 Review
Review

Affiliation:
1Department of Drug Discovery, Galaxies Pharmaceuticals, Juhkentali 8, 10132 Tallinn, Estonia
2Walker College of Business, Appalachian State University, Boone, NC 28608, USA
ORCID: https://orcid.org/0000-0002-3837-8469
Affiliation:
1Department of Drug Discovery, Galaxies Pharmaceuticals, Juhkentali 8, 10132 Tallinn, Estonia
Email: fa_saad@yahoo.co.uk
ORCID: https://orcid.org/0000-0003-3170-3449
Explor Med. 2026;7:1001411 DOI: https://doi.org/10.37349/emed.2026.1001411
Received: November 11, 2025 Accepted: January 24, 2026 Published: June 11, 2026
Academic Editor: Yingyong Zhao, Northwest University, China
Recent studies argue that other physiological solutions are superior to normal saline, which is due to their physiological features, better outcomes in critical care, and lower risk of hyperchloremia and acidosis; nonetheless, it is still a mystery how normal saline has dominated the field of fluid therapy worldwide. Moreover, there is an ongoing debate on whether harm to human health may limit its spread in the future. Additionally, new evidence revealed some of the deleterious effects of normal saline, including coagulopathy, metabolic acidosis, acute kidney injury (AKI), and higher mortality in ICU. The predominant cause for these outcomes appears to be the excess chloride concentration of normal saline relative to plasma. Therefore, it appears relevant to suggest that a normal saline solution should be normalized to that of human serum to overcome these pitfalls. An ideal normal saline solution shall be similar to human serum in its pH, osmolarity, and content of sodium, chloride, and essential minerals.
Normal saline, or physiological saline, as it is frequently called, is a 0.9% sodium chloride (NaCl) solution. It is mainly used to treat dehydration caused by various reasons and as a solvent for drugs in neurology and critical care clinics, where a large amount of experience has been gathered. Commercial normal saline contains 9 g of NaCl per liter, adjusted with hydrochloric acid (HCl) to a pH of around 5.5 [1]. Nonetheless, commercial normal saline is perhaps not normal in many ways [2], or simply, it is neither normal nor physiological [2–5]. Although of the acidic nature (pH 5.6) of normal commercial saline, it is hereafter referred to as normal saline. Normal saline is an unbuffered solution with a higher osmolarity of 308 milliosmoles per liter (mOsm/L) [6] than human serum of 285 (275 to 295) mOsm/L [7–9]. This supraphysiologic chloride content may cause various adverse effects [9]. Figure 1 represents the formula structure of commercial saline (pH, osmolarity, and sodium and chloride concentration).
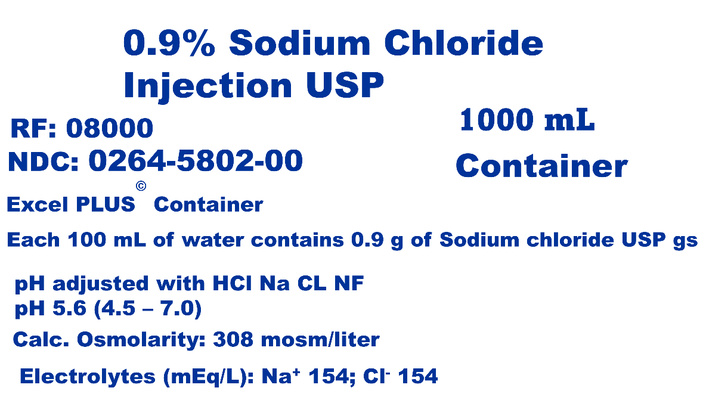
Normal saline formula structure. Osmolarity of 308 mOsm/L, pH 5.6 (4.5–7.0), and sodium and chloride concentrations of 154 mEq/L each. mEq/L: milliequivalents per liter; mOsm/L: milliosmoles per liter.
However, almost two centuries have elapsed since the controversial introduction of normal saline into clinical practice in 1831; it has come to dominate intravenous hydration and fluid resuscitation worldwide. Although a wide variety of side effects are associated with normal saline infusion, it is still a common practice in modern critical care medicine. While various physicians and scientists are aware of the harmful effects of acidic saline infusion on human health, the infiltration of this information to critical care physicians is still poor or lacking. Hence, the harmful effects of normal saline infusion on human health shall be emphasized during medical school education, so physicians may avoid this practice. Normal saline has a lower pH and higher osmolarity, sodium, and chloride concentration than human serum. Thus, it seems important to suggest that osmolarity, chloride and sodium concentration, and the pH of normal saline should be normalized to that of the human serum to avoid these pitfalls. Normal saline is mainly used to treat dehydration caused by various reasons and as a solvent for drugs in neurology and orthopedic surgery clinics (Figure 2). An ideal saline solution shall be similar to serum in its pH, osmolarity, and the content of sodium, chloride, and essential minerals. Once ideal saline solutions have been identified and their efficacy is tested, it is evident that normal saline will be replaced in favor of safer physiological solutions. Actually, balanced crystalloids, which are physiologically closer to plasma than normal saline, have been shown to reduce the composite outcome of death, initiation of renal-replacement therapy, or persistent renal dysfunction in critically ill adults. On the other hand, among critically ill patients requiring fluid challenges, the use of crystalloids compared with 0.9% saline solution did not significantly reduce 90-day mortality. This minireview highlights issues on the horizon of normal saline, enriches, and sparks the ongoing debate led by experts in the field of fluid therapy, like Santi and colleagues [10]. Furthermore, it underlines the various effects of normal saline on calcium homeostasis, induction of pain, and the physiology of blood, kidney, bone, muscle, heart, and brain.
Normal saline applications in medical practice. Fluid resuscitation, including blood volume restoration (left side), or as a carrier fluid for administering medications and other intravenous therapies (right side).
Calcium represents the fifth element in the human body, with about 1 kg in adults [11]. However, about 990 g of total body calcium is present in bone as a calcium phosphate complex (hydroxyapatite), the rest, ~10 g, represents ionic calcium, ionic calcium complexes (calcium phosphate, calcium carbonate, and calcium oxalate), and protein-bound calcium (mainly albumin and globulin in serum), representing 40, 10, and 50% respectively [12]. Calcium plays an essential role in a wide range of biological functions, including bone extracellular matrix mineralization through either endochondral or intramembranous pathways. Calcium provides skeletal strength and serves as a reservoir for calcium release into serum through the parathyroid hormone (PTH) bone resorption pathway. Ionic (free) calcium (hereafter calcium) homeostasis is hormonally regulated by PTH, vitamin D3, and calcitonin [13].
Changes in pH have remarkable influences on calcium homeostasis [14]. Metabolic acidosis induces bone mineral resorption and inhibits osteoblast matrix mineralization in vitro [15, 16]. Hinkle and Cooperman [17] measured serum calcium concentration in a group of six patients after receiving citrated blood transfusions during general anesthesia. This study revealed an average decrease of 0.5 mg/100 mL or 0.6 mg/100 mL after 500 or 1,000 mL of citrated blood infusion, respectively. However, the calcium ion concentration increased by an average of 0.3 mg/100 mL (10 minutes after the transfusion of the citrated blood), indicating a rapid activation of the bone resorption pathway to release calcium into the bloodstream [18]. Therefore, it seems that there is no convincing rationale to use normal saline as the first choice for volume resuscitation of critically ill patients [2, 19]. Furthermore, a deficit of serum calcium due to poor dietary intake, or consumption of acidic drinks, such as soft drinks [20–25] is a detrimental factor to bone mineral density and teeth mineralization.
Normal saline induction of pain in experimental animal models and humans [26–33], myalgia [34], and hyperalgesia [26, 35–39] are popular pain models in pain research. Animal models and clinical studies indicated that normal saline injections may cause metabolic acidosis, inflammation, chronic muscle and abdominal pain, and functional and structural organ damage [40–43], neuronal depolarization [44], vascular and renal function changes [2, 45], and fibromyalgia, which is often associated with various mental disorders including cognitive impairment, anxiety, and depression [46, 47]. In contrast, normal saline pH 7.4 [48], which is equal to serum pH, normal saline (pH 4.0) injection into mice gastrocnemius muscle induces chronic muscle hyperalgesia lasting over 2 weeks [35], which is mediated through acid sensing ion channel 3 [49]. While it is established that acidosis induces pain, acidosis signaling is linked to many elusive chronic pain diseases [50]. Intravenous injection of vecuronium and normal saline (pH 4.08) mixture exacerbates pain in humans [51]. On the contrary, neutral fluid (pH 7.4) infusion into hand skin or interosseous muscle triggers no pain in complex regional pain syndrome patients or healthy controls [52].
Blood roughly comprises 7% of body weight, and it contains plasma, red cells (erythrocytes), white cells (leukocytes), and platelets (thrombocytes). Healthy human blood pH is about 7.4, which is tightly regulated to remain within a minute range of 7.35 to 7.45 [2, 52–55]. Therefore, pH alterations beyond this range can be detrimental to cellular processes such as enzymatic functions that may lead to cellular death. Systemic blood acidity (acidemia) occurs when blood pH drops under 7.28 [56]. However, Khan and colleagues [57] reported that acidosis emerges when blood pH drops below 7.34. Normal saline absorption during transurethral and transcervical surgery leads to metabolic acidemia [58]. A major side effect of normal saline is hyperchloremic acidosis [59–62]. Low-grade metabolic acidosis reduces blood buffering capacity, leading to a greater reliance on muscle, bone, and connective tissue for the removal of residual acid [63]. Furthermore, Yang and colleagues [64] revealed that acidosis elicits tumorigenesis by activating the serine threonine kinase/nuclear factor-κB (Akt/NF-κB) signaling pathway. Lenert and colleagues [65] have proven that normal saline (pH 4.0) promotes T cell-mediated activation of B cells, enhances active plasma cells, increases memory B cells, and raises MHC class II-expressing B cells in peripheral blood, while reducing immunoglobulin G (IgG) levels in a model of chronic widespread pain in a female mouse model. However, therapy of blood acidosis using reduced osmolarity mixed-base solution having a 3:1 ratio of sodium carbonate: sodium bicarbonate or simply carb: bicarb (Na2CO3:NaHCO3) has been achieved through raising plasma pH and serum bicarbonate concentration [HCO3]− while reducing the partial pressure of CO2; normally known as PCO2 [66].
Kidneys are the main buffering system for removing acids and salts from the body. Acute metabolic acidosis decreases the functions of the kidneys as their ability to eliminate acids goes down with acid overload in the body, which impairs kidney function over long periods of time. In fact, chronic metabolic acidosis leads to nephron hypertrophy in animal models, which is due to ammonia’s toxic effects on the kidneys. However, kidneys can remove a certain amount of acids daily before acid retention occurs due to acid overload [63]. Kidney acid overload leads to muscle and connective tissue breakdown to provide nitrogen for ammonia formation and calcium release from bone to avoid acid retention.
Authors have recently provided evidence of the deleterious effects of normal saline infusion in the emergency department, including increased mortality [67], acute kidney injury [10], metabolic acidosis, and coagulopathy, which is due to the higher chloride concentration of the normal saline [154 milliequivalents per liter (mEq/L)] relative to human serum of 96 to 106 mEq/L [68]. A multicenter retrospective study of heat stroke patients has revealed an association between the volume of normal saline infusion in the emergency departments and acute kidney injury [42, 43]. Moreover, sodium overload leads to an increase in blood pressure [69–72].
Bone remodeling includes resorption and regeneration of new bone. An upsurge of serum calcium ions (Ca2+) induces thyroid parafollicular cells (C cells) to release calcitonin, a 32-amino acid hormone. Calcitonin stimulates calcium deposition into bone and inhibits renal reabsorption of calcium, meanwhile restraining bone resorption.
Acidic serum stimulates parathyroid glands to produce PTH, which activates the bone resorption pathway and the release of calcium into the bloodstream. Calcium influx into bloodstreams restores serum pH to 7.4 and calcium concentration to a physiologic range of 88–104 mg/L [11]. Such fine-tuned calcium concentration is required for the body to maintain physiological functions [11, 73, 74]. PTH acts on the kidneys to increase calcium reabsorption and induces bone resorption to release calcium into the bloodstream. Figure 3, left column, shows the effect of normal saline infusion on the bone resorption pathway through the activation of PTH. Consequently, PTH induces the receptor activator of NF-κB ligand (RANKL), RANK, and represses osteoprotegerin, the decoy factor of RANKL [73]. The kidney responds to PTH by increasing the release of vitamin D3, stimulating the intestines to absorb calcium, as seen in Figure 3, middle column. In fact, frequent consumption of soft drinks has similar bone catabolic effects in adolescents, including impaired bone mineral accrual and high bone fracture risk [20–25].
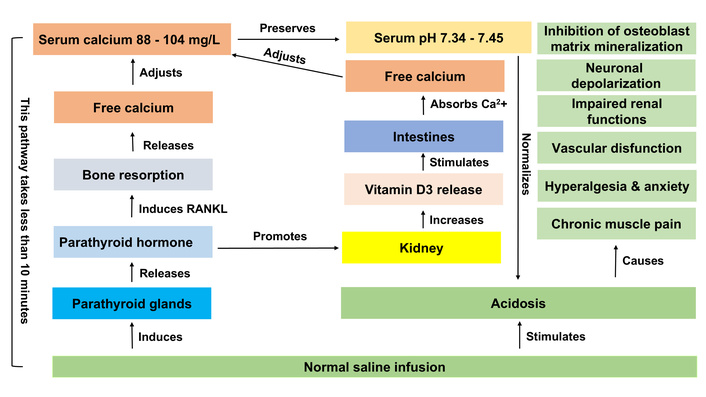
Normal saline effects on human health. Normal saline infusion induces acidosis and parathyroid glands to release parathyroid hormone. Parathyroid hormone induces RANKL to activate bone resorption and the release of free calcium into the bloodstream, which adjusts serum calcium concentration to a range of 88–104 mg/L. Such serum calcium concentration preserves serum pH to 7.34–7.45, leading to acidosis normalization. Parathyroid hormone promotes the kidneys to increase the release of vitamin D3, stimulating the intestine to absorb and infuse calcium into the serum. Acidosis causes chronic muscle pain, vascular dysfunction, impaired renal function, hyperalgesia/anxiety, neuronal depolarization, and inhibition of osteoblast matrix mineralization [86, 87].
Calcium plays an essential role in many events in the body, including cell growth, cell proliferation, programmed cell death (apoptosis), bone matrix mineralization, blood coagulation [10, 60], exocytosis, neuronal function, inflammation, nerve impulse transmission, and muscle contraction [11, 12, 75–80]. Normal saline (pH 4.0) intramuscular infusion induces hyperalgesia, chronic muscle pain, and muscle atrophy [39, 81, 82] as seen in Figure 3, right column. Intense hypocalcemia (less than 85 mg/L) may cause several medical indications, including congestive heart failure, muscle spasms and tetany, fatigue, depression, and seizures, among others [74].
In skeletal muscle, the effects of vitamin D are beyond calcium and phosphate homeostasis and bone health. Vitamin D deficiency is implicated in many neuromuscular diseases. Muscle weakness (myopathy), muscle pain (myalgia), bone pain (ostealgia), and hypotonia are commonly encountered among patients with vitamin D deficiency (e.g., rickets and osteomalacia). Muscle weakness noted in vitamin D deficiency is progressive and mostly appears in the proximal musculature [83, 84]. Metabolic acidosis affects muscle through several pathways, including inducing protein degradation while reducing protein synthesis, leading to muscle breakdown, preventing mitochondrial function, decreasing oxidative phosphorylation and energy production, and directly restricting muscle contraction [85].
Using fluorescence multiphoton microscopy and biochemical techniques, Thatte and colleagues [86, 87] have found a direct correlation between low pH (< 7.0) and apoptosis in cardiac samples obtained from patients undergoing cardiac surgery. Acidosis leads to mechanical alterations in the ferret heart muscle [87]. Furthermore, acidosis of intracellular fluid reduces the contractility of the heart muscle due to its sensitivity to minor physiological decreases in extracellular pH [88]. A steady fall in the pH beyond 7.28 during normal saline infusion in animal models leads to declines in several measures of cardiac function, including global ejection fraction, the maximal rate of rise of left ventricular pressure (dPmax), stroke volume index, cardiac function index, cardiac power index, and cardiac index [56]. Preclinical studies in animal models have shown that systemic acidemia can impair cardiovascular function and weaken cardiac contractility [89], which may lead to heart failure [90–92]. Furthermore, intramuscular injection of normal saline (pH 4.0) triggers widespread pain and unbalanced cardiovascular dysfunctions [93].
Acidosis is a normal aspect of the human brain during ischemic stroke and can cause neuronal injury, which is due to the activation of acid-sensing ion channels [94]. Severe acidosis (pH 6.2) potentiates neuronal apoptosis during cerebral ischemia, which may partially result from oxidative injury exacerbation [95, 96]. Moreover, neuronal loss is detected in the hippocampus of mice following prenatal injection of normal saline [97]. In reality, acidosis induces necrosis and apoptosis of cultured hippocampal neurons [98]. Also, it has been shown that lowering blood pH impairs the nervous system’s excitability to electrical stimulation [99]. Additionally, acidosis may play an essential role in the development of vascular dementia (multi-infraction dementia) and Alzheimer disease [100]. Normal saline (pH 6.2) increases cytosolic calcium ions by stimulating calcium influx in the nucleus ambiguous neurons [44].
The blood-brain barrier (BBB) firmly controls the entry of molecules from plasma into the central nervous system (CNS) and plays a crucial role in appropriate CNS functions. BBB dysfunctions appear in several degenerative neurological disorders such as Alzheimer and Parkinson diseases, among others [101]. However, hyperosmolarity disrupts the BBB of male Wistar rat brains [102]. Furthermore, acidosis impairs brain functions through cortical gamma aminobutyric acid (GABA)ergic neurons deterioration [103, 104]. which is due to the dysfunction of cortical GABAergic neurons through astrocyte-intermediated excitotoxicity [105]. Additionally, acidosis causes neurological disorders via the overexcitation of cortical pyramidal neurons [106].
Guo and colleagues [107] have indicated that acidosis exercises its cytotoxic effects on HT22 neurons by promoting autophagic cell death through the acid-sensing ion channel 1 (ASIC1)-related Akt/mTOR signaling pathway [108]. Moreover, mouse colon sensory neurons sense extracellular acidosis through the transient receptor potential cation channel subfamily V member 1 (TRPV1) [108]. Pirchl and colleagues [100] have revealed that cholinergic neurons have a high capacity to recompense for pH perturbations. However, at a certain pH, cholinergic neurons show weakness, indicating that a low pH has deleterious effects on the brains of Alzheimer patients. Moreover, acidosis may exacerbate the deposition of β-amyloid peptide in the CNS and basal ganglia and contribute to Alzheimer and Parkinson disease pathogenesis [109, 110]. Furthermore, carbonated soft drinks increase oxidative stress and alter the expression of certain genes in the brain of Wistar rats (i.e., increase serum levels of malondialdehyde and dopamine D2 receptor, downregulate the expression of antioxidants glutathione reductase, catalase, glutathione peroxidase, monoamine oxidase A, and 5-hydroxytryptamine transporter, and acetylcholine esterase), which are related to brain activity [111].
While normal saline is mainly used to treat dehydration caused by various reasons and as a solvent for drugs in neurology and orthopedic surgery clinics; nonetheless, some cautions on side effects have to be considered. The medical use of acidic saline in patient care for volume substitution and restoration, as well as hematology and transfusion medicine, began around 1831 [112, 113], which was initiated on the basis of historic delusion and misconception [3]. However, it remains a historical mystery how it came to dominate intravenous infusion and fluid revitalization worldwide [114]. Furthermore, investigations of the composition of the fluids administered by pioneering physicians of that era, such as Thomas Aitchison Latta, reveal solutions without resemblance to normal saline, which indicate that normal saline may have very little scientific basis for its routine use in critical care medicine [3].
Normal saline has nearly 40% more chloride, 10% more sodium, and a lower pH (5.6 versus 7.4) than human serum [113]. Additionally, serum essential minerals are vital for innate and adaptive immune systems [115]. There are concerns about whether normal saline is the safest alternative for infusion therapy [2]. The effects of citrated blood transfusion on bone calcium depletion have been known for more than half a century [17]; nonetheless, normal saline transfusion is still a common practice in USA hospitals and around the world. Although infusion of normal saline can lead to metabolic acidemia, Reddi [1] has reported that the acidity of saline solution is unrelated to acidemia following normal saline infusion.
In animal models and clinical trials, normal saline infusion has been correlated with adverse events including microcirculation problems, acute kidney injury, adverse clinical outcomes, immunological disorders, endothelial activation, a greater inflammatory response, retinal degeneration, glaucoma [10, 15, 42, 116], and glycocalyx degradation among other side effects; all of which are caused by hyperchloremic acidosis [112, 117–118]. However, recent studies argue that other physiological solutions are superior to normal saline, which is due to their physiological characteristics, better outcomes in critical care, and lower risk of hyperchloremia and acidosis [9, 119, 120].
Shaw and colleagues [121] have reported major complications, mortality, and resource utilization after open abdominal surgery comparing 0.9% saline to Plasma-Lyte. Also, Waikar and Winkelmayer [122] believe that sparing intravenous chloride will save from kidney injury.
Furthermore, monoclonal antibodies (mAbs) that are dissolved in normal saline (pH ≤ 6.5) entirely form insoluble aggregates upon mixing with dextrose and serum. This aggregation was not feasible for the mAbs that are liquefied in neutral pH buffers (7.2–7.5) or in buffers containing NaCl with neutral pH [123], which has implications in selecting the right diluent for intravenous infusion of therapeutic mAbs.
Nonetheless, a Canadian crossover trial of hospital-wide lactated Ringer versus normal saline did not result in a meaningfully inferior incidence of death or readmission to the hospital within 90 days after the index admission [124–126]. Moreover, the same results were replicated in a multicenter, double-blind randomized clinical trial conducted in 75 ICUs in Brazil, including the randomization of approximately 11,000 patients to balanced crystalloids or saline groups [127].
Another randomized controlled trial comparing normal saline and lactated Ringer as intravenous fluid therapy in children with diabetic ketoacidosis (DKA) revealed that lactated Ringer can be carefully considered for the administration of pediatric DKA and may be ideal in patients that are at a risk of difficulties due to hyperchloremia [128], indicating that lactated Ringer may offer benefits over normal saline for the handling of patients with DKA [43].
Moreover, current evidence from clinical trials, observational research, and basic science research suggests that using balanced crystalloids such as lactated Ringer or plasma-lyte rather than normal saline may have valuable effects on patient outcomes, renal physiology, and acid-base balance [60, 129]. Nonetheless, the use of normal saline may be favored in certain clinical settings such as advanced liver disease, cerebral edema, and hyperkalemia with renal failure [130]. Also, lactated Ringer appears inappropriate for patients at risk for brain edema and for those with obvious or hidden chloride-deficiency [10]. In reality, Vanderbilt University Medical Center is encouraging physicians to stop using normal saline for intravenous fluid therapy for most patients, a change triggered by landmark clinical trials [131–136]. Yet, it seems that normal saline is a “problem”, not a “solution” [137]. Therefore, the fluid therapy debate shall continue until the characterization of ideal colloid and balanced crystalloids solutions has been fully attained [138–142].
While various adverse effects of normal saline have regularly been highlighted in scientific literature, its use remains common in clinical practice. The precision medicine strategy for fluid therapy should represent the ultimate principle for all patients, considering the best crystalloid therapy suitable for each patient. However, an ideal saline solution shall be like human serum in its pH, osmolarity, essential minerals (calcium, magnesium, potassium, iron, zinc, copper, and selenium), sodium, and chloride strengths. Therefore, until the formulation of this ideal saline solution, the great fluid debate shall continue. However, there is evidence that changing the pH of normal saline to 7.4 has a major effect in reducing the pain [52] and inhibits bone resorption.
Akt: serine threonine kinase
BBB: blood-brain barrier
CNS: central nervous system
DKA: diabetic ketoacidosis
GABA: gamma aminobutyric acid
mAbs: monoclonal antibodies
mEq/L: milliequivalents per liter
mOsm/L: milliosmoles per liter
NaCl: sodium chloride
NF-κB: nuclear factor-κB
PTH: parathyroid hormone
RANKL: receptor activator of nuclear factor ligand
Fawzy A. Saad is the founder of Galaxies Pharmaceuticals. The authors would like to thank Natalie B. Saad for reading the manuscript. The author asserts that the work presented within the manuscript is their own original creation and not under consideration for publication elsewhere.
JFS: Data curation, Formal analysis, Writing—review & editing. FAS: Conceptualization, Writing—original draft, Writing—review & editing, Supervision. Both authors read and approved the submitted version.
The authors declare that there are no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
There are no sources of financial assistance that were used to conduct the study or the analysis of the results described in the manuscript or used to assist with the preparation of the manuscript.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 500
Download: 10
Times Cited: 0
