Case Report
Case Report

Affiliation:
1Department of General Surgery, Faculty of Medicine, Istanbul Atlas University, Istanbul 34403, Turkey
Email: opdreyildirim@gmail.com
ORCID: https://orcid.org/0000-0003-2733-402X
Affiliation:
2Faculty of Medicine, Istanbul Atlas University, Istanbul 34403, Turkey
ORCID: https://orcid.org/0009-0000-7054-5274
Affiliation:
2Faculty of Medicine, Istanbul Atlas University, Istanbul 34403, Turkey
ORCID: https://orcid.org/0009-0005-0062-1979
Affiliation:
2Faculty of Medicine, Istanbul Atlas University, Istanbul 34403, Turkey
ORCID: https://orcid.org/0009-0002-8106-4649
Affiliation:
2Faculty of Medicine, Istanbul Atlas University, Istanbul 34403, Turkey
ORCID: https://orcid.org/0009-0002-4879-0868
Affiliation:
3Department of Internal Medicine, Faculty of Medicine, Istanbul Atlas University, Istanbul 34403, Turkey
ORCID: https://orcid.org/0000-0003-1096-421X
Affiliation:
4Department of Radiology, Faculty of Medicine, Istanbul Atlas University, Istanbul 34403, Turkey
ORCID: https://orcid.org/0000-0002-4884-9842
Affiliation:
5Department of Medical Biochemistry, Faculty of Medicine, Istanbul Atlas University, Istanbul 34403, Turkey
ORCID: https://orcid.org/0000-0002-1347-8498
Explor Dig Dis. 2026;5:1005119 DOI: https://doi.org/10.37349/edd.2026.1005119
Received: January 23, 2026 Accepted: March 26, 2026 Published: April 09, 2026
Academic Editor: Jose C. Fernandez-Checa, Institute of Biomedical Research of Barcelona (IIBB), CSIC, Spain
Acute mesenteric ischemia (AMI) is a rare but highly lethal vascular emergency resulting from the abrupt interruption of intestinal blood flow. In advanced stages, extensive bowel necrosis may require near total enterectomy, leading to short bowel syndrome and permanent dependence on parenteral nutrition. An 86-year-old woman with atrial fibrillation and multiple cardiometabolic comorbidities presented with acute abdominal pain, nausea, and vomiting. Initial laboratory findings revealed marked leukocytosis and severe systemic inflammation (CRP: 21.0 mg/L). Computed tomography (CT) angiography demonstrated impaired perfusion of the superior mesenteric artery. Emergency laparotomy confirmed extensive jejunoileal ischemic necrosis, necessitating near total enterectomy with stapled jejunoileal anastomosis. Second-look surgery revealed progressive ischemia of the ileocecal region and right colon, requiring extended right hemicolectomy. Postoperatively, the patient was managed with total parenteral nutrition and intensive supportive care. Despite temporary stabilization and discharge on home parenteral nutrition, she died six months later. AMI complicated by short bowel syndrome is associated with poor prognosis in elderly patients. Persistent systemic inflammation, progressive organ dysfunction, and intestinal failure remain major determinants of adverse long-term outcomes, highlighting the critical importance of early diagnosis, prompt surgical intervention, and multidisciplinary postoperative management.
Acute mesenteric ischemia (AMI) is a sudden interruption of intestinal blood supply, which can result in cellular injury, necrosis, and death if untreated. The condition may arise from arterial embolism, arterial thrombosis, venous thrombosis, or arterial vasospasm [1]. Risk factors include atrial fibrillation, valvular heart disease, ventricular dysfunction, prior cardiac procedures, peripheral arterial disease, hemodialysis, vasoconstrictive drug use, and coagulation disorders [2].
Although AMI accounts for less than 1% of acute abdomen cases in emergency departments, mortality rates range from 50–90% due to nonspecific presentation and diagnostic delays [3, 4]. Early recognition based on patient history and physical examination is crucial. Initial signs may be minimal, but progressive disease leads to distension, absent bowel sounds, and peritoneal irritation. Laboratory findings such as leukocytosis, elevated lactate, D-dimer, and metabolic acidosis may be present [5].
Imaging studies, including Doppler ultrasonography and computed tomography (CT) angiography, are essential for diagnosis. CT angiography without oral contrast can reveal intestinal dilatation, wall thickening, thromboembolic obstruction, pneumatosis, and intra-abdominal free fluid [6].
Treatment begins with fluid resuscitation, electrolyte correction, pain management, anticoagulation, and antibiotics. Surgical intervention is warranted in suspected intestinal necrosis or perforation [7]. In severe cases, necrosis may necessitate near total enterectomy (NTE), “No Gut Syndrome”, or short bowel syndrome, defined as the removal of the entire small intestine from the ligament of Treitz to the ileocolic junction, sometimes extending to the transverse colon [8, 9]. Patients with short bowel syndrome require lifelong parenteral nutrition. Postoperative care is complex due to comorbidities, risk of sepsis, and nutritional challenges [10–13]. In the present report, we describe an elderly patient with AMI complicated by NTE and subsequent short bowel syndrome.
The chronological sequence of the patient’s clinical course and major interventions is summarized in Table 1.
Timeline of the patient’s clinical course.
| Date | Clinical event | Findings | Intervention |
|---|---|---|---|
| 04.02.2024 | Admission | Severe abdominal pain, leukocytosis, CRP: 21.0 mg/L, CT angiography showing SMA hypoperfusion | Diagnostic evaluation and resuscitation |
| 05.02.2024 | First emergency laparotomy | Extensive jejunoileal necrosis | Near total enterectomy and jejunoileal anastomosis |
| 06.02.2024 | Postoperative deterioration | CRP > 335 mg/L, elevated NLR | Clinical reassessment |
| 06.02.2024 | Second-look laparotomy | Ischemia involving the ileocecal region and the right colon | Extended right hemicolectomy and jejunostomy |
| Postoperative period | Intensive care | Intestinal failure and systemic inflammation | Total parenteral nutrition |
| 6-month follow-up | Home care period | Recurrent infections and metabolic complications | Death |
CRP: C-reactive protein; CT: computed tomography; SMA: superior mesenteric artery; NLR: neutrophil-to-lymphocyte ratio.
This report describes a single elderly patient diagnosed with AMI who underwent emergency surgical management at Istanbul Atlas University Hospital. Clinical, laboratory, radiological, operative, and postoperative data were collected retrospectively from hospital medical records. Laboratory parameters, including hematological indices, inflammatory markers, renal function tests, and coagulation profiles, were recorded preoperatively and during the early postoperative period. Imaging findings were obtained from contrast-enhanced CT angiography. Surgical details were extracted from operative reports. This case report was prepared in accordance with the CARE guidelines (CAse REports). Written informed consent for publication was obtained from the patient’s legal representative. The case is presented to highlight the clinical course, surgical decision-making, and postoperative outcomes of NTE following AMI in an elderly patient.
An 86-year-old female presented to the emergency department with sudden-onset severe abdominal pain accompanied by nausea and vomiting. She had a history of atrial fibrillation, hypertension, diabetes, and hyperlipidemia, and had undergone coronary stent placement five days earlier. On physical examination, the abdomen was distended, bowel sounds were hyperactive in the right lower quadrant, and diffuse abdominal tenderness with guarding was noted. Rectal examination revealed normal. Initial abdominal ultrasonography did not demonstrate any specific pathology but revealed the presence of free intraperitoneal fluid. Subsequent contrast-enhanced abdominal CT angiography showed restricted flow in the superior mesenteric artery (SMA) and edematous small bowel walls. To further clarify the etiology of the intra-abdominal fluid, ultrasound-guided paracentesis was performed, yielding turbid, serous fluid with a broth-like appearance, raising a strong suspicion for advanced intestinal ischemia. The patient’s contrast-enhanced abdominal CT angiography findings are shown in Figure 1.
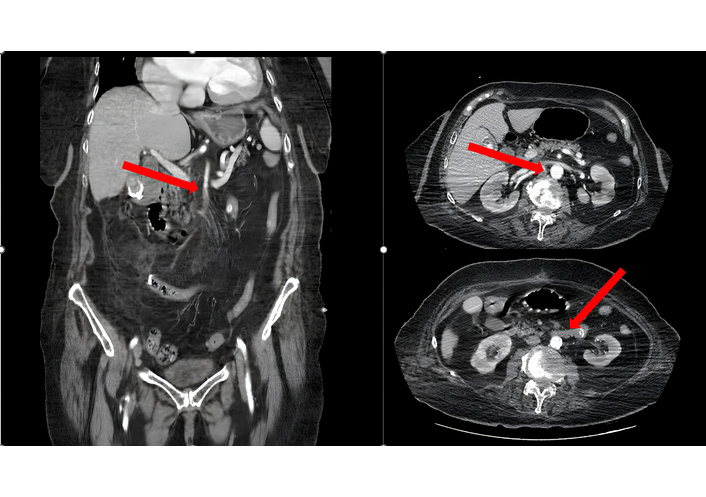
Contrast-enhanced abdominal CT angiography demonstrates paired perfusion of the superior mesenteric artery and edematous small bowel loops consistent with acute mesenteric ischemia. Red arrows indicate the areas of vascular compromise and bowel wall abnormalities suggestive of intestinal ischemia.
On admission, laboratory evaluation demonstrated marked leukocytosis [white blood cell (WBC): 14.5 × 103/µL] with neutrophil predominance and elevated inflammatory markers, such as C-reactive protein (CRP) (21.0 mg/L). Renal function parameters were initially within normal limits. The patient was admitted during the night, and emergency surgery was performed in the early hours of the following day after initial evaluation and stabilization.
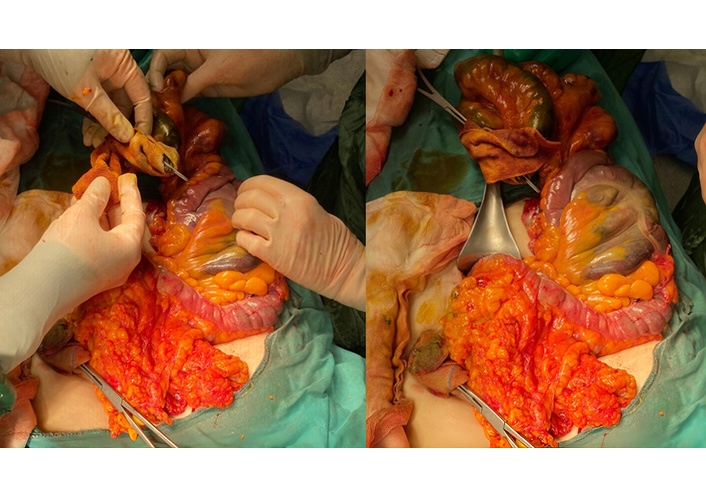
With a strong clinical suspicion of AMI, oral intake was stopped, and an emergency exploratory laparotomy was performed. Upon entering the abdomen, approximately 1,000 mL of turbid, serous intra-abdominal fluid was aspirated. Transmural necrosis of the small intestine was identified starting approximately 15 cm distal to the ligament of Treitz and extending distally to within 90 cm of the terminal ileum. There was no mesenteric arterial pulsation in the affected bowel segments, which suggests embolic occlusion of the jejunal and ileal branches of the SMA. After resection of the necrotic segments, approximately 15 cm of proximal jejunum and 90 cm of distal ileum (about 110 cm of total viable small bowel) were preserved. The colon remained viable, and a jejunoileal anastomosis was performed. The patient was transferred to the intensive care unit for postoperative monitoring. Extensive small bowel ischemia is demonstrated intraoperatively in Figure 2.
During the early postoperative period, the patient was under close clinical observation in the intensive care unit. Despite the initial surgical intervention, abdominal tenderness persisted. Laboratory evaluation revealed elevated inflammatory markers, with CRP levels rising from 21.0 mg/L to over 335 mg/L. The neutrophil-to-lymphocyte ratio (NLR) also increased significantly, indicating severe systemic inflammation. Perioperative laboratory findings and their clinical interpretation are summarized in Table 2.
Perioperative laboratory findings and clinical interpretation.
| Parameters | Preoperative (04.02.2024) | Early postoperative (06.02.2024) | Postoperative day 2 (07.02.2024) | Reference range | Clinical interpretation |
|---|---|---|---|---|---|
| WBC (× 103/µL) | 14.5 | 11.4 | 6.46 | 4.5–11 | Initial leukocytosis consistent with acute ischemia; normalization post-surgery. |
| Neutrophils (× 103/µL) | 11.08 | 10.37 | 5.75 | 1.8–7.7 | Marked neutrophilia reflecting severe inflammatory response. |
| Lymphocytes (× 103/µL) | 2.49 | 0.62 | 0.40 | 1.2–3.9 | Progressive lymphopenia indicates systemic stress and poor prognosis. |
| NLR (ratio) | 4.45 | 16.73 | 14.38 | - | Extremely elevated NLR associated with bowel necrosis and mortality. |
| CRP (mg/L) | 21.0 | 335.5 | 328.6 | < 5 | Severe systemic inflammation due to mesenteric ischemia and necrosis. |
| Hemoglobin (g/dL) | 11.0 | 11.3 | 9.5 | 11.7–16.1 | Postoperative anemia following major bowel resection. |
| Platelets (× 103/µL) | 218 | 260 | 188 | 150–400 | Preserved platelet count. |
| Creatinine (mg/dL) | 0.83 | 1.47 | 2.45 | 0.5–0.9 | Progressive AKI postoperatively. |
| eGFR (mL/min) | 63.7 | 32.3 | 17.3 | ≥ 90 | Worsening renal function consistent with multiorgan dysfunction. |
| AST (U/L) | 43 | 32 | 34 | 5–34 | Mild ischemic hepatocellular injury. |
| ALT (U/L) | 32 | 27 | 22 | 0–55 | Within normal limits. |
| LDH (U/L) | 626 | - | - | 125–220 | Markedly elevated, reflecting tissue ischemia and necrosis. |
| Amylase (U/L) | 155 | - | - | 28–100 | Elevated, likely secondary to intestinal ischemia. |
| INR | - | 1.56 | 1.66 | 0.8–1.2 | Coagulopathy associated with ischemia and anticoagulation. |
| aPTT (sec) | - | 45.1 | 38.4 | 22–30 | Prolonged due to anticoagulation and systemic inflammation. |
Clinical note: Markedly elevated CRP and NLR values were consistent with extensive bowel necrosis and poor prognosis. AKI: acute kidney injury; ALT: alanine aminotransferase; aPTT: activated partial thromboplastin time; AST: aspartate aminotransferase; CRP: C-reactive protein; eGFR: estimated glomerular filtration rate; INR: international normalized ratio; LDH: lactate dehydrogenase; NLR: neutrophil-to-lymphocyte ratio; WBC: white blood cell.
Perioperative trends of CRP and NLR showed a pronounced and persistent elevation following extensive bowel ischemia and NTE, reflecting ongoing systemic inflammation and unfavorable prognosis, as illustrated in Figure 3.
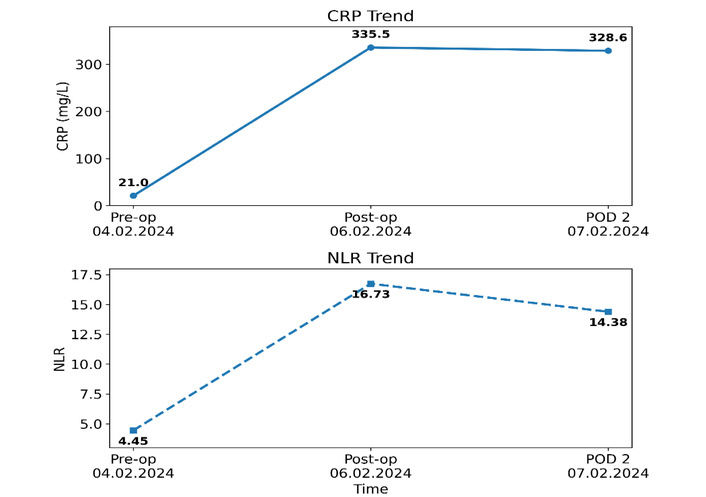
Temporal changes in C-reactive protein (CRP) and neutrophil-to-lymphocyte ratio (NLR).
Due to persistent abdominal symptoms and deteriorating laboratory results, ongoing intestinal ischemia was suspected, and a second laparotomy was deemed necessary. Second-look surgery was performed under general anesthesia through the previous midline incision. An intraoperative examination revealed ischemia affecting the jejunoileal anastomosis and extending to the distal ileum, the ileocecal junction, the cecum, the ascending colon, the hepatic flexure, and the right transverse colon. The liver, stomach, spleen, left transverse colon, splenic flexure, descending colon, sigmoid colon, and rectum were viable. Ileal resection, including the jejunoileal anastomosis, and an extended right hemicolectomy were performed. However, due to the extremely limited remaining length of the small intestine, restoring bowel continuity was not possible. Thus, a jejunostomy was created approximately 10 cm distal to the ligament of Treitz to facilitate drainage. Adequate hemostasis was achieved, abdominal drains were placed, and the abdomen was closed in anatomical layers. The surgical findings and related procedures are summarized in Table 3.
Operative findings and surgical interventions.
| Time point | Findings | Surgical intervention |
|---|---|---|
| 05.02.2024 Initial surgery | Approximately 1,000 mL of serous intra-abdominal fluid; transmural necrosis of the jejunum and ileum beginning approximately 15 cm distal to the ligament of Treitz and extending distally to about 90 cm proximal to the terminal ileum; absent mesenteric pulsation suggesting embolic occlusion of the jejunal and ileal branches of the superior mesenteric artery | Emergency exploratory laparotomy; near total enterectomy with preservation of approximately 110 cm of viable small bowel (15 cm proximal jejunum and 90 cm distal ileum); stapled jejunoileal anastomosis; resection of necrotic bowel with mesentery; abdominal irrigation and JP drain placement |
| 06.02.2024 Second-look laparotomy | Progressive ischemia involving the ileocecal junction and right colon | Extended right hemicolectomy and feeding jejunostomy placement |
The patient required prolonged multidisciplinary management, including total parenteral nutrition (TPN) as the sole means of nutritional support, as well as anticoagulation, fluid and electrolyte replacement, and supportive medical therapy. She experienced multiple complications during her hospital stay, including recurrent infections, catheter-related issues, metabolic disturbances, and cholestatic liver dysfunction. These complications necessitated repeated medical evaluations and specialty consultations.
Throughout the follow-up period, the patient was unable to tolerate any oral nutrition. Her oral intake was limited to small amounts of fluids for comfort, including water and the occasional cup of coffee, neither of which contributed any calories or enteral nutrition. After gradual clinical stabilization, she was discharged on long-term home parenteral nutrition with continued follow-up and supportive care. Despite these measures, she developed recurrent infections and metabolic complications during follow-up and ultimately died at home six months after the initial surgery.
Diagnostic findings are summarized in Table 4.
Perioperative laboratory and diagnostic findings.
| Parameter | Preoperative | Postoperative | Reference range | Interpretation |
|---|---|---|---|---|
| WBC | 14.5 ×103/µL | ↑↑ | 4–10 | Leukocytosis |
| CRP | 21 mg/L to > 335 mg/L | Markedly ↑ | < 5 | Severe inflammation |
| NLR | Elevated | Further ↑ | - | Systemic inflammatory response |
| CT angio | SMA hypoperfusion | - | - | Suggestive of AMI |
| Paracentesis | Turbid fluid | - | - | Advanced ischemia |
AMI: acute mesenteric ischemia; CRP: C-reactive protein; CT: computed tomography; NLR: neutrophil-to-lymphocyte ratio; SMA: superior mesenteric artery; WBC: white blood cell.
Due to the patient’s advanced age and clinical condition, direct subjective reporting was limited. However, according to her caregivers, the patient experienced severe abdominal pain and distress at presentation, significantly affecting her comfort and daily functioning.
Following surgical interventions, although temporary stabilization was achieved, the prolonged dependence on parenteral nutrition and recurrent complications posed a substantial burden. The family expressed appreciation for the life-prolonging interventions despite the challenging clinical course.
AMI is a life-threatening vascular emergency characterized by abrupt interruption of intestinal blood flow, with mortality rates remaining exceedingly high, particularly in cases of delayed diagnosis and advanced bowel necrosis. In the present case, the clinical presentation and the presence of multiple cardiovascular comorbidities, most notably atrial fibrillation, strongly supported an embolic etiology involving the SMA, most commonly originating from the left atrium [1]. Intraoperative findings of extensive jejunoileal necrosis and absence of mesenteric arterial pulsation further confirmed this mechanism (Table 5).
Selected reports on AMI requiring NTE and postoperative outcomes.
| Author (year) | Study type | Patient population | Surgical extent | Nutritional support | Outcome |
|---|---|---|---|---|---|
| Bala et al. (2017) [7] | Guidelines/Review | AMI (mixed etiology) | Extensive bowel resection discussed | PN is recommended in IF | High mortality: survival is possible in selected cases |
| Clair and Beach (2016) [1] | Narrative review | AMI, embolic and thrombotic | Extensive resection, including NTE reported | Long-term PN required | Survival rare but documented |
| Acosta (2015) [14] | Review | AMI patients | Massive bowel necrosis | PN emphasized in survivors | Poor prognosis, high morbidity |
| Pironi et al. (2015) [15] | Consensus statement (ESPEN) | Adult intestinal failure | Near total or extensive bowel loss | Long-term PN standard of care | Survival is possible with PN; outcomes depend on remnant bowel anatomy and comorbidities |
| Amiot et al. (2013) [16] | Cohort study | Non-malignant short bowel syndrome (intestinal failure) | Extensive small bowel resection | Home PN | Long-term survival is achievable; outcomes are influenced by remnant bowel anatomy and comorbidities |
AMI: acute mesenteric ischemia; ESPEN: European Society for Clinical Nutrition and Metabolism; IF: intestinal failure; NTE: near total enterectomy; PN: parenteral nutrition; SBS: short bowel syndrome.
Elderly patients with comorbid conditions such as hypertension, diabetes mellitus, hyperlipidemia, and atrial fibrillation represent a particularly vulnerable population. As illustrated in this case, the nonspecific nature of early symptoms may lead to diagnostic delay, as alternative etiologies are often prioritized in this age group. These findings underscore the importance of maintaining a high index of suspicion and promptly integrating clinical, laboratory, and imaging findings for early diagnosis in high-risk patients [4].
Early intervention remains the cornerstone of AMI management and has a decisive impact on survival. Standard treatment includes aggressive resuscitation, anticoagulation, broad-spectrum antibiotics, and urgent surgical exploration when bowel necrosis is suspected. In advanced disease stages, extensive ischemia may necessitate NTE, as observed in the present case, significantly increasing the risk of short bowel syndrome and long-term nutritional dependency [17].
Beyond the clinical and surgical aspects, this case highlights the potential prognostic relevance of readily available inflammatory biomarkers. Markedly elevated CRP levels and a pronounced increase in the NLR were observed during the perioperative period. Persistent elevation of these markers reflected ongoing systemic inflammation and paralleled the aggressive clinical course despite surgical intervention. These findings suggest that CRP and NLR may serve as dynamic and accessible indicators of disease severity, postoperative inflammatory burden, and prognosis in AMI. Their integration into clinical assessment may facilitate early identification of patients at high risk for deterioration and support timely decision-making.
Reported mortality rates for AMI range between 50% and 70% and are influenced by factors such as diagnostic delay, patient age, physiological reserve, and the extent of bowel necrosis [18]. Patients requiring extensive intestinal resection, particularly those undergoing NTE, represent a subgroup with an exceptionally poor prognosis. Nevertheless, recent advances in perioperative critical care, surgical techniques, and nutritional support have challenged the historically fatal perception of this condition.
NTE remains a rare but critical surgical scenario and is likely underreported in the literature. Massive bowel devascularization represents a common terminal pathway in advanced AMI [19]. While previously considered incompatible with survival, emerging evidence suggests that selected patients may achieve short- to mid-term survival when aggressive surgical management is combined with intensive postoperative care and long-term parenteral nutrition [20]. However, this approach is associated with substantial morbidity, including recurrent infections, catheter-related complications, metabolic disturbances, and hepatobiliary dysfunction.
In the present case, prolonged survival following NTE was achieved through multidisciplinary management, including intensive care support and long-term parenteral nutrition. However, the patient’s course was complicated by persistent systemic inflammation, progressive metabolic disturbances, and recurrent infections, ultimately leading to death six months after the initial surgery. These findings are consistent with existing literature indicating that long-term outcomes are primarily determined by complications related to intestinal failure and chronic systemic inflammation [18].
This case also reflects a broader shift in the management paradigm of embolic AMI. Historically, extensive intestinal necrosis was frequently managed with palliative intent due to the perceived futility of surgical intervention. However, advances in modern critical care and nutritional support have made survival possible even after extreme resections such as NTE. In this evolving context, simple and widely available biomarkers such as CRP and NLR may provide valuable adjunctive information by reflecting the extent of ischemic injury and systemic inflammatory response.
Finally, operative decision-making in such critically ill patients remains highly complex and must balance physiological status, expected quality of life, and patient or family preferences. While intestinal transplantation represents a potential definitive treatment for selected patients with irreversible intestinal failure, its applicability remains limited [21, 22].
Overall, this case underscores the devastating nature of AMI complicated by extensive bowel necrosis, while simultaneously demonstrating that survival, although limited, may be achievable with aggressive surgical and supportive management. It further highlights the potential role of inflammatory biomarkers as adjunctive tools in risk stratification and clinical decision-making in this extremely severe clinical entity [1, 7, 14–16].
In conclusion, this case demonstrates that survival following NTE due to AMI, although historically considered incompatible with life, may be achievable with advances in surgical and critical care management.
However, the clinical course remains highly complex and is frequently complicated by severe systemic inflammation, multiorgan dysfunction, and long-term dependence on parenteral nutrition.
This case highlights the critical importance of:
early diagnosis,
timely surgical intervention,
and meticulous multidisciplinary postoperative care.
Furthermore, readily available inflammatory biomarkers such as CRP and NLR may serve as practical adjunctive tools for assessing disease severity and guiding clinical decision-making in this high-risk population.
AMI: acute mesenteric ischemia
CRP: C-reactive protein
CT: computed tomography
NLR: neutrophil-to-lymphocyte ratio
NTE: near total enterectomy
SMA: superior mesenteric artery
TPN: total parenteral nutrition
WBC: white blood cell
EY: Conceptualization, Visualization, Supervision, Investigation, Validation, Writing—original draft, Writing—review & editing. ASS: Investigation, Writing—original draft, Writing—review & editing. KK: Investigation, Writing—original draft, Writing—review & editing. CF: Investigation, Writing—original draft, Writing—review & editing. ANS: Investigation, Writing—original draft, Writing—review & editing. AS: Conceptualization, Supervision, Investigation, Writing—original draft, Writing—review & editing, Visualization. OO: Conceptualization, Supervision, Investigation, Writing—original draft, Writing—review & editing. HU: Conceptualization, Supervision, Investigation, Writing—original draft, Writing—review & editing. All authors read and approved the submitted version.
There are no conflicts of interest.
This case report was conducted in accordance with the World Medical Association Declaration of Helsinki. Institutional Review Board approval from the Istanbul Atlas University for Medical Sciences was not required for the publication of a single de-identified case report in accordance with institutional policy.
Informed consent to participate in the study was obtained from the patient.
Informed consent to publication was obtained from the relevant participant, including consent for publication of any accompanying images.
The datasets used and/or analyzed during the current study are available from the corresponding author on a reasonable request.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 1777
Download: 12
Times Cited: 0