 Meta-Analysis
Meta-Analysis

Affiliation:
1Faculty of Educational Studies, University Putra Malaysia, Selangor 43400, Malaysia
Email: jhgao523@163.com
ORCID: https://orcid.org/0000-0002-7129-6465
Affiliation:
2Sports Nutrition Centre, National Sports Institute of Malaysia, Kuala Lumpur 57000, Malaysia
ORCID: https://orcid.org/0009-0001-4092-6348
Affiliation:
3Division of Research and Innovation, National Sports Institute of Malaysia, Kuala Lumpur 57000, Malaysia
ORCID: https://orcid.org/0000-0002-5095-7682
Affiliation:
4College Institute of Sports Medicine and Rehabilitation, Shandong First Medical University, Tai’an 271016, Shandong Province, China
Affiliation:
1Faculty of Educational Studies, University Putra Malaysia, Selangor 43400, Malaysia
Affiliation:
5Division of Sports Medicine, National Sports Institute of Malaysia, Kuala Lumpur 57000, Malaysia
Affiliation:
1Faculty of Educational Studies, University Putra Malaysia, Selangor 43400, Malaysia
Explor Musculoskeletal Dis. 2026;4:1007124 DOI: https://doi.org/10.37349/emd.2026.1007124
Received: December 23, 2025 Accepted: May 05, 2026 Published: June 04, 2026
Academic Editor: Ashok N. Johari, Children’s Orthopaedic Centre, India
Background: Pain affected gait performance in patients with non-specific chronic low back pain (NSCLBP) due to protective mechanisms in response to pain. Insufficient evidence demonstrated whether pain altered the walking patterns in NSCLBP. Therefore, this review aimed to compare the walking patterns between individuals with and without NSCLBP.
Methods: The literature was systematically reviewed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The Cochrane, PubMed, Web of Science (WOS), EMBASE, and EBSCOhost were searched for the relevant studies, which were included if they: 1) compared patients with NSCLBP to the healthy controls, 2) evaluated spatiotemporal gait characteristics, 3) were published in English, 4) were peer-reviewed original research articles, and 5) were published since the year of 2000. Two researchers independently assessed the quality of the studies using the modified Downs and Black checklist. Meta-analyses with the random effects model were used, and the standardized mean differences (SMD) and the 95% confidence intervals (CI) were analyzed.
Results: Out of 822 records, thirteen studies were included in the systematic review, and twelve were incorporated into the meta-analysis. The meta-analysis revealed significant differences between NSCLBP patients and healthy controls in walking speed (SMD = –0.67, 95% CI: –1.08 to –0.25, p = 0.002, I2 = 76%) and step length (SMD = –0.55, 95% CI: –0.94 to –0.17, p = 0.004, I2 = 64%).
Discussion: Within spatiotemporal gait parameters, patients with NSCLBP show moderately consistent reductions in walking speed and step length relative to healthy controls, which may reflect pain-related protective strategies. These alterations underscore clinically meaningful gait impairments that should be considered in the design of targeted rehabilitation programs. PROSPERO registration number is CRD42023418511.
Non-specific chronic low back pain (NSCLBP) is characterized by pain located below the twelfth thoracic vertebra and extending to the upper gluteal folds in the rear, lasting for at least twelve weeks, without any identifiable structural or etiological cause [1, 2]. NSCLBP is a prevalent condition, with studies indicating that 46% to 80% of adults experience it at some point in their lives [3]. A significant number of individuals with NSCLBP develop kinesiophobia—a fear of movement—due to an excessive focus on pain [4]. This condition not only heightens awareness of discomfort and fear of movement but also affects the movement quality [5]. Emerging evidence suggests that NSCLBP is associated with central sensitization, a phenomenon characterized by heightened pain perception at the cortical level, which disrupts motor control by interfering with motor planning and execution [6, 7]. Furthermore, individuals with NSCLBP often demonstrate reduced hip and spinal extension during everyday activities, primarily due to pain-induced neuromuscular adaptations [8]. These adaptations usually lead to inhibition of the agonist muscles and overactivation of the antagonist muscles, causing imbalances in muscle length and tension [9]. Such neuromuscular disruptions contribute to abnormal movement patterns, including gait alterations, further impacting functional performance and quality of life [10].
Gait is a fundamental movement crucial for daily activities and serves as a key clinical tool for assessing physical function and recovery in NSCLBP patients [11, 12]. Commonly assessed gait parameters include kinetic characteristics, such as joint moments and ground reaction forces, and kinematic parameters, including joint angles, linear and angular displacements, and velocity. Spatial and temporal gait parameters are commonly used in gait assessments because these parameters require high levels of muscle coordination in the lower limbs [13]. Patients with NSCLBP often exhibit muscle weakness, stiffness, or abnormal muscle control, which can influence lower limb activity and affect spatiotemporal parameters.
The evidence regarding spatiotemporal parameters in NSCLBP patients compared to healthy individuals remains controversial, likely due to a combination of clinical, psychological, and methodological factors. Observational evidence suggests that patients with NSCLBP exhibit abnormal gait characteristics as a pain accommodation strategy [14], particularly in spatiotemporal gait parameters such as walking speed, step length, cadence, step width, stance phase, single support phase, swing phase, and stride length. Several studies have also indicated that individuals with NSCLBP exhibit slower walking speeds, shorter step lengths, and reduced cadences [15, 16]. Conversely, some studies have reported that NSCLBP patients show no significant differences in spatiotemporal parameters compared to healthy individuals. For example, Gombatto et al. [17] concluded that there was no statistical difference in stride duration, step length, and walking speed between patients with NSCLBP and healthy participants. Given these inconsistencies and the lack of specificity in existing research, there is a need for a more focused examination of spatiotemporal gait parameters in NSCLBP patients. Therefore, this study aims to systematically review, synthesize, and quantify the evidence on variations in spatiotemporal gait parameters between NSCLBP patients and healthy individuals.
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol was registered on the PROSPERO website (http://www.crd.york.ac.uk/prospero) with registration number CRD42023418511.
Cochrane, PubMed, Web of Science (WOS), Embase and EBSCOhost, were accessed for searching the related articles with the keywords of ‘chronic non-specific low back pain’, ‘NSCLBP’, ‘chronic low back pain’, ‘CLBP’, ‘low back pain’, ‘LBP’, ‘back pain’, ‘lumbar pain’, ‘spinal pain’, ‘lumbar pelvic pain’, ‘lumbar-pelvic pain’, ‘healthy participant’, ‘healthy control’, ‘asymptomatic individual’, ‘asymptomatic subject’, ‘healthy subject’, ‘gait pattern’, ‘gait’, ‘gait parameter’, ‘walking’, ‘gait characteristic’, ‘gait analysis’, ‘gait behavior’, ‘gait kinetics’. Boolean operators ‘AND’ and ‘OR’ were applied to combine the keywords in a search, and a valid wildcard of an asterisk (*) was added to some of the keywords to broaden the search. The concrete searching strategies of each database can be referred to in Table 1. Only document types (full-text or trials), language (English) and human studies were limited during search in each database. The latest search was updated on 22nd July 2024.
Search strategy.
| Library | Search statement | Results |
|---|---|---|
| Cochrane | #1 (non-specific chronic low back pain OR NSCLBP OR chronic low back pain OR CLBP OR low back pain OR LBP OR back pain OR lumbar pain OR spinal pain OR lumbar pelvic pain OR lumbar-pelvic pain):ti,ab,kw in Trials (Word variations have been searched)#2 (healthy participant* OR healthy control* OR asymptomatic individual* OR asymptomatic subject* OR healthy subject*):ti,ab,kw in Trials (Word variations have been searched)#3 (gait pattern* OR gait OR gait parameter* OR walking OR gait characteristic* OR gait analysis OR gait behavior* OR gait kinetics):ti,ab,kw in Trials (Word variations have been searched)#4 #1 AND #2 AND #3 | 128 |
| PubMed | ((“non-specific chronic low back pain”[Title/Abstract] OR “NSCLBP”[Title/Abstract] OR “chronic low back pain”[Title/Abstract] OR “CLBP”[Title/Abstract] OR “low back pain”[Title/Abstract] OR “LBP”[Title/Abstract] OR “back pain”[Title/Abstract] OR “lumbar pain”[Title/Abstract] OR “spinal pain”[Title/Abstract]) AND (“healthy participant*”[Title/Abstract] OR “healthy control*”[Title/Abstract] OR “asymptomatic individual*”[Title/Abstract] OR “asymptomatic subject*”[Title/Abstract] OR “healthy subject*”[Title/Abstract]) AND (“gait pattern*”[Title/Abstract] OR “gait”[Title/Abstract] OR “gait parameter*”[Title/Abstract] OR “walking”[Title/Abstract] OR “gait characteristic*”[Title/Abstract] OR “gait analysis”[Title/Abstract] OR “gait behavior*”[Title/Abstract] OR “gait kinetics”[Title/Abstract])) AND ((fft[Filter]) AND (English[Filter])) | 103 |
| WOS | AB=( non-specific chronic low back pain OR NSCLBP OR chronic low back pain OR CLBP OR low back pain OR LBP OR back pain OR lumbar pain OR spinal pain OR lumbar pelvic pain OR lumbar-pelvic pain) AND AB= (healthy participant* OR healthy control* OR asymptomatic individual* OR asymptomatic subject* OR healthy subject*) AND AB= (gait pattern* OR gait OR gait parameter* OR walking OR gait characteristic* OR gait analysis OR gait behavior* OR gait kinetics) and Article (Document Types) and English (Languages) | 221 |
| Embase | #1 (‘non-specific chronic low back pain’ OR ‘nsclbp’ OR ‘chronic low back pain’/exp OR ‘chronic low back pain’ OR ‘clbp’ OR ‘low back pain’/exp OR ‘low back pain’ OR ‘lbp’ OR ‘back pain’/exp OR ‘back pain’ OR ‘lumbar pain’/exp OR ‘lumbar pain’ OR ‘spinal pain’/exp OR ‘spinal pain’ OR ‘lumbar pelvic pain’ OR ‘lumbar-pelvic pain’) AND [humans]/lim AND [English]/lim#2(‘healthy participant*’ OR ‘healthy control*’ OR ‘asymptomatic individual*’ OR ‘asymptomatic subject*’ OR ‘healthy subject*’) AND [humans]/lim AND [English]/lim#3 (‘gait pattern*’ OR ‘gait’ OR ‘gait parameter*’ OR ‘walking’ OR ‘gait characteristic*’ OR ‘gait analysis’ OR ‘gait behavior*’ OR ‘gait kinetics’) AND [humans]/lim AND [English]/lim#4 #1 AND #2 AND #3 | 205 |
| EBSCOhost | AB (non-specific chronic low back pain OR NSCLBP OR chronic low back pain OR CLBP OR low back pain OR LBP OR back pain OR lumbar pain OR spinal pain OR lumbar pelvic pain OR lumbar-pelvic pain ) AND AB ( healthy participant* OR healthy control* OR asymptomatic individual* OR asymptomatic subject* OR healthy subject* ) AND AB ( gait pattern* OR gait OR gait parameter* OR walking OR gait characteristic* OR gait analysis OR gait behavior* OR gait kinetics) ; limiters full text and English | 165 |
Two researchers (JG and JST) independently evaluated the eligibility of articles according to predefined inclusion and exclusion criteria to minimize bias, with any disagreements resolved through consultation with a third reviewer (SW).
Full-text, peer-reviewed original research articles since 2000 were included if the following inclusion criteria were met: 1) The primary study population consisted of patients with NSCLBP who had experienced pain for a minimum of three months; 2) Gait or walking pattern is captured by the motion capture system, treadmill and gait mat; 3) The study reported spatiotemporal variables such as walking speed (m/s), step length (m), cadence (steps/min), step width (m), stance phase (%), single support phase (%), swing phase (%), and stride length (m).
Articles were excluded if those met the following exclusion criteria: 1) The full text of the article was unavailable; 2) Mean values and standard deviations of relevant parameters were not reported; 3) The parameters were not related to spatiotemporal parameters; 4) The study population included other types of low back pain, such as acute low back pain, sub-acute low back pain, or low back pain with specific causes.
All findings were imported into EndNote X8 (Thomson Reuters), where duplicate references were identified and removed using the duplication detection feature. Two researchers (JG and JST) independently screened the remaining entries by reviewing the titles and abstracts. Studies were excluded if they were thesis, guidelines, conference presentations, protocols, reports, reviews, grey literature, or non-English articles. After this initial screening, the remaining articles underwent eligibility assessment based on the predefined criteria. The primary outcomes of interest were spatiotemporal gait parameters, including walking speed, step length, cadence, step width, stance phase, single support phase, swing phase, and stride length. Articles matching the relevant keywords and content were selected for inclusion in the systematic review. Additionally, studies that reported the mean and standard deviation of these parameters were included in the meta-analysis. The data extraction process was independently carried out by two researchers (JG and JST) to ensure accuracy and consistency.
To minimize bias, two researchers (JG and JST) independently assessed the methodology quality and referred to the modified version of the Downs and Black checklist [18, 19]. Four categories were evaluated, including the reporting (questions 1, 2, 3, 5, 6, 7, and 10), external validity (questions 11 and 12), internal validity (questions 16, 18, and 21), and confounding (questions 21, 22, and 25). Each question was scored as either 1 (Yes) or 0 (No or unable to determine), except for question 5, which was scored as 2 (Yes), 1 (Partial), or 0 (No), giving a maximum total score of 16. Discrepancies were resolved through discussion, with a third researcher consulted when necessary. Inter-rater reliability was assessed using Kappa correlation.
Review Manager 5.4 (Copenhagen, the Nordic Cochrane Centre, Cochrane Collaboration) software was used to do a meta-analysis. The forest plot with the random effects model was compared to the kinematic gait data between the NSCLBP patients and the healthy controls. I2 was used to check the heterogeneity among studies, and it could be classified into three levels, which included low heterogeneity (0–50%), moderate heterogeneity (50–75%), and high heterogeneity (> 75%) [20]. The total standardized mean difference (SMD, effect size [ES]), 95% confidence interval (CI), and p-value were calculated. ES was categorized into small effect (0.2–0.5), medium effect (0.5–0.8), and large effect (> 0.8) [21]. The percentage would be calculated with the formula (percentage = scored/total score (16) × 100%). Kappa’s correlation was analyzed by SPSS (v26.0; CED, Cambridge, United Kingdom), and no more than 60%, 60% to 75%, and above 75% were considered lower quality, moderate quality, and high quality, respectively [18].
822 papers were found from the databases of Cochrane (128/822), PubMed (103/822), WOS (221/822), Embase (205/822), and EBSCOhost (165/822). 359 duplicated papers were removed. Non-English (1/463), non-related title or abstract (359/463), case report (2/463), conference (1/463), review (4/463), and research protocols (74/463) were excluded. Meanwhile, nine studies out of 22 were not retrieved due to violating the eligibility assessment of the unrelated parameters or targeted participants. Eventually, thirteen studies were included in the systematic review [15, 16, 22–32]. One [26] out of 13 was not entered into the meta-analysis due to missing reporting of the mean and standard deviation. Therefore, twelve studies [15, 16, 22–25, 27–32] were included in the meta-analysis (Figure 1).
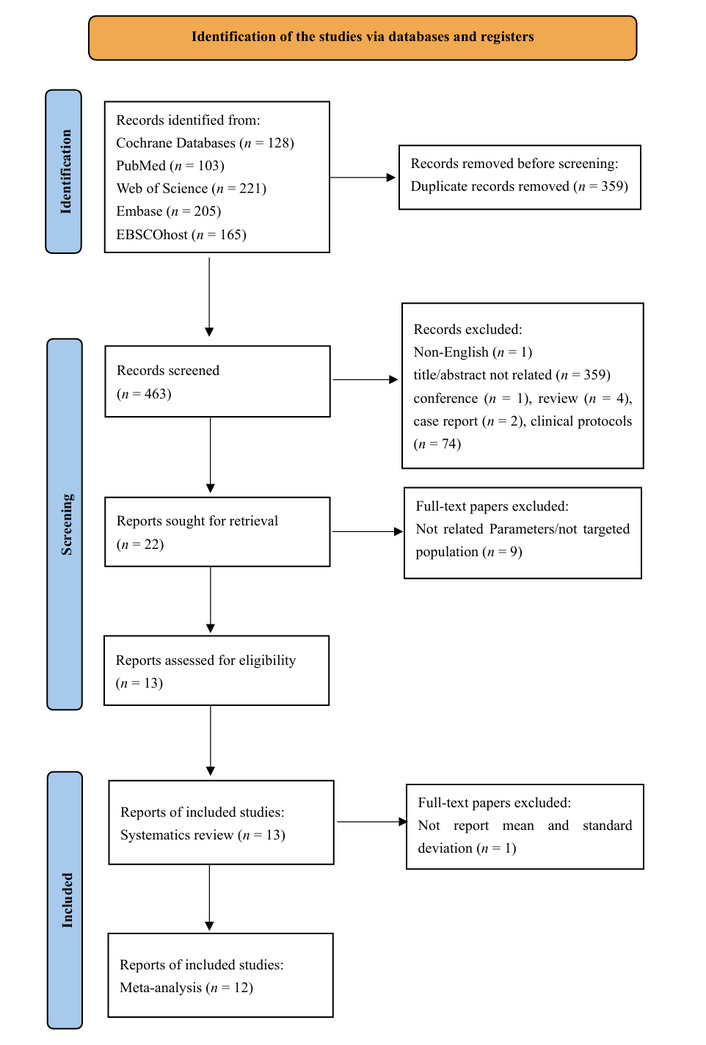
PRISMA flow diagram. Adapted from [47]. © The Author(s) 2026. Licensed under a Creative Commons Attribution (CC BY 4.0).
Thirteen studies [15, 16, 22–32] were assessed for quality. Two studies [26, 27] scored 50%, one study [32] scored 62.5%, three studies [22, 24, 31] scored 68.25%, four studies [15, 16, 25, 28] scored 75%, and three studies [23, 29, 30] scored 81.25%. Based on these scores, seven studies [15, 16, 23, 25, 28–30] were classified as high quality, six studies [22, 24, 26, 27, 31, 32] as moderate quality, and only two studies [26, 27] as low quality. All studies [15, 16, 22–32] reported poor external validity. Regarding internal validity and confounding, four studies [22, 24, 31, 32] showed low validity in items 21 and 22, one study [27] in items 21, 22, and 25, and one study [24] in item 21. Inter-rater reliability was high, with a Kappa of 0.836 (p < 0.001) (Table 2).
Quality assessment results.
| Items (Study) | Reporting | External validity | Internal validity -bias | Internal validity-confounding | Total (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 5 | 6 | 7 | 10 | 11 | 12 | 16 | 18 | 20 | 21 | 22 | 25 | ||
| Tomkins-Lane et al. 2012 [22] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 11/16 (68.75%) |
| van den Hoorn et al. 2012 [23] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 13/16 (81.25%) |
| Crosbie et al. 2013 [24] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 11/16 (68.75%) |
| Müller et al. 2015 [25] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 12/16 (75%) |
| Barzilay et al. 2016 [15] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 12/6 (75%) |
| Vickers et al. 2017 [16] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 12/16 (75%) |
| Tabard-Fougère et al. 2018 [27] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 8/16 (50%) |
| Hicks et al. 2017 [26] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 8/16 (50%) |
| Demirel et al. 2020 [28] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 12/16 (75%) |
| Jiménez-Del-Barrio et al. 2020 [29] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 13/16 (81.25%) |
| Castro-Méndez et al. 2020 [30] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 13/16 (81.25%) |
| Lee et al. 2021 [31] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 11/16 (68.75%) |
| Lin et al. 2023 [32] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 10/16 (62.5%) |
1) Is the hypothesis/aim/objective of the study clearly described? 2) Are the main outcomes described clearly? 3) Are the characteristics of participants described clearly? 5) Is the distribution of principal confounders described clearly? 6) Are the main findings described clearly? 7) Are estimates of the random variability provided? 10) Are actual probability values reported? 11) Were the participants asked to join the study representative of the entire population? 12) Were the participants preparing to participate representative of the entire population? 16) Was it clear if results were based on “data dredging”? 18) Were the statistical tests used to assess the main outcomes appropriate? 20) Were the measurements used for main outcomes accurate? 21) Were the study group and controls recruited from the same population? 22) Were the study group and controls recruited from the same period? 25) Was confounding adequately adjusted? The scoring criteria were based on the methodological quality assessment checklist proposed by Downs and Black [19].
A total of 678 participants were recruited from the thirteen studies [15, 16, 22–32] for the systematic review. 378 NSCLBP were compared to different gait parameters in the 300 healthy controls, and 168 males (NSCLBP: 98, control group [CON]: 70) and 278 females (NSCLBP: 135, CON: 143) were reported among nine studies [16, 22–26, 29–31] out of 13. Twelve studies [15, 16, 22–26, 28–32] described participants’ age, with mean ages of 46.82 years for the NSCLBP group and 44.76 years for the healthy group. Nine studies [22–26, 28–30, 32] reported pain intensity in NSCLBP patients, with a combined mean pain score of 3.85 ± 1.29. The spatiotemporal parameters of walking speed, step length, cadence, step width, stance phase, single support phase, swing phase, and stride length were selected to compare the NSCLBP and healthy controls. Six studies [15, 16, 24, 25, 28, 30] reported that patients with NSCLBP walked significantly more slowly than healthy participants. Two of these studies [15, 30] specifically found a statistically significant reduction in cadence in the NSCLBP group compared to healthy controls, with values of 107.2 ± 8.4 vs. 111.0 ± 7.1 steps/min and 107.03 ± 8.7 vs. 110.9 ± 8.8 steps/min, respectively (p < 0.05). Additionally, three studies [15, 16, 28] observed shorter step lengths in NSCLBP patients, while one study [28] reported a smaller stride length compared to healthy controls. No studies reported significant differences between NSCLBP patients and healthy participants in step width, single support phase, stance phase, or swing phase [15, 16, 22–32] (Table 3).
Characteristics of the included studies.
| Authors | Instruments | Participants | Age | Gender (M/F) | Pain intensity | Comparison | Parameters | Conclusion |
|---|---|---|---|---|---|---|---|---|
| Tomkins-Lane et al. 2012 [22] | Distance measurement instrument(Lufkin Pro-Series Model PSMW38a) | 44 NSCLBP 32 CON | NSCLBP 62.27 ± 6.70CON 66.19 ± 8.01 | NSCLBP 12/32CON 11/21 | 3.79 ± 2.43 | NSCLBP vs. CON | Stride length (m) | No. sig. |
| van den Hoorn et al. 2012 [23] | 3D motion capture | 13 NSCLBP 12 CON | NSCLBP 35.3 ± 12.4CON 32.2 ± 13.1 | NSCLBP 5/8CON 4/8 | 2.92 ± 1.48 | NSCLBP vs. CON | Walking speed (m/s) | No. sig. |
| Crosbie et al. 2013 [24] | Multi-sensor, 6-df electromagnetic tracking device | 19 NSCLBP 19 CON | NSCLBP 34 ± 13.3CON 28.6 ± 5.4 | NSCLBP 7/12CON 6/13 | 2.8 ± 2.2 | NSCLBP vs. CON | Walking speed (m/s) | Sig. |
| Müller et al. 2015 [25] | 3D motion capture | 11 NSCLBP 11 CON | NSCLBP 38.2 ± 13.9CON 38.5 ± 12.1 | NSCLBP 5/6CON 5/6 | 1.9 ± 1.2 | NSCLBP vs. CON | Walking speed (m/s); step length (m) | Sig. (walking speed), no sig. (step length) |
| Barzilay et al. 2016 [15] | Four convex biomechanical units(AposTherapy System, APOS—Medical and Sports Technologies Ltd., Herzliya, Israel) | 60 NSCLBP 24 CON | NSCLBP 53.3 ± 14CON 48.4 ± 13.1 | NA | NA | NSCLBP vs. CON | Walking speed (m/s); cadence (step/min); step length (m); single stance (%) | Sig. |
| Vickers et al. 2017 [16] | Gait mat (Gait Rite 1; CIR Systems, Inc.; Havertown, PA) | 30 NSCLBP 25 CON | NSCLBP 51.2 ± 17.9CON 31.9 ± 12.4 | NSCLBP 17/13CON 10/15 | NA | NSCLBP vs. CON | Walking speed (m/s); cadence (step/min); step length (m); step width (m); single support (%); double support (%) | Sig. (walking speed, step length), no sig. (other parameters) |
| Tabard-Fougère et al. 2020 [27] | NA | 39 NSCLBP 24 CON | NA | NA | NA | NSCLBP vs. CON | Walking speed (m/s); cadence (step/min); step length (m); stance phase (%) | No. sig. |
| Hicks et al. 2017 [26] | GaitMat IITMsystem(E.Q. Inc., Chalfont, PA) | 54 NSCLBP 54 CON | NSCLBP 69.3 ± 6.7CON 71.1 ± 6.8 | NSCLBP 17/37CON 17/37 | 3.4 ± 1.6 | NSCLBP vs. CON | Step length (m); step width (m); swing time (s); stance time (s); double support time (s) | No. sig. |
| Demirel et al. 2020 [28] | NA | 30 NSCLBP 32 CON | NSCLBP 44.80 ± 11.67CON 40.81±10.95 | NA | 3.48 ± 3.04 | NSCLBP vs. CON | Walking speed (m/s); step length (m); stance phase (%); stride length (m); swing phase (%); single support (%); double support (%); cadence (step/min) | Sig. (walking speed, step length, stride length), no sig. (other parameters) |
| Jiménez-del-Barrio et al. 2020 [29] | 16 Megapixel camera, Nikon Coolpix, model | 20 NSCLBP 20 CON | NSCLBP 24.6 ± 5.21CON 23.2 ± 5.01 | NSCLBP 5/15CON 6/14 | 5.68 ± 2.23 | NSCLBP vs. CON | Step length (m) | No. sig. |
| Castro-Méndez et al. 2020 [30] | Opto-gait photocell sensor | 20 NSCLBP 12 CON | NSCLBP 41 ± 10.7CON 28 ± 7.6 | NSCLBP 16/4CON 2/10 | 6.59 ± 0.20 | NSCLBP vs. CON | Walking speed (m/s); stride length (m); cadence (step/min) | Sig. (cadence, stride length), no sig. (other parameters) |
| Lee et al. 2021 [31] | Motion analysis system (Motion Analysis Corporation, Rohnert Park, CA, USA) | 22 NSCLBP 19 CON | NSCLBP 28.91 ± 12.80CON 27.58 ± 9.13 | NSCLBP 14/8CON 9/10 | NA | NSCLBP vs. CON | Walking speed (m/s); cadence (step/min); stride length (m); step length (m); stance phase (%); swing phase (%) | No sig. |
| Lin et al. 2023 [32] | Treadmill (FDM-T Lido, Noraxon, USA) with a deck of 2560 capacitive sensors(Myo-Pressure-T, Noraxon, USA) | 16 NSCLBP 16 CON | NSCLBP 28 ± 6.94CON 28.88 ± 7.09 | NA | 2 (1–3.5) | NSCLBP vs. CON | Stance phase (%); swing phase (%); step length (m); stride length (m); step width (m); walking speed (m/s); cadence (step/min) | No. sig. |
CON: control group; NA: not applicable; No sig.: no significance; NSCLBP: non-specific chronic low back pain.
Ten studies [15, 16, 23–25, 27, 28, 30–32] out of twelve compared walking speed between the NSCLBP and healthy controls (Figure 2), and the meta-analyses with the random effects model revealed significant overall effects of walking speed between the NSCLBP and the healthy controls (SMD = –0.67, 95% CI: –1.08 to –0.25, p = 0.002).
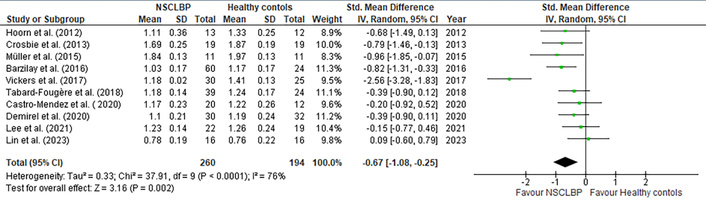
Forest plots of walking speed comparing non-specific chronic low back pain (NSCLBP) patients and healthy controls.
Six studies [15, 16, 27–29, 32] out of twelve reported the comparison step length between the NSCLBP and healthy controls (Figure 3), and the meta-analyses with the random effects model revealed significant overall effects of step length between the NSCLBP and the healthy controls (SMD = –0.55, 95% CI: –0.94 to –0.17, p = 0.004).
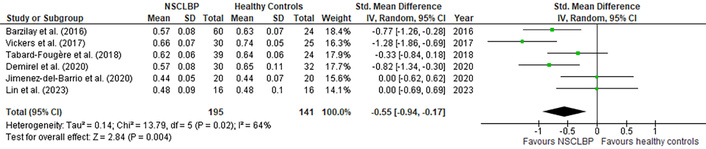
Forest plots of step length comparing non-specific chronic low back pain (NSCLBP) patients and healthy controls.
Six studies [15, 16, 27, 30–32] out of twelve reported the comparison cadence between the NSCLBP and healthy controls (Figure 4), and the meta-analyses with the random effects model revealed no significant overall effects of cadence between the NSCLBP and the healthy controls (SMD = –0.29, 95% CI: –0.62 to 0.04, p = 0.09).
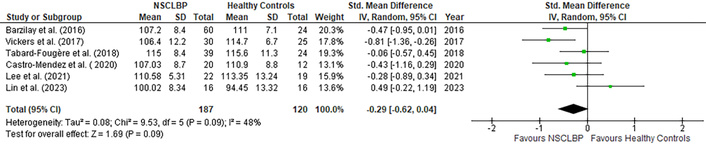
Forest plots of cadence comparing non-specific chronic low back pain (NSCLBP) patients and healthy controls.
Three studies [16, 31, 32] out of twelve reported the comparison step width between the NSCLBP and healthy controls (Figure 5), and the meta-analyses with the random effects model revealed no significant overall effects of step width between the NSCLBP and the healthy controls (SMD = 0.27, 95% CI: –0.14 to 0.68, p = 0.20).

Forest plots of step width comparing non-specific chronic low back pain (NSCLBP) patients and healthy controls.
Five studies [15, 27, 28, 31, 32] out of twelve reported the comparison stance phase between the NSCLBP and healthy controls (Figure 6), and the meta-analyses with the random effects model revealed no significant overall effects of stance phase between the NSCLBP and the healthy controls (SMD = 0.20, 95% CI: –0.18 to 0.58, p = 0.30).

Forest plots of stance phase (%) comparing non-specific chronic low back pain (NSCLBP) patients and healthy controls.
Four studies [15, 16, 28, 32] reported the single support phase, three studies [28, 31, 32] presented the swing phase and four studies [22, 28, 30 31] described the stride length, and the meta-analyses with random effects model revealed no significant overall effects of single support phase (SMD = –0.17, 95% CI: –0.60 to 0.25, p = 0.42), swing phase (SMD = 0.19, 95% CI: –0.28 to 0.66, p = 0.43) and stride length (SMD = -0.01, 95% CI: -0.36 to 0.33, p = 0.94) between the NSCLBP and the healthy controls (Figure 7).
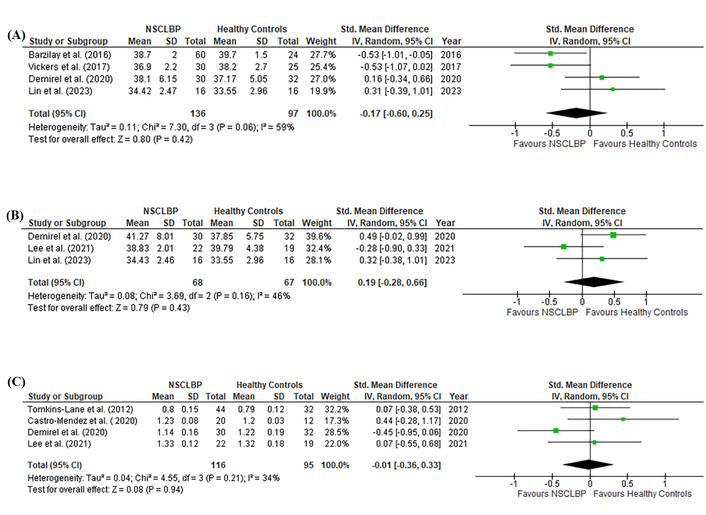
Forest plots of (A) single support phase (%), (B) swing phase (%) and (C) stride length (m) comparing non-specific chronic low back pain (NSCLBP)patients and healthy controls.
The meta-analysis revealed a significantly reduced walking speed (ES = 0.67) and step length (ES = 0.55) compared to healthy controls. Meanwhile, NSCLBP patients showed smaller cadence (ES = 0.29), bigger step width (ES = 0.27), and shorter stance phase (ES = 0.20) when compared to the healthy controls. Furthermore, no evidence was found to suggest changes in the single support phase, swing phase, and stride length among NSCLBP patients compared to healthy participants. Higgins’ I2 statistics revealed low heterogeneity (26–46%) for spatiotemporal parameters such as cadence, step width, stride length, and swing phase. Moderate heterogeneity (57–64%) was observed for the single support phase, stance phase, and step width, while walking speed demonstrated high heterogeneity (76%). Therefore, caution is advised when interpreting walking speed in NSCLBP patients.
Walking speed, an essential spatiotemporal parameter, is calculated via distance divided by displacement time. In this review, ten out of twelve studies investigated walking speed. Five studies [15, 16, 24, 25, 28] reported that NSCLBP patients walked significantly slower (1.03 m/s to 1.84 m/s) compared to healthy participants (1.17 m/s to 1.97 m/s). However, another five studies [23, 27, 30–32] found no significant difference in walking speed between the two groups. The potential causes of these differences can be attributed to multiple factors, including pain intensity, gender, age, body weight, muscle inhibition, restricted trunk-lower limb flexibility, and other variables.
Pain severity is a factor that may influence walking speed. Cross-sectional studies comparing NSCLBP patients with age- and gender-matched healthy controls normalized gait velocity by accounting for stride length, body weight, and stride time, and the findings revealed that NSCLBP patients with higher pain intensity tend to walk at a slower pace [33]. Therefore, pain intensity may be a potential factor contributing to the variability in walking speed. This evidence is further supported by an observational study that compared muscle activation between NSCLBP patients and healthy controls [34]. The study found that NSCLBP patients tend to exhibit reduced muscle activation during voluntary contractions, particularly in muscles such as the lumbar multifidus, knee extensors, and hip extensor muscles. The decreased activation of these key muscle groups may contribute to limited knee and hip extension, which in turn could impair overall gait mechanics. This reduction in muscle function may restrict the range of motion and efficiency of movement, ultimately leading to a slower walking speed in patients with NSCLBP. Thus, the compromised muscle activation observed in NSCLBP patients may play a significant role in the altered gait patterns and reduced mobility seen in this population.
Gender is a recognized factor influencing walking speed, with females typically walking slower than males. A descriptive meta-analysis highlighted differences in walking speed across sexes and age groups, reporting preferred walking speeds ranging from 0.97 to 1.43 m/s for males and 0.94 to 1.39 m/s for females [35]. Ayis et al. [36] observed that healthy women aged 35 to 44 years had an average walking speed of 1.26 m/s (95% CI: 1.19–1.34), while men in the same age group averaged 1.35 m/s (95% CI: 1.28–1.42). Therefore, gender should be considered when evaluating walking speed in NSCLBP patients. In this review, all studies included male and female participants, which may influence the consistency of findings. Additionally, walking speed may be affected by age. One study categorized participants into young (below 30 years), middle-aged (31–45 years), and older adults (above 45 years) and found that walking speed decreases with age [37]. Similarly, Hageman [38] also reported a declining trend in walking speed with ageing, with averages of 1.76 m/s (age 39.2 ± 12.6), 1.60 m/s (age 61.5 ± 3.4), and 1.39 m/s (age 74.7 ± 6.6).
This review reported walking speeds ranging from 1.03 m/s to 1.84 m/s in NSCLBP patients aged 20 to 60 and from 1.17 m/s to 1.97 m/s in healthy individuals. Notably, the fastest walking speed was 1.97 m/s in healthy participants and 1.84 m/s in NSCLBP patients aged 20 to 40 years [25], exceeding previously reported values for females (1.34 m/s) and males (1.42 m/s). In Müller et al.’s [25] study, participants were allowed to select their walking and running speeds, which may account for differences in walking speed on level ground compared to earlier findings. It is also important to consider that walking speed variability could be influenced by factors such as measurement devices, walking conditions, individual muscle strength, and other variables [25]. Therefore, while evidence suggests that walking speed is significantly reduced in NSCLBP patients compared to healthy controls, these findings should be interpreted with caution. Nevertheless, this finding is clinically significantly important for clinicians to address the issue during rehabilitation.
The linear distance from the heel of one foot to the heel of the opposite foot is a sensitive parameter commonly used to evaluate gait patterns in NSCLBP patients. In this review, step length ranged from 0.44 m to 0.66 m in NSCLBP patients and from 0.44 m to 0.74 m in healthy controls [15, 16, 27–29, 32]. NSCLBP patients typically exhibit shorter step lengths compared to healthy controls [15, 16, 27, 28], which may be attributed to reduced pelvic rotation in the horizontal plane. This restriction is often associated with shortened hip flexors, causing anterior pelvic tilt [39], which limits the pelvic rotation required for achieving larger step lengths [40]. Additionally, pain in the lower back may contribute to reduced step length. NSCLBP patients often decrease lumbar and pelvic movement to minimize pain, further restricting step length [41]. However, two studies [29, 31] found similar step lengths in NSCLBP patients and healthy controls. It is worth mentioning that these studies primarily involved younger participants aged 20 to 30 years, which may explain the less pronounced changes in step length despite back pain persisting for over three months.
This meta-analysis suggests no significant differences in cadence between NSCLBP patients and healthy controls, although a small ES indicates a decreasing trend. Cadence, defined as the number of steps per minute, is influenced by walking speed and stride length. Most evidence indicates that NSCLBP patients tend to decrease cadence during walking tasks [15, 16, 24, 27, 31], likely as a strategy to minimize pain irritation. For instance, NSCLBP patients often take longer to complete walking tasks with reduced step frequency, reflecting an adaptive strategy to avoid discomfort. A cross-sectional study observed that NSCLBP patients had a longer cadence duration (132.90 ± 39 s) compared to healthy controls (122.18 ± 21.91 s), suggesting fewer steps per minute [28]. This trend toward a slower cadence highlights an effort by NSCLBP patients to reduce pain while walking. The reduction in cadence may serve as a compensatory mechanism, where patients prioritize minimizing discomfort over maintaining normal gait patterns. Overall, while cadence differences between NSCLBP patients and healthy controls are subtle, the observed trends underscore the importance of considering cadence as a key factor when assessing gait adaptations and pain management strategies in NSCLBP patients.
This systematic review and meta-analysis revealed significant alterations in the spatiotemporal gait parameters of NSCLBP patients, particularly reductions in walking speed, step length, and cadence. However, no significant differences were observed between NSCLBP patients and healthy controls in parameters such as step width, stride length, stance phase, single support phase, and swing phase. Despite this, trends toward specific gait adaptations, including increased stride width, were noted. NSCLBP patients tended to have wider stride width, which may reflect an unconscious strategy to reduce excessive load on the affected leg during pain episodes. A wider stride width may help distribute weight evenly between both legs, facilitating balance and reducing strain on the painful side. Additionally, previous studies have reported that stride width increases with age [42]. Including participants aged 20 to 60 years in this meta-analysis could contribute to inconsistencies in the findings. Regarding another spatial parameter, this review found no significant differences in stride length between NSCLBP patients and healthy controls. Research indicates that trunk-pelvis rotation amplitude plays a crucial role in influencing stride length during gait [43]. NSCLBP patients often have tight hip flexors, trunk extensors, and lumbar rotators, limiting trunk-pelvis movement toward the symptomatic side and affecting stride length. However, compensation may be achieved by increasing the stride length on the unaffected side. Notably, included studies did not report stride length for the affected side, possibly explaining the absence of detectable differences in this analysis.
In this review, the standing phase also showed an increasing trend; however, the single support and swing phases were not detectable in the gait adaptation of the NSCLBP patients. The stance phase begins with the heel initially contacting the ground and concludes when the foot toes off [32]. The single support phase is when only one foot is in contact with the ground while the other leg swings [44]. The swing phase is when one leg is off the ground and moving forward to take the next step [45]. Patients with NSCLBP were usually reported with a rigid lumbar-pelvic region due to pain disturbance [46], notably reduced hip-lumbar extension. This stiffness makes generating forward motion during the transition from the stance phase to the swing phase more challenging. Consequently, patients may extend the stance phase to stabilize the body for longer durations, reducing the reliance on the hip and lumbar regions for forward propulsion during the swing phase. Additionally, as single support and swing phases are brief and transitional within the gait cycle, an increased stance phase may maintain a normal single support duration without significant observable adaptations. This could explain why single support and swing phases were not distinctly detected in this review. Moreover, the influence of pain intensity on specific gait phases, such as the single support and swing phases, requires further investigation to understand its impact comprehensively.
In conclusion, this systematic review and meta-analysis found moderate evidence that patients with NSCLBP exhibit significantly slower walking speed and shorter step length compared to healthy controls. These findings suggest a distinct clinical alteration in walking pattern that should be targeted during rehabilitation to improve functional outcomes. However, other spatiotemporal parameters—including cadence, step width, stride length, phase timings-showed high variability across studies due to clinical and methodological differences. As these findings are specific to NSCLBP, their generalizability to other types of low back pain remains uncertain. Future high-quality studies are warranted to explore multidimensional gait variability, assess the impact of pain intensity, and examine gait characteristics across diverse low back pain populations.
This review employed a comprehensive search strategy and a two-reviewer screening process, adhered to PRISMA guidelines, and included a quantitative synthesis using meta-analysis. Therefore, the results provide robust evidence supporting and explaining the differences in walking patterns between individuals with NSCLBP and healthy controls.
However, this review has several limitations that warrant attention. First, the study focuses solely on spatiotemporal parameter changes to summarize gait characteristics and does not incorporate other kinematic parameters, such as joint angles in the sagittal, frontal, and transverse planes, or kinetic data on force generation during different gait phases. Consequently, the high heterogeneity observed in walking speed and step length may reflect unmeasured variability in these additional gait dimensions, limiting the generalizability of the pooled results. Second, the severity of pain, a critical factor influencing spatiotemporal gait parameters, was not addressed. Differences in pain intensity may further contribute to the observed variability and warrant further investigation. Finally, this systematic review and meta-analysis exclusively examined gait variability in patients with NSCLBP, so the applicability of these findings to other types of low back pain remains uncertain.
CI: confidence interval
CON: control group
ES: effect size
NSCLBP: non-specific chronic low back pain
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
SMD: standardized mean difference
WOS: Web of Science
JG: Conceptualization, Data curation, Formal analysis, Methodology, Software, Validation, Visualization, Writing—original draft. KWG: Validation, Visualization, Writing—review & editing. JST: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing—review & editing. SW: Validation, Visualization, Writing—review & editing. JG: Validation, Visualization, Writing—review & editing. FMJ: Validation, Visualization, Writing—review & editing. CSC: Validation, Visualization, Writing—review & editing. All authors read and approved the submitted version.
All authors declare that they have no conflicts of interest with respect to the research, authorship, and/or publication of this article.
This project was supported by the University Putra Malaysia Research Ethics Committee (JKEUPM-2021-856), and the National Sports Institute of Malaysia Research Ethics Committee (ISNRE/A/002/2022-009/2021).
Not applicable.
Not applicable.
The primary data for this systematic review were sourced online from databases listed in the methods. Referenced articles are accessible on Cochrane, PubMed, Web of Science (WOS), Embase, and EBSCOhost. Additional supporting data are available from the corresponding author upon request.
This work was funded by the National Sports Institute of Malaysia (ISNRG No. 008/2021-009/2021). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 1761
Download: 24
Times Cited: 0
