therapy helpful, while others find it is harmful [109]. The variation in patient response to the same intervention is consistent with exercise being helpful only if it is within the patient’s therapeutic window of activity tolerance. The extreme amplification of stop signals of bedbound patients may limit physical activity to raising and lowering the arm a few times every half an hour. The duration, intensity, and type of activity can be increased very, very slowly, where any increase should be attempted only after at least a month of stability has been achieved. Activity levels should be adjusted down during infection or any form of biological or psychological challenge. The patient should become the expert in determining what type, intensity, and duration of behavior promotes recovery and what is pathogenic, using post-exertional malaise as an indicator of pathogenic behavior.
Psychological treatments for central sensitivity syndromes often include evidence-based third-wave CBT techniques (e.g., mindfulness, self-compassion therapy, acceptance and commitment therapy, gratitude therapy). For many patients, these are Goldilocks activities because they provide emotionally positive, relaxing experiences, they are low intensity, there is no external goal, and they are of short duration. Emotionally positive, relaxing experiences are also provided by the energy therapies of complementary and alternative medicine. These therapies provide behavioral interventions that are rich in meaning [110, 111]. Sham and real Reiki are both beneficial for FMS [112–114] and ME/CFS [114, 115]. Sham and real distant healing produce equal and significant benefit for ME/CFS [116]. Manual therapies (no valid sham) also improve outcomes. A meta-analysis found that massage improved outcomes for ME/CFS [117] and the Bowen technique improves FMS [118] and chronic pain [119]. Chinese mind-body exercises (qigong and tai chi) have been found beneficial for ME/CFS [120], and tai chi has been found effective for FMS [108], as has virtual reality treatment [121].
The considerable heterogeneity of the interventions that improve outcomes, at least in the short term, is consistent with the hypothesis that they are effective through a single mechanism. They all provide the opportunity for a person to engage in self-protective behaviors, and it is these behaviors that reduce the pathological amplification of the stop signal. Different patients will benefit from different interventions depending on the match between the meaning associated with the therapy and the person’s values and beliefs [122]. Self-protective behaviors ‘feel good’ but different behaviors ‘feel good’ for different people. There may be a ‘best’ intervention for a particular patient, but it is unlikely that there is a ‘best’ intervention for all.
The various therapeutic interventions described above are effective in the short term, but without evidence of long-term effectiveness. Long-term outcomes of central sensitivity syndromes are known to be poor despite best practice [10]. Although an intervention can help in the short term, the self-protective experience often stops after treatment stops, and even if the patient continues with the experience, it takes up only a small part of the patient’s day.
There are two reasons that make recovery difficult. The first is that the circumstances that give rise to illness often persist, and illness adds additional stress to a lifestyle already full of challenges. Stress increases systemic inflammation. It can be difficult to change established patterns of behavior and obligations to others, and pleasant, inconsequential activities can be difficult to achieve in busy lives. Patients may need help to set barriers that prioritize their own needs over others, to not feel they must be perfect, and to manage the demands and commitments of dependents, relatives, employers, and others. Patients may need ‘permission’ to be kind to themselves (e.g., a prescription of a ‘treat a day’). Recovery requires activities where the proportion of self-protective behaviors is high compared to sensation-suppressive behaviors, and so comprehensive behavioral change in daily life is often needed.
A second reason that can make recovery difficult is that central sensitivity syndromes are often comorbid with inflammatory diseases or other conditions that cause systemic inflammation. Inflammation is a challenge that causes stop signals, making it more difficult for patients to engage in behaviors that are not associated with stop signals. Anti-inflammatory medicines reduce inflammation but have other effects, so the benefit from use, if any, would need to be determined empirically. Anti-inflammatory control through lifestyle or medication could be helpful, but requires investigation.
For these two reasons, full recovery is possible but difficult. However, even when fully recovered, a person may not be able to revert to an earlier lifestyle without a return of symptoms.
People with FMS and ME/CFS can be resistant to psychological interpretations of their illness and reject therapy that does not involve some form of biological intervention. Sensation-suppression theory provides a more sympathetic explanation of the cause of illness than the cognitive model, and it contains a biological element. However, because behavioral change is needed for recovery, engagement can be reduced if an intervention is interpreted as psychological [12, 24].
Body reprogramming [123] is an intervention for FMS currently provided in a limited number of centers in the UK on the NHS (National Health Service) based on an earlier, less well-developed version of the theory [61, 124], but, like the present theory, provides a sympathetic narrative for the cause and treatment of central sensitivity. Patient engagement is achieved through analogies and by providing a biologically focused explanation of their illness. This intervention has been found by patients to be empowering and promotes hope and activates lifestyle change [125, 126] as well as producing positive outcomes [127].
Because patients’ lives differ, patients should be empowered to find out for themselves, rather than being told what to do. To achieve this objective, strategic questioning [128] may be more helpful than direct suggestions. The health professional should help patients discover the best way that ‘little and often’ can be applied to their lives.
Finally, the labels FMS and ME/CFS provide a poor description of etiology and symptomatology and are associated with negative stereotypes. The term central sensitivity syndrome fails to acknowledge other biological abnormalities and symptoms associated with FMS and ME/CFS. Consensus for better terminology would assist scientific understanding and patient communication.
A mechanical control system malfunctions if any part becomes broken or worn. The error is localised and specific. The modern disease concept is modelled on the same principle of specificity. A disease is defined by a specific pathophysiology that is unique to only one disease. A self-organizing control system can malfunction in the same way, but it can also malfunction because system parameters (e.g., gain, lag) have been incorrectly set due to self-organizational change. System errors are distributed over the control system, and therefore, there is no specific pathophysiology. Sensation-suppression theory proposes that central sensitivity syndromes are caused by a distributed error resulting from a particular type of challenging lifestyle. This type of error will not reveal itself as a specific pathophysiology but will be associated with multiple biological abnormalities. The system error can be diagnosed only through symptoms and the way the body functions.
Some chronic illnesses exhibit spontaneous recovery or recovery through lifestyle change, and for these illnesses, a self-correcting mechanism must exist. Sensation-suppression theory provides an example of a self-correcting mechanism. However, self-correcting mechanisms must exist for other illnesses where complete remission rather than only control is sometimes achieved, and this type of mechanism provides the potential for new understanding and treatments. Lifestyle medicine exploits the body’s ability to self-heal, given the right conditions [129], and the concept of a self-organising control system provides a new way of understanding the effects of lifestyle as adaptation rather than damage. Illness caused by adaptation can be prevented. In the case of central sensitivity syndromes, prevention requires hearing and responding to what the body is saying. Some other illnesses could also be preventable with a better understanding of the body’s adaptation mechanisms.
CBT: cognitive behavior therapy
FMS: fibromyalgia syndrome
hEDS: hypermobility Ehlers-Danlos syndromes
ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome
MEH: Conceptualization, Visualization, Writing—original draft, Writing—review & editing. The author read and approved the submitted version.
The author declares that he has no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 1694
Download: 35
Times Cited: 0
