Review
Review

Affiliation:
1Department of Clinical Immunology and Rheumatology, Kalinga Institute of Medical Sciences, Bhubaneswar 751024, India
ORCID: https://orcid.org/0000-0002-1278-6042
Affiliation:
1Department of Clinical Immunology and Rheumatology, Kalinga Institute of Medical Sciences, Bhubaneswar 751024, India
ORCID: https://orcid.org/0000-0003-4631-311X
Affiliation:
2Department of Clinical Immunology and Rheumatology, Christian Medical College, Vellore 632002, India
Email: debashisdandacmc@hotmail.com
ORCID: https://orcid.org/0000-0002-2121-0942
Explor Musculoskeletal Dis. 2024;2:20–30 DOI: https://doi.org/10.37349/emd.2024.00030
Received: August 01, 2023 Accepted: November 09, 2023 Published: January 22, 2024
Academic Editor: Fernando Pérez-Ruiz, Cruces University Hospital, Spain
The article belongs to the special issue Digital health technologies in rheumatology: emerging evidence and innovation
Remote monitoring technologies (RMTs) are an emerging tool for assessing, monitoring, and following up on patients with chronic diseases including autoimmune rheumatic diseases (AIRDs). The best use of these exponentially expanding technologies warrants optimum evidence. Rheumatoid arthritis (RA) is a chronic inflammatory process that requires close monitoring of disease activity, response to treatment, and the potential adverse effects. Though there are several studies that have explored RMTs in RA, there is little head-to-head comparison between the individual technologies or the standard of care. Before investing in potentially high-cost strategies like RMTs, it is prudent to estimate their pragmatic role in the management and potentially with long-term follow-up including drug titration. A thorough search of the literature was conducted across PubMed/MEDLINE, Scopus, and WebOfScience databases for recent and relevant literature looking at the acceptance, practical utility, and outcomes in RA using RMTs. This scoping review aims to summarize the current level of evidence in favor of RMTs, estimate real-world benefits and costs, potential hazards and limitations, and finally, identify future studies needed before endeavoring to mainstream RMTs. It emphasizes randomized trials using RMTs, patients reported outcomes and disparities in the usage of RMTs.
Rheumatoid arthritis (RA) is a chronic inflammatory arthritis that imposes a significant healthcare and economic burden on patients. Treatment-to-target approaches can dramatically improve outcomes. However, the patient-to-rheumatologist ratio is a major barrier that restricts the ability of timely and adequate follow-up [1]. Due to the progressive nature of uncontrolled disease or an aggressive phenotype, these individuals require close monitoring for disease activity, progression, and surveillance of adverse events. However, in low-income states and remote areas with limited or restricted access to healthcare, telephonic or digital remote disease monitoring can be a valuable tool [2].
Remote monitoring technologies (RMTs) are among the emerging tools for assessing, monitoring, and following up on patients with chronic diseases including autoimmune rheumatic diseases (AIRDs) [2–5]. These technologies can take the form of telemedicine, smartphone applications, wearables like health watches, etc. Internet usage has expanded exponentially to reach the remotest areas, and smartphones are now easily and affordably accessible. It is not uncommon for patients with chronic diseases, especially RA, to experience frequent relapses, which can be multifactorial in nature. Speciality access, such as rheumatology, is often concentrated in urban areas, which can pose a logistical challenge for patients in remote areas who require regular follow-up. RMT is a valuable tool that can help to bridge this gap.
Beyond teleconsultation, there has been growing interest in the development and usage of mobile applications to monitor health. Usage of these Apps is fairly versatile, covering arenas from disease activity measurement and calculation of disease activity indices with clear questionnaires (RheumaHelper) to data storage and retrieval, facilitation of connection of different people living with RA to facilitate formation of self-help groups, etc. [4].
RMT in the context of AIRDs and RA management is relatively new and the evidence available is scattered and scarce. With the advent of novel and more convenient methods of storage, integration and analysis of large data, there is a recent rise in the usage of remote monitoring apps and other digital tools to capture health data, disease progression and response to therapy electronically. Based on the model of continuous glucose monitoring (CGM), daily logging of health assessment as perceived by the patient can be done and this data can be captured to optimize therapy to obtain maximal response to treatment.
Remote health monitoring technologies have been predominantly used in the field of cardiology, cardiovascular medicine, oncology, however, their extension in rheumatology has not been popularized yet. The aim of this review is to explore the usage of RMTs in AIRDs, particularly in RA, as this technology can add on to the therapeutic armamentarium that the rheumatologists possess to treat the disease, which may aid in conceptualizing and drafting mainstream guidelines for usage and effectiveness of RMTs in RA.
This scoping review mainly aimed to target randomized controlled trials (RCTs), systematic reviews and meta-analyses which assessed the usage of RMTs in the context of RA. However, due to the scarcity of published literature on this subject, observational studies, retrospective studies, and proof-of-concept studies were included. Relevant literature that was cross-referenced from the selected articles from the search was also incorporated in the review.
The literature search was based on the population, intervention, comparison, and outcome (PICO) guidelines and also in consultation with the Arksey and O’Malley [6] framework for scoping reviews [7]. The PICO framework is described below:
Population—Patients with RA, in whom digital or mobile health (mHealth) monitoring and/or telemedicine was incorporated in the course of management.
Intervention—Usage of RMTs in the management of RA.
Comparison—There was no specific comparison, however, some studies included have compared RMTs with traditional in-person clinic monitoring.
Outcome—This involved patient reported outcomes, acceptance of remote health monitoring, adherence to the intervention and feasibility to employ it at a larger scale.
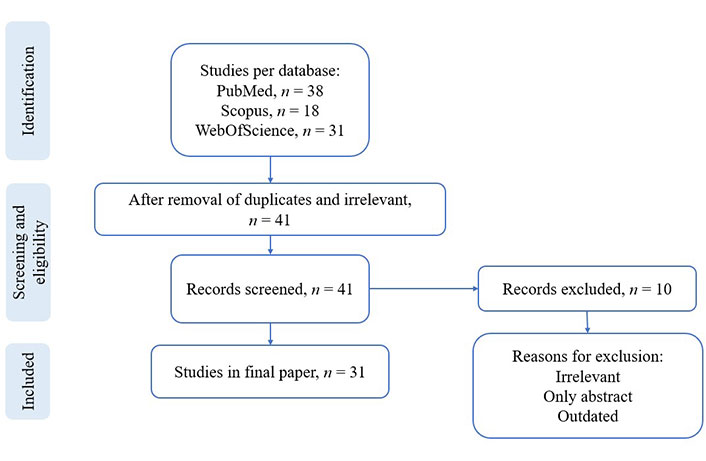
A thorough search of PubMed/MEDLINE, Scopus and WebOfScience databases with “Arthritis, Rheumatoid” AND “digital health” OR “remote monitoring” OR “telemedicine” OR “mHealth” in various combinations was conducted. Medical subject headings (MeSH) and full titles were used to conduct the search. The articles were screened for eligibility using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines and finally resulted in 31 articles for the scoping review, which is depicted in the flowchart (Figure 1) [8, 9]. Only the publications from the last 5 years were included. Publications in languages other than English and conference abstracts/proceedings were excluded. Other criteria for exclusion during study identification are depicted in the flowchart. The final list of extracted data from the selected articles is summarized in Table 1.
Summary of studies on RA starring remote health care
| Authors | Type of study | N (RA patients/apps reviewed) | Monitoring device | Outcome/Remarks |
|---|---|---|---|---|
| Azevedo et al. [5] (2015) | Cross-sectional | 100 | Willingness to use health-based assessment apps | Good compliance to apps |
| Barlas et al. [10] (2023) | Review article | 31 | Telemedicine, digital medicine, mHealth | PROMs showed good compliance, however, no significant difference between in-person consults. Data security is an issue |
| Chevallard et al. [11] (2021) | Retrospective | 431 | Tele-health with digital reporting of patient PROMs | General health and VAS was similar in patients who followed up digitally as compared to the ones who did an in-person clinic follow-up during COVID-19 |
| Colls et al. [12] (2021) | Observational | 78 | mHealth (electronic PRO app) | Good adherence, better remission rates |
| Cozad et al. [13] (2022) | Review article | 20 | mHealth apps | Better patient-centered care with mHealth apps, but better ones need to be developed in America |
| Dixon et al. [14] (2018) | Review article | NA | mHealth apps, EHRs | Summarized different EHRs and mHealth apps that can be integrated for better management |
| Doumen et al. [15] (2021) | Qualitative study | 58 | mHealth | Improved patient care, however, stakeholders felt that it can lead to negative-illness behavior |
| Fedkov et al. [16] (2022) | Prospective pilot | 17 | Mida Rheuma app for patients; DocBoard web-app for doctor | Improvement in QoL and disease activity |
| Ferucci et al. [17] (2022) | Observational | 122 | Telemedicine | Video telemedicine favored. Patients with higher disease activity, those who visited rheumatologist more often in the preceding year used it more |
| Ferucci et al. [18] (2022) | Observational | 122 | Telemedicine | No significant difference in outcome and quality measures between in-person follow-up group and telemedicine |
| Grainger et al. [4] (2017) | Review article | 19 apps (met inclusion criteria) | Mobile applications | Identification of good-quality apps for prospective monitoring of RA, including calculators for rheumatologists and data tracking tools for patients |
| Heiberg et al. [19] (2007) | Observational | 38 | PDA vs. pen-paper | PDA performed like traditional method |
| Foti et al. [20] (2022) | Observational | 171 | Telemedicine with use of PROMs | FM, depression and anxiety was uncovered in RA patients during the pandemic and those who needed in-person consults to address these were identified |
| Yun et al. [21] (2020) | Observational | 6,154 | CAT-PROMIS | RAPID3 and PROMIS-predicted RAPID3 had agreement |
Austin et al. [22] (2020) White et al. [23] (2021) | Proof-of-concept | 9 | Integrated patient generated health data from smartphone into EHRs | Acceptance of real time-RMT by the patient for RA self-management and care |
| McBeth et al. [24] (2022) | Prospective | 254 | Triaxial accelerometer with smartphone app | Assessed sleep variability and hygiene on QoL in RA patients |
| Mollard and Michaud [25] (2021) | Review article | NA | mHealth apps | mHealth apps aid and improve self-management of RA |
| Morales-Ivorra et al. [26] (2022) | Observational | 146 | ThermoDAI | ThermoDAI strongly correlated with USG-synovitis than PtGA |
| Müskens et al. [27] (2021) | Observational | 1,145 | eHealth platform | Better self-management, better disease control despite lesser utilization of healthcare |
| Radin et al. [28] (2022) | Prospective controlled | 20 | TuTOR app to tailor tofacitinib | TuTOR app was preferred by patients for ease of use and immediate response. However, no significant difference between paper dairy use and the app |
| Schougaard et al. [29] (2023) | Cross-sectional | 775 | Electronic questionnaire | Those compliant to remote care had a higher income, fewer comorbid conditions and faith in remote care |
| Seppen et al. [30] (2020) | Systematic scoping review | 10 studies | mHealth (SMS, web apps, mobile apps, pedometers) | mHealth tools led to positive outcome in nearly all studies included |
| Shenoy et al. [31] (2020) | Observational | 723 | Telemedicine | Aided in better disease control, compliance to treatment during the pandemic and switch was feasible and acceptable |
| van der Leeuw et al. [32] (2022) | Proof-of-concept | 279 | Dynamic flare prediction model | May aid in therapeutic decisions of tapering bDMARDs while maintaining continued remission |
| Vodencarevic et al. [33] (2021) | RCT data (from RETRO [34]) used to build a predictive model for flare | 41 | Machine learning models (stacking meta-classifier method) | Development of a clinical prediction tool for flare in patients who have achieved remission |
PROMs: patient-reported outcome measures; VAS: visual analogue scale; COVID-19: coronavirus disease 2019; PDA: personal digital assistant; FM: fibromyalgia; CAT-PROMIS: computer-adaptive testing-Patient Reported Outcomes Measurement Information System; EHR: electronic health record; QoL: quality of life; RAPID3: Routine Assessment of Patient Index Data 3; ThermoDAI: thermographic disease activity index; eHealth: electronic health; USG: ultrasonography; SMS: short message service; PtGA: patient global assessment; bDMARDs: biological disease modifying anti-rheumatic drugs; RETRO: REduction of Therapy in patients with RA in Ongoing remission study [34]; TuTOR: tailoring tofacitinib oral therapy in RA
In the wake of the COVID-19 pandemic, healthcare of chronic diseases was inevitably pushed into telemedicine consultations, which proved to be beneficial in more ways than one. The concept of remote monitoring has been around since the 1960s, when electrocardiograms (EKGs) were being transported over telephone wires. Over the years, these technologies gained popularity, but not since the exponential growth and access to internet did telemedicine and remote health monitoring become as accessible, adoptable, reproducible with adequate patient satisfaction. These systems gained popularity mostly in the field of cardiology initially and have now been expanded into other fields including rheumatology [35–37].
The literature and evidence for the effectiveness of telemedicine saw a recent surge since the COVID-19 pandemic. In 2022, European League Against Rheumatism (EULAR) and Asia Pacific League of Associations for Rheumatology (APLAR) published recommendations for telemedicine and remote care in AIRDs [2, 38]. Even in developed countries, the wait to consult a specialist rheumatologist is often long and painful. Remote care and telemedicine can help bridge this gap to some extent. However, remote care is not a smooth sail and may face hurdles in the form of patient reported barriers like reluctance to adopt new technology, non-uniform access and technological illiteracy, clinical factors like inability to conduct a clinical examination and assess true disease burden, lack of training of healthcare providers in remote care, and logistical and technical issues like data privacy, storage and analysis of big data, etc. [38]. Though initial assessment and pre-diagnostic tests may be done by telemedicine, final diagnosis, and targeted treatment decisions like initiation of disease modifying anti-rheumatic drugs (DMARDs) must be done during an in-person consult only.
The summary of observational studies including retrospective and prospective cohorts, surveys, qualitative studies and reviews related to RMT has been presented above (Table 1), while stronger evidence from RCTs and systematic reviews are presented separately (Table 2).
Randomized control trials (RCT) and systematic review of RCTs
| Authors | Type of study | N (RA patients/apps reviewed) | Monitoring device | Outcome/Remarks |
|---|---|---|---|---|
| Bernard et al. [39] (2022) | RCT | 89 | SATIE-PR app (monitoring interface connected to a smartphone) | Higher QALY, more economical during monitoring |
| El Meidany et al. [40] (2016) | Double-blind RCT | 211 | ePROM | ePROM equivalent to standard PROM, aided in compliance to treatment |
| Doumen et al. [41] (2022) | Meta-analysis | 9,694 | Any app/wearable | All chronic arthritis assessed |
| Li et al. [42] (2023) | Multicenter, pragmatic RCT | 2,197 | Smart system of disease management group (SSDM) app | Digital health app translated to increased disease control rate |
| MacIver et al. [43] (2021) | Systematic review of RCTs | 791 | Tele-health including digital health interventions | Telehealth monitoring translated to improved medication adherence, disease activity, good self-management |
ePROM: electronic PROM; QALY: quality-adjusted life years
There is a good amount of literature to suggest that patients are comfortable and compliant with the usage of various apps and these help with self-management [25]. Optimal requirements for apps have been suggested [4]. The compliance to the shift from clinic based in-person consultations to remote monitoring with apps was well received among patients with RA. Patients found the smartphone apps convenient and they were willing to pay for it and were of the opinion that it would help them be more compliant to treatment [5]. A scoping review including 10 studies have found that RMTs are acceptable and useful [30].
In RA, multiple PROMs have been developed over the years to assess disease activity. These PROMs have been successfully adopted in clinical practice and can be either paper-based or digital, depending on individual patient preference. Patients can also be trained to assess disease activity using PROMs such as the Rheumatoid Arthritis Disease Activity Index (RADAI), RADAI-Five (RADAI5), RAPID3, health assessment questionnaire (HAQ), VAS, Patient-derived Disease Activity Score with 28-joint count (Pt-DAS28), and so on. This can lead to improved monitoring of disease activity and timely therapeutic intervention or modification by the treating physician [44]. The practical utility of these PROMs in RMT has not been validated.
It is an unconscious human nature to overplay inconvenience. It has been found that the correlation between PtGA of the disease and physician global assessment (PGA) of the disease is suboptimal. Patients tend to overestimate pain and functionality more and physicians tend to overestimate the disease based on swollen joints. The Rheumatoid Arthritis in Real Life (REAL) cohort from Brazil showed that there was a discordance between PtGA and PGA in one-third of the patients, with a positive discordance in 80% of them [45]. ePROMs may also tend to overestimate the disease as patient will be the only assessor of clinical disease status and may carry a risk of over-treatment by the physician. Thus, there needs to be validated measures to objectively access patients disease state. Though function capacity and proxies like sleep patterns can be captured via devices monitoring number of steps and polysomnography, these are affected by both disease activity and damage.
Beyond capturing disease activity and functional limitations, RMTs have also been used to assess adherence, responsiveness and tailoring of drug regimens. One such study was the development and validation of an app, tailoring tofacitinib oral therapy in RA (TuTOR) for tailoring tofacitinib and to assess the adherence to the drug [28]. They found that patients preferred using the app for easy interface, improved adherence to therapy, which translated to an overall better control of the disease [28].
The integration of EHRs and RMT can lead to various newer possibilities such as predictive analysis [14]. An EHR-based prediction model fared well to aid tapering of bDMARDs while preventing flares [32]. Such a tie-up between RMT and EHR can lead to real-time predictive analysis to identify and prioritize patient for follow-up visits.
Evidence from RCTs for the effectiveness of remote care and RMTs is limited (Table 2). Two RCTs were identified, which showed that ePROM is non-inferior to in person PROMs [40] and digital health apps have translated to increased disease control [42]. However, there appears to be a dearth of trials comparing RMTs vs. standard of care. Only one RCT has shown that RMTs can be cost-saving and also improve the quality of life of users [39]. A recent systematic review suggested that there are more than 17 mobile applications available for use in patients with rheumatic diseases for remote monitoring and storage of data [4, 46].
While these PROMs may be obtained via telemedicine and tele-counselling, the newer technologies of remote monitoring may not be as affordable and accessible to all patients alike. Access to smartphones and these newer technologies is not uniform and is mostly concentrated among the urban and semi-urban population with a higher per-capita income. The non-uniform access to these techs from rural and lower socioeconomic areas may result in an observation and population bias while assessing disease activity and monitoring follow-up using RMT.
The survey by Schougaard and colleagues [29] have shown that compliance with RMT is associated with higher income and the presence of fewer comorbidities. As the use of RMTs increase, these differences may become more apparent.
There is clear evidence that wearables, mobile-based apps and other internet of things (IoT) components such as smart beds and pill dispensers have good patient acceptance and usability, and this has been demonstrated largely in the setting of RA.
PROMs used in RA mentioned earlier, like RADAI, RADAI5, RAPID3 though beneficial, have shown inconsistent association with physician assessment of disease [45]. As telemedicine and usage of mobile-based apps would rely on the patient’s report and assessment of disease, it may not be prudent to levy the onus of assessment of disease activity on the patient, as beyond active inflammation, there may be other contributors to a higher perceived pain like a mechanical component due to secondary osteoarthritis of the joints or a neuropathic pain or fibromyalgia. This would result in false perception of a higher disease activity. Beyond assessment of disease, usage of RMTs for drug monitoring and titrating treatment has been one of the more intriguing areas of exploration in RA, with evidence available for tofacitinib [28]. The results of this have been encouraging and can be expanded to other drugs in the therapeutic armamentarium.
The main issues that remain are two. First, whether RMTs can improve long term outcomes including quality of life and even mortality has not been demonstrated so far. Second, it is not known whether these solutions are cost-effective. Though some preliminary cost analyses have been done, there are again questions related to the equity of distribution and ease of access. Analyzing only a privileged group may provide biased answer. There is a fear that RMT may be leading to increased cumulative dosage of medication and more healthcare related costs. It is not known if this price actually reduces long term adverse outcomes like erosions, health-related quality of life or cardiovascular events. The gaps in knowledge are summarized in Table 3.
Recommendations for future research
| Category | Goals | Unmet need |
|---|---|---|
| Adherence and acceptability |
| There are some suggestions that adherence to the use of RMT tend to reduce over time. Also, the current literature may be biased to include mostly privileged patients for whom access to smart devices or fast internet is not an issue. |
| Development of tools and standards |
| “Smart” pill dispensers that can tie up with physical activity monitors via an IoT approach. What should be the minimum requirements for RMTs? |
| Integration of new technologies |
| There must be a framework to intergrade and test newer emerging technologies. |
| Validation of existing tools |
| Though several studies have used these tools and have found them useful, there is less information on sensitivity to change or external validation. |
| Proof of benefit |
| Ideally randomized trials are needed to show the superiority of using various grades of technology over usual standard of care. |
Though RMTs are a very promising prospect, they are limited by availability and long-term validation. They may potentially lead to over-treatment and exaggerated costs. Language barriers, non-uniform access to technology, and development of complacency in the patient may be other potentially unwanted effects. However, the data till date is positive and suggests that RMT can be adopted widely as an invaluable tool in the therapeutic armamentarium for RA.
AIRDs: autoimmune rheumatic diseases
bDMARDs: biological disease modifying anti-rheumatic drugs
ePROM: electronic patient-reported outcome measure
EHR: electronic health record
IoT: internet of things
mHealth: mobile health
PDA: personal digital assistant
PROMs: patient-reported outcome measures
PtGA: patient global assessment
RA: rheumatoid arthritis
RADAI: Rheumatoid Arthritis Disease Activity Index
RAPID3: Routine Assessment of Patient Index Data 3
RCTs: randomized controlled trials
REAL: Rheumatoid Arthritis in Real Life
RETRO: REduction of Therapy in patients with rheumatoid arthritis in Ongoing remission
RMTs: remote monitoring technologies
ThermoDAI: thermographic disease activity index
TuTOR: tailoring tofacitinib oral therapy in rheumatoid arthritis
VAS: visual analogue scale
PM: Data curation, Formal analysis, Writing—original draft, Writing—review & editing. SA: Conceptualization, Data curation, Formal analysis, Methodology, Writing—original draft, Writing—review & editing. DD: Conceptualization, Methodology, Supervision, Writing—review & editing.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

Hannah Labinsky ... Johannes Knitza
Michael Schirmer ... Johannes D. Pallua
Diego Benavent ... Antonio Gómez-Centeno
Sumaira Farman ... Saira Elaine Anwer Khan
Carlos A. Guillén-Astete ... Mónica Vázquez-Díaz
Judy L. Seraphine, Alvin F. Wells