 Perspective
Perspective

Affiliation:
Barts and The London School of Medicine and Dentistry, Queen Mary University of London, E1 2AD London, UK
Email: tuan.pham@qmul.ac.uk
ORCID: https://orcid.org/0000-0002-4255-5130
Explor Med. 2026;7:1001413 DOI: https://doi.org/10.37349/emed.2026.1001413
Received: October 17, 2025 Accepted: May 12, 2026 Published: June 11, 2026
Academic Editor: Gabriele Cervino, Messina University, Italy
Artificial intelligence (AI) is transforming clinical decision-making across cranio-maxillofacial trauma, oral health, and systemic disease. These domains are increasingly recognised as biologically and clinically interconnected, yet they are often studied and managed independently. This perspective introduces the concept of an integrative triangle linking facial trauma, oral health, and systemic disease, with AI serving as the computational bridge that enables cross-domain modelling and coordinated care. AI applications within this framework include imaging-based fracture detection, patient-specific implant design, automated oral disease diagnosis, multimodal risk prediction, and longitudinal outcome modelling. By integrating imaging, clinical, laboratory, and behavioural data, AI can identify shared inflammatory and metabolic pathways influencing trauma recovery and chronic disease progression. This closed-loop paradigm supports continuous learning, allowing outcomes in one domain to inform prediction and intervention in the others. The integrative triangle provides a translational roadmap for precision medicine, moving from isolated prediction toward coordinated prevention and intervention. Future development will require multimodal data integration, prospective validation, and responsible governance to ensure explainable and equitable AI deployment. This framework positions facial trauma and oral health as central components of systemic precision medicine and highlights AI as a catalyst for integrated, patient-centred care.
Artificial intelligence (AI) has progressed from theoretical exploration to practical implementation across medicine and dentistry. In cranio-maxillofacial (CMF) surgery, AI-based systems can segment complex anatomy, detect fractures, assist virtual surgical planning, and design patient-specific implants (PSIs) [1]. In dentistry and oral pathology [2, 3], algorithms classify caries, periodontal disease, and malignant transformation with accuracy comparable to expert clinicians. Concurrently, extensive evidence links oral health with systemic disorders such as diabetes, rheumatoid arthritis, obesity, and cardiovascular disease, underscoring the role of the oral cavity as a diagnostic window into general health [4, 5].
Despite these advances, research and clinical practice often remain fragmented. Trauma management, oral health, and systemic disease are treated as separate entities. The concept of an integrative triangle, with these three domains as its vertices, reframes patient care as a continuum. AI serves as the central connective layer, synthesising multimodal data from imaging, clinical records, laboratory findings, and sensor streams to support holistic decision-making [6]. Figure 1 illustrates the conceptual framework of the integrative triangle, highlighting how AI operates as the central link that combines facial trauma, oral health, and systemic disease into a cohesive, data-driven model of precision care.
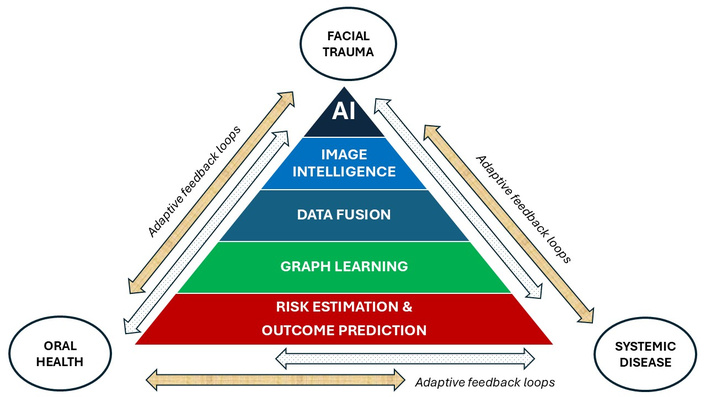
The integrative triangle. The three domains (facial trauma, oral health, and systemic disease) are linked through continuous, bidirectional interactions that support coordinated patient care. For each pair of domains, one bidirectional arrow represents direct biological and clinical interactions, such as inflammatory, metabolic, and healing-related pathways shared across domains. The second bidirectional arrow denotes artificial intelligence (AI)-enabled feedback loops, through which imaging findings, clinical data, and outcomes are integrated to support image intelligence, data fusion, graph learning, and personalised risk estimation and outcome prediction. This closed-loop structure connects acute trauma management with longer-term oral and systemic health processes, allowing outcomes in one domain to iteratively inform monitoring, planning, and intervention in the others.
This framework emphasises that oral inflammation, systemic disease, and facial trauma recovery are biologically and computationally interconnected. Chronic inflammatory pathways originating in the oral cavity can influence systemic metabolic and vascular regulation, while systemic dysregulation affects bone healing and infection risk in craniofacial trauma. AI can provide a scalable means to model these bidirectional interactions through multimodal data fusion, enabling cross-domain prediction and the identification of shared mechanistic signatures that guide integrated prevention and treatment strategies.
While existing multidisciplinary or multimodal AI approaches typically focus on aggregating heterogeneous data to improve disease-specific prediction, the integrative triangle advances this paradigm by explicitly modelling the dynamic interactions between facial trauma, oral health, and systemic disease. The framework is structured as a bidirectional and closed-loop system in which data, predictions, and outcomes continuously inform one another across domains. AI can operate as the adaptive mechanism that captures feedback between acute surgical events and chronic inflammatory or metabolic processes, thereby linking short-term trauma management with long-term systemic health trajectories. This closed-loop configuration distinguishes the integrative triangle from static multimodal frameworks and establishes a unified model for integrating acute and chronic care through adaptive AI feedback.
CMF trauma often presents with complex fracture geometries that challenge manual interpretation. Deep learning models trained on computed tomography (CT) or cone beam CT (CBCT) can identify fracture lines, quantify displacement, and generate structured diagnostic outputs. Integration of computer vision with natural language processing (NLP) applied to clinical notes can allow prioritisation of urgent cases and automated triage [7]. Such applications accelerate decision-making and improve equity of access in high-volume emergency environments.
AI-driven segmentation and reconstruction underpin virtual surgical planning. Generative and reinforcement learning models create PSIs with geometry optimised for anatomical and biomechanical fit [8]. Surrogate models trained on finite element simulations predict fixation stability, supporting preoperative design refinement [9]. Virtual simulation of osteotomies and implant positioning can enhance surgical preparedness and patient communication [10].
Predictive modelling that integrates imaging features with systemic parameters enables personalised surgical planning [11]. Multimodal algorithms can estimate infection risk, wound complications, or revision probability [12]. Such models link trauma severity to systemic context, allowing targeted antibiotic prophylaxis and tailored postoperative care.
AI is increasingly integrated into dental implant planning and digital workflows [13, 14], supporting precision-driven treatment planning and patient-specific reconstruction. These developments are closely aligned with advances in CMF trauma management, where similar imaging, modelling, and design pipelines are used for PSIs and surgical planning. The integration of AI into implant dentistry, therefore, represents an important component of the broader integrative triangle, linking structural reconstruction, oral health, and systemic considerations within precision medicine frameworks.
AI-driven analysis of CBCT and intraoral imaging enables automated identification of anatomical landmarks, bone morphology, and critical structures such as the inferior alveolar nerve and maxillary sinus [15–17]. Machine learning models have been developed to evaluate bone quality, detect anatomical variations, and assist in determining optimal implant positioning. These automated tools can improve planning consistency, reduce operator variability, and support risk assessment, particularly in complex anatomical or trauma-related reconstruction cases.
In CMF trauma, similar AI-based segmentation and anatomical modelling approaches are used to assess fracture patterns and reconstruct osseous defects [18]. The convergence of these techniques highlights the shared computational foundation between implant dentistry and trauma reconstruction, reinforcing the role of AI in patient-specific surgical planning.
As AI-assisted implant planning increasingly incorporates prosthetically driven workflows, implant positioning can be guided by functional and restorative considerations [19]. Integration of CBCT data with intraoral scanning and digital prosthetic design can enable virtual simulation of implant placement, occlusal alignment, and biomechanical loading conditions. Generative and optimisation algorithms can support automated implant positioning that accounts for anatomical constraints, prosthetic requirements, and biomechanical stability [20–22].
These virtual planning environments parallel those used in CMF trauma reconstruction, where AI-assisted simulation supports osteotomy planning, fixation design, and PSI development [6, 23]. The shared reliance on multimodal imaging and computational modelling further supports the integrative triangle framework by linking structural reconstruction with oral functional outcomes.
AI-enhanced digital workflows extend from preoperative planning to guided surgical execution. Digital surgical guides generated from AI-assisted planning can improve placement accuracy and reduce intraoperative variability. Additionally, automated workflow integration between imaging, planning software, and manufacturing platforms supports streamlined clinical pathways and reduced planning time [24].
In trauma reconstruction, similar digital workflows are applied to PSI fabrication and surgical guide production. These parallel developments demonstrate how AI-enabled digital workflows can unify implant dentistry and CMF reconstruction within a common precision-surgery ecosystem.
AI-based predictive models have also been applied to implant stability prediction, osseointegration assessment, and complication risk estimation [25, 26]. By integrating imaging features, patient-specific clinical data, and systemic health indicators, these models may support personalised treatment planning and improved outcome prediction. Such approaches are particularly relevant in patients with systemic conditions such as diabetes, osteoporosis, or inflammatory disorders, where healing capacity and implant success may be affected.
These predictive capabilities align with the integrative triangle concept, where oral rehabilitation, trauma recovery, and systemic health are modelled as interconnected processes. AI-driven prediction may therefore support coordinated management strategies that account for structural, biological, and systemic factors.
Recent systematic reviews cited earlier indicate that AI-enabled implant planning and digital workflows demonstrate promising improvements in planning efficiency and surgical accuracy. However, many studies remain retrospective or simulation-based, and prospective multicentre validation remains limited. Clinical adoption is increasing but varies across institutions depending on infrastructure, interoperability, and regulatory considerations.
AI demonstrates strong performance in analysing intraoral photographs, bitewings, panoramic radiographs, and cone-beam CT images to detect caries, bone loss, and periapical pathology [27, 28]. Machine learning applied to histopathological slides enhances recognition of oral potentially malignant disorders (OPMD) and oral squamous cell carcinoma (OSCC) [29]. Thus, automated detection systems embedded in routine practice can shorten diagnostic delays and improve consistency in interpretation.
Recent work has also evaluated multimodal AI systems for oral diagnosis using broader performance criteria beyond conventional accuracy metrics. For example, a multimodal AI model was assessed across diagnostic accuracy, narrative quality, calibration, and response latency, while comparing performance with human experts [30]. Such multidimensional evaluation frameworks are particularly relevant for clinical deployment, where explainability, reliability, and workflow efficiency are critical considerations. These findings highlight the importance of assessing multimodal AI systems using clinically meaningful metrics that extend beyond classification performance alone.
Longitudinal electronic dental records facilitate predictive analytics for identifying patients at risk of disease progression [31, 32]. Algorithms can predict rapid periodontal attachment loss, peri-implantitis, or caries recurrence. These insights enable risk-adapted maintenance and resource optimization, ensuring that preventive interventions are allocated according to patient-specific profiles.
Mobile imaging combined with AI inference can support remote screening and early referral [33]. Cloud-based solutions using smartphone cameras can extend access to diagnostics in resource-limited regions, potentially improving early detection of oral malignancy and reducing late-stage presentation.
Stomatognathic diseases and systemic disorders exhibit strong bidirectional relationships [4, 34–41]. Periodontal inflammation contributes to atherosclerotic burden, while metabolic dysregulation and oxidative stress exacerbate oral tissue breakdown [42]. AI and advanced data science methods capable of managing nonlinear and high-dimensional data offer new approaches for investigating causality beyond correlation [43].
Multimodal AI architectures can integrate radiographs, laboratory data, medication history, and microbiome signatures to produce unified patient embeddings [44–48]. Related approaches have also been applied to oral-systemic health integration [49, 50]. Graph neural networks (GNNs) can capture dependencies between oral features and systemic biomarkers, facilitating the prediction of cardiovascular events or glycaemic trajectories [51].
The NLP of combined medical and dental records can allow identification of comorbidity networks and temporal patterns linking oral inflammation with systemic outcomes [52, 53]. Federated learning frameworks enable collaborative model development across institutions while preserving data privacy [54].
Consider a patient presenting with a mandibular fracture following low-energy trauma in the context of poorly controlled type 2 diabetes and chronic periodontitis. Imaging-derived fracture characteristics indicate increased comminution and delayed callus formation, while periodontal indices and inflammatory biomarkers suggest elevated systemic inflammatory burden. Within the integrative triangle, AI-enabled models jointly analyse trauma imaging, oral health parameters, and metabolic indicators to estimate infection risk, predict healing trajectories, and identify modifiable contributors to delayed recovery. As postoperative outcomes are observed, these data are reintegrated to refine risk estimation, informing coordinated surgical, dental, and metabolic interventions. This example illustrates how acute facial trauma can serve as an entry point for identifying systemic vulnerability and how oral health acts as a mediator linking local injury to broader disease processes. This illustrative scenario motivates the conceptual structure of the integrative triangle described below.
Within the integrative triangle, AI is not positioned as a collection of analytical tools, but as an enabling mechanism for modelling the causal continuum linking oral inflammation, systemic dysfunction, and recovery following facial trauma. The central conceptual advance lies in treating facial trauma, oral health, and systemic disease as dynamically coupled states rather than independent clinical entities. By integrating imaging-derived biomarkers, periodontal indices, and systemic laboratory parameters, AI-enabled models can represent mediating pathways and feedback effects that are not accessible through siloed analysis. This perspective reframes recovery and disease progression as interconnected processes and enables hypothesis-driven simulation of intervention effects across domains.
Although the integrative triangle is introduced here as a unified conceptual framework, elements of this model already exist in partially integrated clinical and research domains. For example, substantial evidence supports bidirectional relationships between oral health and systemic disease, including diabetes, cardiovascular disease, and inflammatory disorders [6]. Similarly, systemic conditions such as diabetes, osteoporosis, and vascular disease are known to influence fracture healing, infection risk, and surgical outcomes in CMF trauma. In addition, perioperative risk prediction models increasingly integrate systemic comorbidities with imaging-derived and clinical features to support personalised surgical planning and complication risk estimation [55].
However, these approaches typically operate within pairwise integrations, such as oral-systemic or trauma-systemic modelling, rather than a fully unified triangular framework.
Consequently, the integrative triangle remains at an early conceptual and methodological stage, with limited real-world implementations that simultaneously model facial trauma, oral health, and systemic disease within a single multimodal architecture.
Rather than viewing facial trauma solely as an acute surgical event, the integrative triangle positions it as a measurable perturbation of systemic resilience. Fracture patterns, healing trajectories, and postoperative complications reflect underlying metabolic, inflammatory, and vascular states. AI models that relate trauma morphology to systemic indicators, therefore, serve as exploratory instruments for uncovering latent systemic vulnerabilities, shifting the role of trauma data from descriptive imaging to mechanistic insight.
Within this framework, oral health is conceptualised as a mediating state that modulates both systemic risk and trauma recovery. Periodontal inflammation contributes to systemic inflammatory load, while oral microbial and tissue conditions influence infection risk and wound healing. AI-based mediation modelling enables quantification of these effects, allowing oral pathology to be represented as an active contributor to recovery dynamics rather than a coincidental comorbidity. This reframing supports the hypothesis that targeted oral interventions may alter systemic and surgical outcomes through identifiable causal pathways [56].
Systemic disorders such as diabetes, cardiovascular disease, and osteoporosis are incorporated as feedback drivers that influence both susceptibility to injury and repair capacity. In the integrative triangle, systemic disease is not treated as a static background risk but as a dynamic state that evolves in response to trauma and oral inflammation. Multimodal predictors capturing these feedback effects allow trauma recovery to be interpreted as a functional readout of systemic control, extending concepts explored in other domains of recovery science [57].
Recent advances in multimodal AI provide foundational components for this integration. Vision-language models [58], GNNs [59], and multimodal fusion architectures [60] have demonstrated the feasibility of combining heterogeneous data sources, including imaging, clinical records, and laboratory measurements, into unified predictive frameworks. In dentistry, similar multimodal AI approaches have been applied to oral disease detection, risk stratification, and outcome prediction, illustrating the potential of cross-domain data integration for clinical decision support [61–63]. These developments represent building blocks of the integrative triangle, but comprehensive implementations that simultaneously integrate all three domains remain limited.
A defining feature of the integrative triangle is its closed-loop structure. Sequential stages of sensing, prediction, planning, action, and learning are continuously linked through AI-driven feedback. Outcomes following surgical or preventive interventions are reintegrated into predictive models, enabling adaptive refinement of risk and outcome representations. This closed-loop configuration represents a conceptual shift from episodic, disease-centred care toward a learning-based model in which acute events and chronic conditions jointly inform long-term management strategies.
Table 1 summarises representative multimodal data sources that support this paradigm by enabling predictive, generative, and causal modelling across the facial trauma, oral health, and systemic disease domains.
Illustrative multimodal signals and analytical roles for integrative AI across the triangle (non-exhaustive).
| Domain | Representative data streams | AI applications/Analytical goals |
|---|---|---|
| Facial trauma | CT/CBCT volumes; segmentation masks; 3D meshes; operative notes; fix-ation metadata; perioperative labora-tory results | Image intelligence for fracture detection and morphology characterisation; outcome and complication risk estimation; simulation of healing trajectories |
| Oral health | Intraoral photographs; radiographs (bitewing, panoramic); periodontal charts; histopathology WSI (whole slide imaging); microbiome profiles | Automated disease detection; progression and mediation modelling; causal inference linking oral inflammation with systemic and surgical outcomes |
| Systemic | EHR summaries; medication history; vital signs; laboratory data (HbA1c, CRP, lipid panels); DEXA; ECG/echocardiography; wearable-derived signals | Multimodal data fusion for systemic risk estimation; longitudinal outcome prediction; identification of feedback effects influencing trauma recovery and oral health |
AI: artificial intelligence; CBCT: cone beam computed tomography; CT: computed tomography; CRP: C-reactive protein; ECG: electrocardiography.
The deployment of integrative AI systems across facial trauma, oral health, and systemic disease introduces important ethical, legal, and regulatory challenges. Unlike single-domain models, multimodal cross-domain AI integrates heterogeneous data sources, including imaging, clinical records, laboratory values, and behavioural data. This complexity increases the risk of bias propagation, data imbalance, and unintended disparities across demographic, socioeconomic, and institutional contexts. Ensuring fairness, therefore, requires careful dataset curation, cross-institutional validation, and performance auditing across diverse patient populations.
Explainability is particularly important in integrative AI systems, where predictions may be derived from multiple interacting data sources. Clinicians must understand how imaging features, oral health indicators, and systemic parameters jointly contribute to model outputs. Techniques such as feature attribution, attention-based modelling, and interpretable graph representations may help improve transparency and clinician trust. Human-in-the-loop frameworks may further support safe deployment by combining algorithmic recommendations with expert clinical oversight.
Regulatory implementation also presents challenges for integrative AI systems that operate across multiple clinical domains. Existing regulatory frameworks for medical AI are typically designed for single-purpose applications, whereas integrative models may influence surgical planning, dental management, and systemic disease risk assessment simultaneously. This cross-domain functionality may require adaptive regulatory pathways, continuous monitoring, and post-deployment performance evaluation. Federated learning and privacy-preserving architectures may further support regulatory compliance by enabling multi-institutional model development without centralised data sharing [64].
In addition, governance frameworks should address accountability, transparency, and auditability of AI-assisted decision-making [65]. Documentation of model development, dataset composition, and validation procedures will be essential to support responsible implementation. These considerations are particularly important for multimodal integrative systems, where interactions between domains may introduce new sources of uncertainty.
Addressing these ethical, regulatory, and explainability challenges will be critical for translating the integrative triangle from a conceptual framework to clinically deployable systems. Future work should therefore prioritise fairness-aware modelling, transparent algorithm design, and prospective evaluation within regulated clinical environments.
This perspective aims to introduce the integrative triangle as a conceptual framework linking facial trauma, oral health, and systemic disease through multimodal AI. The primary objective is to synthesise emerging developments across these domains and propose a translational roadmap for integrated precision care, rather than to present new experimental findings or validated clinical models.
This perspective has several limitations. First, the integrative triangle is introduced as a conceptual framework and is not supported by original experimental data or prospective clinical validation within this work. While individual components of the triangle-facial trauma analytics, oral-systemic modelling, and multimodal AI have been explored in prior studies, their unified integration remains at an early stage. Consequently, many of the described applications represent anticipated capabilities based on emerging multimodal AI technologies rather than established clinical implementations.
Furthermore, evidence from prospective multicentre studies evaluating integrative AI approaches across facial trauma, oral health, and systemic disease remains limited. The clinical impact, workflow feasibility, and cost-effectiveness of such integrative systems therefore require rigorous evaluation. This work is intended to provide a conceptual and translational roadmap to guide future empirical validation and interdisciplinary collaboration.
To transition from a conceptual framework to clinical implementation, a staged translational pathway is required. Initial efforts should focus on establishing pilot and multicentre registries that integrate trauma imaging, oral health indicators, and systemic clinical data, enabling harmonised multimodal datasets across institutions. These data can support proof-of-concept multimodal modelling and retrospective validation to assess whether integrative approaches provide incremental predictive value beyond single-domain models.
Advances in AI for the integrative triangle are expected to transition from prediction to actionable intervention. Generative design can yield biomechanically validated implants; adaptive perioperative algorithms can synchronise surgical planning with metabolic indicators; and causal mediation models can guide targeted periodontal therapy. Prospective multicentre trials and open data collaborations will be crucial for evaluation. In low-resource settings, lightweight edge AI systems [66] may extend diagnostic and triage capabilities, supporting equitable global health initiatives [67].
Building on this trajectory, future work should focus on translating the integrative triangle from a conceptual framework into an evaluable research paradigm within clinical and health-system settings. A first step involves the establishment of pilot multicentre registries that prospectively capture harmonised trauma, oral-health, and systemic data, enabling structured experimentation with multimodal data fusion across institutional boundaries. These registries would provide controlled environments for assessing feasibility without presupposing clinical deployment.
Progress in operationalisation can be monitored using measurable methodological milestones, including data harmonisation success rates across domains, stability and interpretability of multimodal representations, and quantitative indices of model explainability and uncertainty. Additional performance indicators may include integration efficiency, defined as the incremental predictive or causal insight gained through cross-domain modelling relative to single-domain baselines.
As methodological robustness is established, the integrative triangle can support a staged progression from prediction toward hypothesis-driven intervention studies. Early-phase trials may examine whether AI-informed coordination between surgical, dental, and systemic management alters recovery trajectories or risk profiles, thereby generating evidence to guide subsequent interventional designs. This milestone-based roadmap emphasises iterative validation and learning, ensuring that advances in integration, interpretability, and feedback modelling precede large-scale clinical implementation.
Subsequent prospective observational studies should evaluate workflow integration, data interoperability, and clinician acceptance in real-world settings. Ultimately, interventional trials will be required to determine whether integrative AI-guided coordination of surgical, dental, and systemic management improves clinically meaningful outcomes, including complication rates, healing trajectories, hospital length of stay, and long-term systemic health indicators. Parallel work should address interpretability, fairness, generalisability, and cost-effectiveness to support scalable and responsible deployment within integrated precision medicine frameworks.
AI can constitute the computational infrastructure linking facial trauma, oral health, and systemic disease into an integrated, learning-based framework. By operationalizing the integrative triangle through multimodal sensing, causal inference, and predictive modelling, clinical care can become simultaneously more precise, preventive, and patient-centred. Responsible implementation, supported by transparent data governance and interdisciplinary collaboration, has the potential to reposition dentistry and facial trauma surgery as core components of systemic precision medicine.
AI: artificial intelligence
CBCT: cone beam computed tomography
CMF: cranio-maxillofacial
CT: computed tomography
GNNs: graph neural networks
NLP: natural language processing
PSIs: patient-specific implants
TDP: Conceptualization, Investigation, Methodology, Visualization, Writing—original draft, Writing—review & editing. The author read and approved the submitted version.
Tuan D. Pham, who is the Editorial Board Member of Exploration of Medicine, had no involvement in the decision-making or the review process of this manuscript. There are no other conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 585
Download: 18
Times Cited: 0
