Case Report
Case Report

Affiliation:
Department of Orthopaedic Surgery, Tan Tock Seng Hospital, Singapore 308433, Singapore
Email: jason.chia@nhghealth.com.sg
ORCID: https://orcid.org/0009-0007-2485-8553
Explor Musculoskeletal Dis. 2026;4:1007123 DOI: https://doi.org/10.37349/emd.2026.1007123
Received: October 10, 2025 Accepted: April 06, 2026 Published: May 08, 2026
Academic Editor: Fernando Pérez-Ruiz, Cruces University Hospital, Spain
The popliteus is a thin, flat, triangular muscle that originates from the lateral condyle of the femur and inserts on the posterior surface of the tibia and soleal line. Injury to the popliteus musculotendinous unit is an infrequent cause of posterolateral knee pain. This can result from a traumatic event or as a result of cumulative overload. This report describes posterior knee pain from a popliteal injury that resulted from an unusual low-velocity mechanism while performing a dance movement, which can be easily missed. Clinical and ultrasonographic features that lead to the diagnosis are described. The patient was able to return to dancing after physical rehabilitation and adjustment to dance technique. The report provides an account of popliteus injury through an unusual mechanism and treatment that can aid the clinician in the diagnosis and management of popliteus injury.
Injury to the popliteus is an uncommon cause of posterior knee pain and is typically a result of a high-velocity trauma or repetitive overuse in sports. This report describes the mechanism of injury and diagnostic features of a low-velocity injury in dance that might otherwise be missed, and also presents technical corrections for the prevention of this injury.
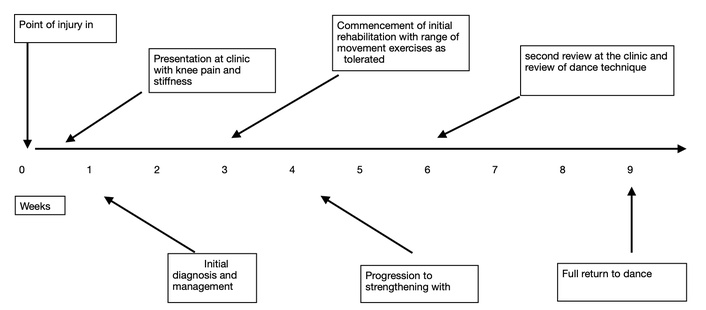
The patient sustained the injury on Day 0 during a dance activity, with immediate onset of pain and functional limitation. Clinical evaluation and initial imaging were performed within 72 hours, followed by initial management with anti-inflammatories. Conservative management was initiated at 3 weeks post-injury. Progression to body weight exercise was instituted at Week 4. Review of the dance techniques was by 6 weeks, and full return to pre-injury activity by 9 weeks. The timeline is represented in Figure 1.
The patient was a recreational dancer with no past medical history who presented with left posterolateral knee pain soon after performing a contemporary dance manoeuvre from a standing position into a seated position on the ground. The pain was initially mild and was rated between 2 and 3 on the visual analogue scale (VAS). The patient subsequently experienced progressive pain and tightness in the back of the knee during knee movement in class. This was accentuated when sitting with the left shin crossed over the right knee on the same day, as well as posterior knee tightness at the end of the stance phase while walking, rated 5–6 on VAS. He decided to seek medical attention on the third day of injury as the symptoms impeded his return to dance.
On examination, pain was felt most acutely on palpation of the lateral popliteal fossa. Range of motion was 0–150 degrees vs 0–130 on the contralateral knee. Manual muscle testing (MMT) of knee flexion showed power of 4 out of 5 on the injured knee versus full power on the contralateral knee. The lateral joint line, collateral ligament, lateral head of the gastrocnemius, and biceps femoris tendon were not tender. Of note was the full range of movement and the absence of effusion. Varus stress test, Cabot test for snapping popliteus tendon, Dial test for posterolateral instability, and McMurray and Apley grind tests were negative. Garrick’s test for popliteus injury was positive and reproduced the posterolateral knee pain.
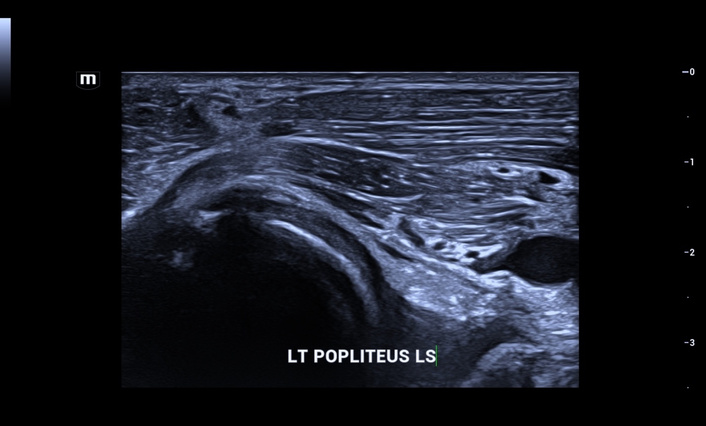
On bedside ultrasound scan, the popliteus tendon was intact in the popliteal groove, while the muscular portion showed disruption of superficial fibres and an overlying haematoma (Figure 2). Sonopalpation over the popliteus reproduced the patient’s symptoms, which suggests a popliteus injury as one of the causes of his symptoms. A working diagnosis of a second-degree strain to the popliteus was made.

Ultrasound image in long axis with the popliteus with discontinuity of the muscle fibres (white asterisk). The tendinous portion is intact (white arrow).
The second-degree strain was managed with anti-inflammatories and cryotherapy for the first week to reduce pain. Range of motion exercises were prescribed with supine heel slides in the first week, followed by seated knee extensions in the second week to reduce stiffness. These were performed in repetitions of 10–20, 3–4 times a week. The pain reduced to 4 on the VAS scale after three weeks, allowing progression to strengthening exercises. Range of movement showed slight improvement (0–120 degrees). Knee flexion strength on the affected knee remained at 4 out of 5. Strengthening of the quadriceps, hamstrings, and popliteus using resistance bands was initiated by the third week with seated hamstring curls and standing resisted terminal knee extension and prone internal rotation at 90 degrees of knee flexion, each performed 3 sets of 10 repetitions daily, and then progressed to weight-bearing exercises. The popliteus was strengthened with standing tibial internal rotation against resistance with the left knee flexed. Split squats and single-leg bridging were prescribed (3 sets of 10 repetitions) for strengthening of the quadriceps, gluteal, and hamstring muscles. Rehabilitation progressed to dance-specific strengthening such as plié-based exercises with attention to maintaining turnout as well as parallel passé to turnout to improve hip rotation control. Stretches in the frog pose and the pigeon pose were prescribed to improve hip range of movement, particularly in external rotation and flexion.
On review in six weeks, the patient reported resolution of pain on activities of daily living. The popliteus was non-tender, and Garrick’s test was negative. MMT showed symmetrical strength of both knees, and knee flexion was 130 degrees bilateral. Ultrasound examination confirmed resolution of the hypoechogenicity of the muscle defect consistent with resorption of the haematoma and interval healing of the popliteus muscle, evinced by restoration of the continuity of the muscle fibres. Of note was the absence of structural alterations compared to the surrounding muscles (Figure 3). A review of the movement that caused the injury was performed with a physiotherapist familiar with dance, beginning with slow controlled transitions to the ground with support from the barre, followed by unsupported transitions. The patient was able to perform the provocative dance manoeuvre asymptomatically in the clinic.
Ultrasound image in long axis with the popliteus at 6 weeks follow-up with restoration of the architecture of the muscle.
The patient reported satisfaction with the rehabilitation process. In particular, he found the incorporation of dance-specific conditioning as well as dance technique correction instrumental in facilitating his return to dance confidently. In particular, correcting the timing of the weight shift between both legs and the degree and timing of the external rotation of the hips permitted a smoother transition to the ground. This, in conjunction with adequate ankle plantar flexion, reduced torque on the knees. Discussion with the dance instructor, familiar with the participant, also confirmed that the revised movement was technically better and closer to that performed by the other dancers in movements with transitions to the floor. Upon review in nine weeks, he was able to fully participate in dance classes without difficulty or pain. The timeline of the clinical events is presented before.
Isolated injury to the popliteus is uncommon and occurs predominantly in the muscular portion [1]. Injury can occur through an acute traumatic event or with cumulative overload from downhill walking and running [2]. To our knowledge, the injury to the popliteus as a result of a low-velocity injury in contemporary dance has yet to be described.
The popliteus is unique in that it has a muscular distal insertion on the posterior tibia and a tendinous proximal origin from the lateral femoral condyle [3]. The tendon is intra-capsular, although extra-articular and extra-synovial [4].
It serves an important function in the screw home mechanism of the knee by rotating the tibia internally on the femur when standing. It externally rotates the femur on the leg and unlocks the knee, hence initiating flexion of the knee. It is a primary internal rotator of the tibia in the non-weight-bearing state and resists external rotation of the tibia on the femur with a flexed knee [4]. This is pertinent to the mechanism of injury described below [5].
The popliteus can be injured by direct blows to the anteromedial knee with varus forces on the flexed knee, as well as hyperextension to the knee in non-contact injuries [6]. The musculotendinous junction is susceptible to injury, being the weakest part of the muscle [7]. Some authors opine that the mechanism of non-contact injury is not always discernible nor fully understood [8]. Other causes of posterolateral knee pain to consider include biceps femoris tendinopathy, calf strain, posterior lateral corner injury, and popliteus strain and tendinopathy.
The proposed mechanism of injury is depicted in Figure 4. The injuring manoeuvre in question begins in a forward lunging position to the right. The weight mainly on the right leg, with the left knee flexed and the left hip extended behind and internally rotated (left picture). As the body pivots to the left and the weight shifts towards the left, the left knee rests on the ground, and the shin begins swivelling on the ground and experiences external rotation torque with reference to the thigh (middle picture). Finally, the left hip is fully externally rotated. The shin completes swivelling on the ground. The shin experiences internal rotation torque with reference to the thigh. The movement is completed by resting in a seated position with the left hip flexed and externally rotated and the knee fully flexed (right picture).

Sequential images (from left to right) demonstrating the mechanism of injury from Phase 1: initial lunge (left picture), to Phase 2: pivot and weight transfer (middle picture), and Phase 3: seated position (right picture).
Injury to the popliteus may potentially occur from technical errors in executing this manoeuvre. If the weight is prematurely shifted to the left leg in the first phase while the body is beginning to pivot towards the left, before the hip has time to externally rotate and the left knee to rest on the ground, the tibia is torqued in external rotation on the femur. This, along with active knee flexion, places eccentric load on the popliteus muscle. This is exacerbated if the ankle is not fully plantar flexed, obstructing the shin from a smooth external rotation on the thigh.
Injury may also occur in the later phase after the body has pivoted to the left, with excessive transfer of weight to the left shin before the knee is adequately flexed. This creates a moment arm between the shin and the thigh with the knee as the pivot, placing varus and rotatory stresses on the posterolateral corner of the knee. Insufficient range in external rotation of the hip joint may also place additional torque on the knee joint.
Novice dancers unfamiliar with this manoeuvre should familiarise themselves with the correct timing of weight shift and the sequence of movement with support from a barre to reduce loading on the knee. Other potential measures include improving hip range of movement and gluteal strength, drills to improve neuromuscular control in floor transitions, and a gradual increase in loading over a few weeks with gradually reduced reliance on the barre, although further research is necessary to empirically support these preventive measures.
Due to the low-impact nature of the trauma and the split-second execution of the manoeuvre, the injury might go unrecognised, particularly if clinicians are unfamiliar with contemporary dance techniques or do not routinely test for popliteus injury. Localised tenderness of the lateral popliteal fossa and pain elicited on resisted external rotation of the lower leg with the flexed knee (Garrick’s test) in the absence of effusion and joint line tenderness suggest popliteal injury, which can be confirmed with imaging studies.
There are few ultrasonographic reports on injuries to the muscular portion of the muscle, a reflection of its relative inaccessibility compared to the tendon. This report demonstrates that bedside ultrasound is a useful modality for diagnosing popliteus injury. The tendon is easily located in the transverse axis in the popliteal at the lateral side of the knee and followed in the longitudinal plane to locate the discontinuity and oedema of the fibres in the muscular portion of the muscle to differentiate a tear from popliteal tendinopathy [4]. Sonopalpation to localise the pain aids in diagnosis. In this particular report, the contrast between the hypoechoic haematoma and disruption of the injured muscle fibres, with the adjacent intact gastrocnemius, aids in localisation of the injury. Serial ultrasound scans allowed for confirmation of resolution of haematoma and muscle healing in the clinic and helped guide the decision to return to dance. Further imaging with an MRI scan may be warranted to assess concomitant injuires ot he postero-lateral corner complex and the posterior horn of the lateral meniscus if the diagnosis is in doubt.
Partial tears of the popliteus can be managed conservatively with good long-term results [6, 7]. Complete tears are best managed with direct repair in an acute presentation or reconstruction of chronically injured structures [9, 10].
The unusual mechanism of injury through dance and the correlation between clinical and ultrasonographic features have not been described in the literature. A limitation is the exploratory nature of the biomechanical interpretation of the mechanism of injury.
The proposed injury mechanism and associated prevention strategies should be interpreted as hypothesis-generating rather than definitive evidence-based conclusions. Prospective studies would be necessary to validate these hypotheses.
A limitation in this report is the narrative nature of the outcome measures. Future prospective research would benefit from incorporating validated functional assessment tools to allow more objective evaluation of recovery and facilitate comparison across studies. Further research with larger numbers will be necessary to elucidate the prevalence and risk factors of this injury in dancers. In particular, the influence of hip range of movement and gluteal strength might have a bearing on the risk of this injury, and the prevalence may differ between genres of contemporary dance with different stylistic demands. Other possible pertinent factors include fatigue, training volume, and general flexibility. Another limitation is the absence of an MRI to exclude differential diagnosis with similar symptoms, such as postero-lateral corner injuries and posterior horn tears. As such, the injury to the subject cannot be definitively isolated to the popliteus strain alone.
In summary, isolated popliteus injury as a cause of posterior knee pain following a low-velocity dance injury is poorly recognised. A high index of suspicion and recognising the mechanism of injury in dance, reproducing the symptoms on examination, are important for diagnosis. A bedside ultrasound is a useful adjunct to confirming the diagnosis. Further imaging with an MRI can be useful in excluding injuries to the structures of the postero-lateral corner of the knee. Examination of the biomechanics behind the dance manoeuvre may provide dance educators and dance physiotherapists with a framework to arrive at a working hypothesis on the mechanism of action. It also provides avenues for further research into interventions that can potentially prevent these injuries, such as through screening of dancers for readiness to perform this floor-based movement and through the correction of technical faults.
MMT: manual muscle testing
VAS: visual analogue scale
JKKC: Conceptualization, Data curation, Investigation, Methodology, Writing—original draft, Writing—review & editing, Visualization, Supervision, Project administration. The author read and approved the submitted version.
The author declares that he has no conflicts of interest.
This case report was reviewed by the National Healthcare Group Ethics Committee (Domain D) Institutional Review Board (IRB) and was granted exemption from formal ethics approval (Reference No: 2022/00602). The study complies with the 2024 version of the Declaration of Helsinki.
Informed consent to participate in the study was obtained from the participants.
Informed consent to publication was obtained from relevant participants.
The datasets supporting the findings of this study are available from the corresponding author upon reasonable request.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 1748
Download: 19
Times Cited: 0