Case Report
Case Report

Affiliation:
1Programa de Doctorado en Investigación Clínica, Instituto de Investigación Sanitaria del Principado de Asturias,Universidad de Oviedo, 33011 Oviedo, Spain
Affiliation:
2Faculty of Physiotherapy, University of Valencia, 46010 Valencia, Spain
Email: carlos.forneralvarez.pt@gmail.com
ORCID: https://orcid.org/0009-0006-1575-1589
Affiliation:
3Servicio de Rehabilitación, Instituto de Investigación Sanitaria Fundación Jiménez Diaz (IIS-FJD, UAM), Hospital Universitario Rey Juan Carlos, 28040 Madrid, Spain
Affiliation:
4Department of Physiotherapy, University of Valencia, 46010 Valencia, Spain
ORCID: https://orcid.org/0000-0003-4644-3758
Affiliation:
5Departamento de Cirugía, Ciencias Médicas y Sociales, Facultad de Medicina, Universidad de Alcalá, 28871 Alcalá de Henares, Spain
6Grupo de Investigación Clínico-Docente sobre Ciencias de la Rehabilitación (INDOCLIN), Centro Superior de Estudios Universitarios La Salle, 28023 Madrid, Spain
ORCID: https://orcid.org/0000-0002-1056-7305
Explor Neuroprot Ther. 2025;5:1004102 DOI: https://doi.org/10.37349/ent.2025.1004102
Received: December 15, 2024 Accepted: April 11, 2025 Published: April 26, 2025
Academic Editor: Rafael Franco, Universidad de Barcelona, Spain
Chronic upper limb pain is rather common among people in general and is characterized by a complex diagnosis due to the wide variety of factors that are involved in its development. In terms of treatment, pharmacology and manual therapy have classically been the most used options. However, based on current evidence, recommendations are more inclined to apply multimodal treatments, mainly with exercise therapy and pain education, based on the patient-centered care model. This case report details the evaluation and treatment of a 23-year-old woman with chronic upper limb pain using a multimodal physical therapy with a biobehavioral approach. The intervention lasted 12 weeks with a total of 9 sessions, in which manual therapy, therapeutic exercise, pain neuroscience education, motion representation methods, and sensory retraining were applied. The treatment resulted in a substantial improvement in the patient’s health condition. This case report indicates that a multimodal physical therapy treatment based on a biobehavioral approach may offer benefits in reducing pain symptoms and enhancing somatosensory, motor-functional, and affective-cognitive abilities in patients with chronic upper limb pain, as observed in the described case. Accordingly, this treatment can be a therapeutic option for patients with chronic upper limb pain.
Chronic upper limb pain (CULP) is relatively prevalent in the general population and is associated with physical dysfunction in patients [1]. Some studies estimate that about 30% of the population will suffer from CULP [2], which increases with age and varies depending on some factors related to activity, being more frequent in those with jobs that involve repetitive movements or intensive use of the hands [3].
The diagnosis of CULP is often complex due to the variety of factors that contribute to its development. Musculoskeletal injuries have been traditionally linked with diagnosed disorders such as shoulder tendinitis, adhesive capsulitis, lateral epicondylitis, and more specifically, when dealing with hand pain, carpal tunnel syndrome or de Quervain’s disease [4]. However, psychosocial factors and patient context have been identified as prognostic factors in this type of disorder [5, 6], therefore, these factors may play an important role in the management of CULP.
Regarding treatments, traditional approaches to the treatment of chronic pain have included the use of pharmacology and manual physical therapy techniques [7]. However, recent evidence suggests that interventions combining pain neuroscience education (PNE) and therapeutic exercise (TE) may have more lasting effects on reducing pain and improving function in these complex patients [8–10]. Furthermore, integrating an appropriate, well-designed, biopsychosocial model, has been shown to offer a promising framework for the comprehensive care of individuals with musculoskeletal pain conditions [11].
This case report describes a multimodal physiotherapy treatment approach grounded in a biobehavioral perspective for a patient with CULP. It is one of the first studies to utilize a biobehavioral framework for this patient profile, contrasting with more traditional physiotherapy methods, which had not provided any previous improvement to the patient presented. Thus, the objective of this case report was to describe the assessment and treatment of an actual patient with CULP by using a multimodal physical therapy treatment based on a biobehavioral approach, as such an approach is grounded in a patient-centered biobehavioral model.
The patient was a 23-year-old woman who had been experiencing chronic pain for a duration of 1 year and 2 months. The reason for consultation was the presence of pain in her right hand with irradiation to the forearm. Besides, she also presents with neck pain. Her injury mechanism occurred while working, catching an object. Since then, she began to feel pain and was functionally impaired in her hand.
The patient did not present any relevant medical history or condition. In the first instance, after a few days since the acute episode, a simple wrist radiography did not find any signs of injury. After a month, during which pain persisted, she underwent a local imaging study by ultrasound, with no conclusions, and a magnetic resonance, with no findings. Subsequently, the patient received a medical diagnosis of early wrist osteoarthritis and had her arm immobilized for 4 months. After that, she presented incapacitating symptoms while writing, night awakenings, and upon waking up in the morning. Because of that, she attended a doctor’s consultation again (11 months since the episode) and she underwent a bone scintigraphy that revealed “bone inflammation in both hands”. The medical assistance concluded here, with no study of other regions, advising not to “force” the hand when dealing with pain and to think about changing jobs.
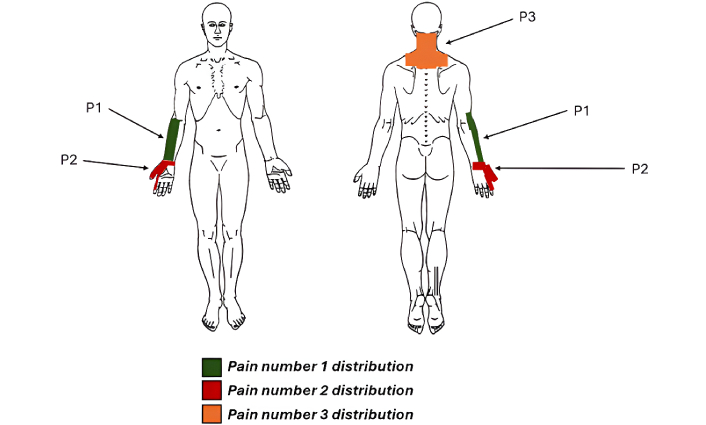
The primary symptomatology reported by the patient during the initial interview included three distinct pain locations: pain in the thumb and hand (P1), pain in the anterior and lateral aspects of the forearm (P2), and neck pain (P3). The intensity of these pains was assessed using a Visual Analogue Scale (VAS). P1 was assigned a VAS score of 6.5/10. She described it as deep and constant, with no relief maneuvers and worsening when writing or picking up something heavy. P2 had a VAS score of 3/10. It was described as superficial, mechanical, with tingling to the elbow and associated with P1. It improved with myofascial treatment. P3 received a VAS score of 5/10. It was described as superficial and constant, with no relationship with the others, and improving with rest while worsening with stress and mechanical load. The baseline body chart, illustrating the distribution of symptoms, along with pre-intervention measurements of pain characteristics, is provided in Figure 1.
Following the medical interview, a physical examination was conducted. Concerning P1, it was observed that both active and passive movements of the trapeziometacarpal joint elicited pain, in addition to anteroposterior mobilization. The distal radioulnar joint was also checked, noticing pain with active dorsal flexion, passive dorsal flexion with radial deviation, and showing congruence with the instability model. No symptoms were found at the elbow evaluation. Regarding P2, both radial and median nerve tension tests were positive. Because the assessment focused on the affected arm and hand, and considering the patient’s purpose of consultation, P3 did not undergo a physical exploration at first instance. The baseline values for all assessed pain levels are detailed in Table 1.
Pre-intervention and post-intervention measurements
| Measure | Pre-intervention | Post-intervention | |
|---|---|---|---|
| Pain (VAS) | Right hand | 6.5/10 | 0/10 |
| Right forearm | 3/10 | 0/10 | |
| Neck | 5/10 | 0/10 | |
| 2-PDT (cm) | Right | 4 | 1.5 |
| Left | 2 | 1.5 | |
| TS (VAS) | Right LE | 1.3/10 | 0/10 |
| Right thumb | 0/10 | 0/10 | |
| Strength (kg) | Right | 12 | 29.5 |
| Left | 19 | 31.5 | |
| Neck disability (NDI) | 13/55 | 7/55 | |
| Upper limb disability (DASH) | 38/55 | 22/55 | |
| Quality of life (SF-36) | 7/20 | 4/20 | |
| Pain catastrophizing (PCS) | 12/52 | 4/52 | |
| Kinesiophobia (TSK-11) | 20/44 | 13/44 | |
VAS: Visual Analogue Scale; 2-PDT: two-point discrimination test; TS: temporal summation; LE: lateral epicondyle; NDI: Neck Disability Index; DASH: Disabilities of the Arm, Shoulder and Hand; PCS: Pain Catastrophizing Scale; TSK-11: 11-item Tampa Scale of Kinesiophobia
The strength of both upper limbs was assessed using a hand-held dynamometer, which expressed the results in kilograms. The baseline values of the strength assessment are described in Table 1.
Secondly, a somatosensory assessment was conducted. Using an esthesiometer, the two-point discrimination test (2-PDT) was conducted. In accordance with the protocol outlined by Nolan [12], the calipers were initially set at 70 mm, and the distance between the points was progressively reduced by 10 mm until the patient reported perceiving only one point instead of two. The test was performed on both the right and left radial styloids.
Subsequently, the time summation magnitude was evaluated using Von Frey monofilaments. Additionally, the test was carried out on the right thumb and epicondyle. At the outset of the test, a primary stimulus was applied using monofilaments to one of the designated points. The patient was then asked to rate the intensity of the pain induced by the stimulus using the VAS scale. Subsequently, 10 rhythmic stimuli were administered to the same point, guided by a metronome set at 60 bpm. Finally, the difference between the mean of three repetitions of a single stimulus and the mean of three repetitions of ten stimuli was calculated. The result of this calculation represents the value of the temporal summation (TS) effect [13, 14]. Besides, the hand grip capacity of both hands was measured using dynamometry. All baseline measures of the somatosensory factors can be found in Table 1.
Finally, the affective-cognitive status was evaluated using several instruments. The Spanish version of the Neck Disability Index (NDI) was employed to assess the patient’s level of disability caused by neck pain. It is composed of 10 items, each of which is adjustable on a scale from 0 to 5. Depending on the total score, the patient can be stratified into one of the five levels of disability [15]. The Spanish version of the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire was conducted to assess the patient’s level of disability induced by the upper limb pain. It consists of 30 items and grades the patient’s disability from 0 to 100 [16]. Patient’s quality of life was measured using the SF-36 questionnaire. The SF-36 health questionnaire is composed of 36 items that aim to collect all the relevant aspects to characterize the health of an individual. With these questions, it is intended to cover at least 8 aspects or dimensions: physical function, physical role, pain, general health, vitality, social function, emotional role, and mental health. [17]. Pain catastrophizing was measured using the Spanish version of the Pain Catastrophizing Scale (PCS), which consists of 13 questions, yielding a maximum score of 52 points. A higher score indicates greater catastrophizing. A significant change is defined as a difference in the PCS score exceeding 9.1 points [18]. Additionally, the Spanish version of the 11-item Tampa Scale of Kinesiophobia (TSK-11) was used to assess kinesiophobia. The TSK-11 is scored between 11 and 44, with higher scores indicating a greater degree of kinesiophobia. A change greater than 5.6 points in the TSK-11 is considered clinically significant [19].
All baseline values for the aforementioned affective-cognitive assessments are provided in Table 1.
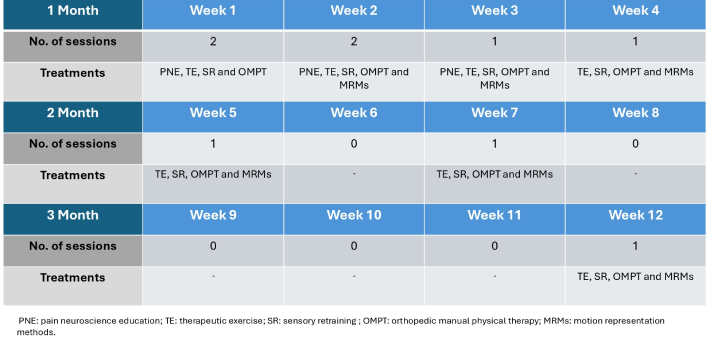
The therapeutic intervention lasted 3 months. The patient agreed to undergo the treatment and signed the informed consent documents for treatment, data protection, and permission for academic use, and consent for telephone and e-mail communications. Over the course of the 12-week treatment period, the patient attended a total of 9 sessions, with each session lasting approximately 60 minutes. During the first two weeks, the patient attended two sessions per week, while from the third to the fourth week, the rehabilitation was carried out once a week. After that, in the second month of treatment, she received one session every 15 days, and finally, in the third month, she received only one session. The biobehavioral physiotherapy approach included PNE, motion representation methods (MRMs), orthopedic manual physical therapy (OMPT), TE, and sensory retraining (SR). All the modules were gradually supplied from session one, except MRM, which was implemented in the second week. Figure 2 contains the schedule of sessions. As for PNE, it was applied during the first 5 sessions. The contents implemented were as follows: session 1: pain and context; session 2: influence of psychosocial factors on pain; session 3: peripheral and central sensitization; session 4: neuroplasticity; and session 5: benefits of TE. Regarding the OMPT used, this included neural mobilization and joint mobilization techniques. As for TE, it contained both unloaded and loaded exercises, the latter using mainly elastic bands. In terms of SR, the focus was on improving sensitivity to vibration, touch, and pressure. Finally, the MRMs used were action observation, motor imagery, and mirror therapy.
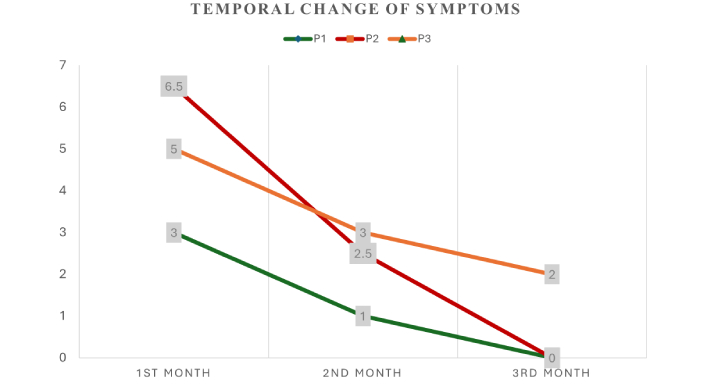
Regarding the overall results of the treatment, a significant improvement in the patient’s condition was achieved. As for the pain, both P1 and P2 disappeared. P3, despite not receiving a “topographic” approach, also remitted a favourable response by attaining adequate pain relief. In addition, the somatosensory, motor-functional, and affective-cognitive factors were rated below the basal point. Table 1 shows all the measurements collected after the intervention in detail. In addition, Figure 3 shows a graph depicting the temporal change of the patient’s symptoms over time.
This case report provides a comprehensive description of the multimodal physiotherapy treatment administered to an adult female patient with CULP, along with the results achieved. The proposed treatment successfully eliminated the intensity of pain. Furthermore, significant improvements were observed in the somatosensory, motor-functional, and affective-cognitive abilities.
In the literature, there are other case reports in which physiotherapy has been employed to alleviate hand pain, such as the case described by Özüdoğru and Ceylan [20]. In contrast to our report, this case focuses on a more conventional approach to physiotherapy, utilizing only passive techniques.
Moreover, this is not the first time that this approach is able to obtain significant improvements in a patient with chronic pain. There are previous reports focused on chronic non-specific neck pain [21], which have gotten positive results. Marcos-Martín et al. [22] and Forner-Álvarez et al. [23] also obtained significant improvements when applying this kind of multimodal intervention in patients with chronic cervico-craniofacial pain and chronic low back pain, respectively.
Notwithstanding sharing the same basis of clinical reasoning and management, this report differs from the one mentioned above, and other ones reported, in some key points. Firstly, the patient presented with chronicity in topographically separated locations. Despite there is plenty of literature describing the link between upper limb and neck disfunctions [24], this patient’s clinical history implied greater complexity when reasoning and subsequent decision-making.
Furthermore, despite having literature that explores the biopsychosocial approach to address the loss of upper limb functionality [25], the literature has traditionally focused on structural reasoning approaches when dealing with hand pain [26] that persist to our days [27], proposing frameworks which leave aside patients who are not governed by provocative orthopedic tests, as the one presented in this case. In this sense, this report provides a correct management guide aligned with the proposed biopsychosocial approach, which has previously been successful in other pathologies, and which here demonstrates to do so in the same way.
As for the motor-functional aspect, focusing on hand strength, the significant improvement in this outcome after the implementation of the therapeutic intervention may be caused mainly by TE, as seen in the current literature [28–30].
Regarding the somatosensory factors, some studies have pointed out that these factors are directly related to the symptoms of pain, such as intensity or expansion [31, 32]. Therefore, the significant pain score regression presented in this case could be linked to the somatosensorial management developed. In line with our proposal, the use of the MRMs has been used before in other kinds of conditions dealing with upper limb disfunction, achieving positive results [33, 34].
As for the affective-cognitive aspects, multimodal intervention based on TE and PNE may explain the results obtained. Similar to previous literature, besides its hypoalgesic effect [35], TE has been employed as a useful tool, expecting to downgrade the patient’s disability [36]. Otherwise, the improvement observed in catastrophism or kinesiophobia could be partly explained by the employment of the PNE [37].
From a broader perspective, considering the combined effects of these techniques, the therapeutic potential of the biopsychosocial model in generating neurophysiological changes is highly relevant to clinicians. Since chronic pain induces changes in the neurocognitive domain [38], physiotherapists’ clinical reasoning should be guided by models aimed at producing central-level changes [39, 40]. Strong evidence already supports the added benefits of combining therapies within this model, such as exercise and education [41, 42] or showing how manual therapy can be applied not merely to achieve peripheral effects on the treated area but rather to modulate the pain process under this framework, emphasizing the patient’s interpretative process as a key factor to achieve these neurophysiological goals [43, 44].
This case report presents certain limitations that should be acknowledged. First, the absence of long-term follow-up limits our awareness of sustained effectiveness. We believe that extending a regular follow-up would provide a more concrete understanding, especially given the chronic nature of their condition. Secondly, because of the study design, this report is not appropriate to extrapolate results to other patients or broad generalizations of the effect of the intervention. Finally, since this is merely a case report, it will be necessary to conduct a study in the future involving a larger cohort of patients.
In conclusion, this case report highlights the effectiveness of a multimodal physiotherapy treatment based on a biobehavioral approach for managing CULP. By employing a patient-centered model, the intervention successfully alleviated pain intensity while also enhancing somatosensory, motor-functional, and affective-cognitive abilities. These findings support the integration of biobehavioral strategies in physiotherapy to address both the physical and psychological aspects of chronic pain, ultimately improving patient outcomes.
CULP: chronic upper limb pain
DASH: Disabilities of the Arm, Shoulder, and Hand
MRMs: motion representation methods
OMPT: orthopedic manual physical therapy
PCS: Pain Catastrophizing Scale
PNE: pain neuroscience education
SR: sensory retraining
TE: therapeutic exercise
TSK-11: 11-item Tampa Scale of Kinesiophobia
VAS: Visual Analogue Scale
FBBF, CFÁ, CVQ, and FCM: Methodology, Supervision, Validation, Writing—original draft, Writing—review & editing. MGA: Conceptualization, Methodology, Supervision, Validation, Visualization, Project administration, Writing—original draft, Writing—review & editing.
The authors declare that they have no conflicts of interest.
According to the Centro Superior de Estudios Universitarios (CSEU) La Salle regulations, ethical approval is not required for this article.
Informed consent to participate in the study was obtained from the participant.
Informed consent to publication was obtained from the relevant participant.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.