Review
Review

Affiliation:
1School of Health Sciences, University of Aveiro, 3810-193 Aveiro, Portugal
2Institute of Biomedicine, University of Aveiro, 3810-193 Aveiro, Portugal
Email: mariolopes77@ua.pt
ORCID: https://orcid.org/0000-0001-9790-2120
Affiliation:
3School of Health Sciences, Polytechnic Institute of Bragança, 5300-121 Bragança, Portugal
ORCID: https://orcid.org/0000-0002-1822-8156
Explor Musculoskeletal Dis. 2026;4:1007117 DOI: https://doi.org/10.37349/emd.2026.1007117
Received: September 29, 2025 Accepted: February 02, 2026 Published: March 13, 2026
Academic Editor: Philippe Gorce, University of Toulon, France
The article belongs to the special issue Prevalence and Risk Factors of Work-related Musculoskeletal Disorders
Work-related musculoskeletal disorders (WMSDs) are a major global occupational health concern, causing substantial pain, disability, and economic burden. They affect muscles, tendons, nerves, joints, and related structures, arising from or being aggravated by workplace factors. This narrative mini-review synthesizes evidence from targeted searches of peer-reviewed occupational health and ergonomics literature, focusing on epidemiological studies, systematic reviews, and recent advances in risk assessment. The review summarizes current knowledge on the prevalence and risk factors of WMSDs across sectors such as healthcare, manufacturing, construction, transport, and office work, where the lower back, neck, shoulders, and upper limbs are most frequently affected. Physical risk factors include repetitive motion, forceful exertion, awkward postures, prolonged static positions, and vibration exposure, while psychosocial factors such as high job demands, low control, inadequate support, and job dissatisfaction further increase risk. Individual characteristics, including age, gender, body mass index, and genetics, also influence susceptibility and highlight the need for tailored prevention, for example, interventions that accommodate women’s double work burden and age-sensitive strategies that help older workers maintain functional capacity. Advances in biomechanical modeling, wearable sensors, and multifactorial risk assessment now allow more precise exposure quantification and earlier detection of WMSD risk. Effective prevention requires multidisciplinary strategies that combine ergonomic workplace redesign, worker training, organizational policies addressing psychosocial risks, health promotion, and early clinical intervention. By consolidating epidemiological evidence, key risk factors, and prevention approaches from an occupational health perspective, this review supports evidence-informed prevention and underscores that coordinated occupational health policies and participatory workplace practices are essential to achieve sustainable reductions in the global burden of WMSDs.
Musculoskeletal disorders (MSDs) related to occupational activities represent one of the most prevalent health problems affecting workers globally and a leading cause of work disability and absenteeism [1]. Characterized by pain and functional impairment in muscles, tendons, ligaments, joints, and nerves, these disorders can develop insidiously or acutely due to repeated or sustained biomechanical stresses encountered in the workplace. The term “work-related musculoskeletal disorders” (WMSDs) differentiates those conditions that are caused or aggravated by occupational factors, highlighting the critical role of work environment, task demands, and organizational factors in aetiology.
The significant socio-economic burden of WMSDs is well documented, with costs stemming from healthcare expenditures, compensation claims, productivity losses, and reduced quality of life for affected workers [2]. Although WMSDs occur across all occupational sectors, prevalence rates vary widely by type of work, exposure levels, and worker demographics. Healthcare professionals, manual labourers, assembly line workers, computerized office workers, and transport operators frequently report high rates of WMSDs [1, 3–6].
Within these high‑risk sectors, WMSD patterns vary substantially across sub‑specialties. Among healthcare workers, for example, nurses and other patient‑handling staff show particularly high rates of low‑back and shoulder disorders linked to repetitive lifting, transferring, and repositioning of patients. In contrast, surgeons are more prone to neck, upper‑back, and lower‑limb complaints associated with prolonged static postures in the operating room and constrained standing positions [6, 7]. In orthopaedical surgery, lower‑limb pain and fatigue related to extended periods of standing and the use of heavy protective equipment have been repeatedly documented, illustrating how task‑specific biomechanical demands shape body‑region‑specific WMSD profiles even within the same sector [8].
Recent decades have witnessed changes in work organization, such as aging workforces, remote and flexible working, technological automation, and evolving employment patterns, that affect the nature and distribution of WMSD risk factors [9]. This highlights the need for a comprehensive understanding of prevalence patterns and a multifactorial view of risk that encompasses physical, psychosocial, individual, and organizational dimensions [4].
Therefore, this narrative review aims to provide an up-to-date synthesis of evidence on the prevalence and risk factors of WMSDs, incorporating studies from multiple industries and occupations. It discusses emerging trends in risk assessment and interventions, emphasizing a multidisciplinary approach to prevention and management in diverse work environments.
This narrative mini‑review was conducted to synthesize recent evidence on the prevalence and risk factors of WMSDs across diverse occupational sectors. Targeted literature searches were performed in PubMed, Scopus, and Web of Science, complemented by manual screening of the reference lists of key articles.
The search strategy combined terms related to MSDs and work, including variants of “work‑related musculoskeletal disorders,” “occupational musculoskeletal disorders,” “work‑related pain,” “ergonomic risk factors,” and “psychosocial risk factors,” using Boolean operators (AND, OR) to link concepts. Searches were limited to articles published in peer‑reviewed journals between 2000 and 2025 and written in English, to capture vast existing evidence reflecting work organization and technologies.
Studies were eligible for inclusion if they: (1) involved an adult working population; (2) reported prevalence, incidence, or burden of WMSDs and/or examined associations with physical, psychosocial, or individual risk factors; and (3) used observational, interventional, or review designs (cross‑sectional, cohort, case‑control, randomized or non‑randomized interventions, or systematic reviews/meta‑analyses). Exclusion criteria were: (1) studies focusing exclusively on non‑occupational musculoskeletal conditions; (2) case reports, conference abstracts, editorials, or commentaries without primary data; and (3) articles not available in full text.
After removing duplicates, titles and abstracts were screened for relevance, followed by a full‑text assessment for eligibility. Given the narrative nature of this review, a formal risk‑of‑bias assessment was not undertaken; instead, emphasis was placed on recent, large, or methodologically robust studies and high‑quality systematic reviews in occupational health and ergonomics. In total, 64 studies meeting the inclusion criteria were included in the synthesis, with findings organized around prevalence patterns by sector and body region, key physical and psychosocial risk factors, and emerging approaches to risk assessment and prevention.
WMSDs represent a significant proportion of occupational illnesses worldwide. The International Labour Organization estimates that MSDs constitute between 30% to 45% of all occupational diseases across countries. Prevalence varies by body region, occupation, and country-specific factors [10].
Lower back pain is typically the most prevalent WMSD complaint, reported in up to 60% of workers in physically demanding jobs and 20–40% in sedentary roles [11]. Neck and shoulder disorders also impose a considerable burden, especially in occupations that require sustained arm elevation or static postures, such as healthcare and office work [2, 3]. Upper limb disorders, including carpal tunnel syndrome and tendonitis, are frequent among assembly line workers and data-entry professionals [12]. Lower limb disorders are comparatively less studied but recognized in occupations involving prolonged standing or heavy lifting [8].
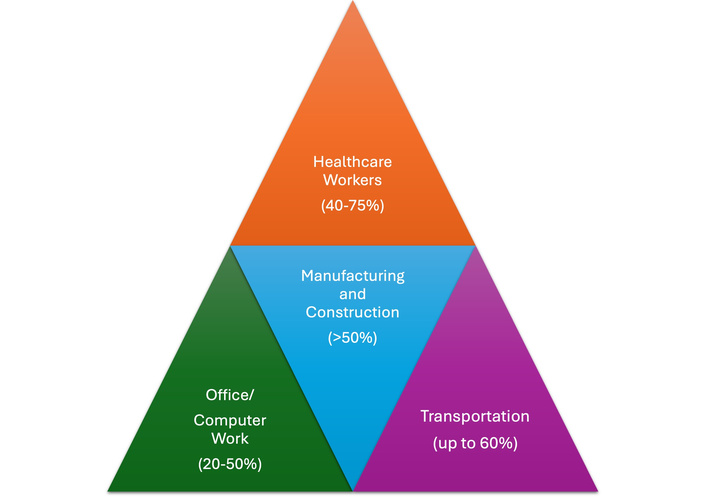
Healthcare workers: High prevalence of WMSDs, especially lower back and shoulder pain, due to patient handling and repetitive movements. Prevalence estimates range from 40% to 75% (Figure 1) depending on the study and country [2]. Intense physical demands lead to prevalence rates exceeding 50%, often associated with repetitive lifting, vibration exposure, and awkward joint postures [13–15]. Among healthcare professionals, WMSDs consistently rank among the highest-prevalence figures reported across occupations, with umbrella and meta-analytic evidence indicating overall 12‑month rates frequently between 60% and 85%, and even above 80% in some nursing groups. Nurses are among the most extensively studied, with systematic reviews and continental meta-analyses showing very high prevalence in European and Asian hospital settings, and particularly elevated rates of low back, neck, and shoulder symptoms, typically exceeding 50–60% for the lumbar region and around 45–55% for the neck [6, 16–20]. Body‑region‑specific syntheses for perioperative and theatre nurses confirm that the lower back, shoulder/upper back, waist, and knee are the most frequently affected sites, and highlight the contribution of prolonged static standing, awkward trunk flexion/rotation, and patient handling in constrained environments [19]. Similar patterns have been documented in other healthcare professions: dental meta‑analyses report pooled MSD prevalence close to 78%, with particularly high involvement of the neck, back, and shoulders [21, 22], while a large surgeon‑focused meta‑analysis identified the neck, back, lower back, and shoulders as the body areas with the highest worldwide WMSD prevalence, regardless of specialty [8, 23, 24]. Recent umbrella reviews integrating dentists, nurses, surgeons, and mixed healthcare samples across continents confirm that the lower back is the most exposed region (prevalence around 55–57%), followed by the neck and shoulder, and suggest that these high burdens are remarkably consistent despite geographical and organizational differences [2, 8, 21–25].
Office/Computer work: Increasingly documented WMSDs such as neck and upper extremity disorders linked to static postures and repetitive keyboard/mouse use, reported in 20–50% of workers [26].
Transportation: Prolonged sitting, whole-body vibration, and static postures are associated with high rates of lower back and neck disorders, with up to 60% prevalence [27].
Studies indicate wide variation in WMSD prevalence internationally, influenced by differences in work practices, reporting systems, and labour regulation. Developing countries may report fewer cases due to underdiagnosis, but often have high actual prevalence due to poor ergonomic standards [13, 14, 28].
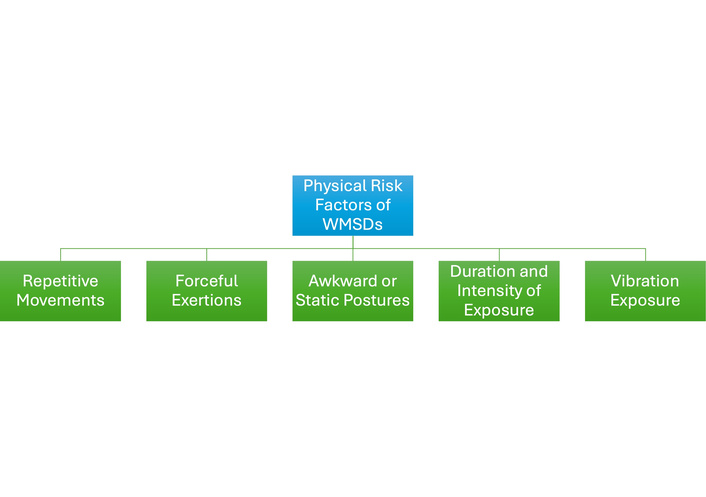
The pathophysiology of WMSDs is complex, involving biomechanical overload, microtrauma, inflammation, and neural sensitization. Physical risk factors (Figure 2) play a cardinal role [29]. Across healthcare settings, physical risk factors for WMSDs are dominated by high biomechanical loads, particularly heavy manual handling, awkward trunk postures, and repetitive upper-limb tasks [30]. Long periods of static standing or constrained postures, such as sustained trunk flexion or rotation during patient handling, surgery, and dental work, substantially increase spinal compression and are strongly associated with low-back and neck pain among healthcare workers [30–32]. Repetitive fine-motor activities and forceful gripping, for example, during manual therapy, instrument manipulation, or precision surgical tasks, are consistently linked with wrist/hand and thumb disorders in physiotherapists, surgeons, and dentists [31, 33]. High patient loads, frequent transfers or mobilizations, and limited recovery time amplify these biomechanical exposures, with treating an excessive number of patients in one day and repeatedly working near physical limits identified as key predictors of WMSDs in hospital staff [30]. Systematic reviews of healthcare professionals more broadly converge on the conclusion that combinations of heavy physical work, excessive repetition, awkward postures, and insufficient rest breaks represent the core physical determinants of WMSDs, particularly in the lower back, neck, shoulders, and upper extremities [31, 32].
Repetitive movements: Prolonged repetition of similar tasks without adequate recovery contributes to tissue microdamage, with dose-response relationships documented between repetition rate and risk for upper extremity disorders [12, 34, 35].
Forceful exertions: Tasks requiring high force, such as heavy lifting or grip strength, elevate WMSD risk, especially when combined with awkward postures [36].
Awkward or static postures: Non-neutral joint positions increase musculoskeletal strain. For example, sustained neck flexion is linked to cervical disorders, while trunk bending and twisting correlate with low back pain [37, 38].
Duration and intensity of exposure: Longer exposure to physical risk factors increases risk, with cumulative effects over time [12, 36].
Vibration exposure: Whole-body vibration in drivers and hand-arm vibration in tool operators are associated with WMSDs affecting the spine and upper limbs, respectively [39, 40].
Beyond biomechanical loading, psychosocial and organizational factors have a profound and well-documented impact on both the risk and outcomes of WMSDs. Modern research demonstrates that physical exposures do not simply determine the onset and chronicity of these conditions; they are also modulated by the psychosocial context of the workplace, which in turn modulates both worker behaviours and physiological responses [41, 42].
Job demands and control: High job demands, such as tight deadlines, excessive workload, and persistent time pressure, combined with low decision latitude or minimal influence over one’s work, are strongly associated with an increased risk of musculoskeletal symptoms [43]. The mismatch between demands and control may heighten stress, leading to increased muscle tension, altered movement patterns, and reduced recovery time, which ultimately contribute to the development and exacerbation of WMSDs [44]. Environments where workers perceive little participation in decision-making or lack autonomy show consistently higher rates of multiple-site musculoskeletal pain and long-term sickness absence [45].
Social support: Low levels of social support from supervisors and colleagues are associated with a higher rate of WMSDs [46]. Poor interpersonal relationships at work can intensify stress, decrease coping abilities, and reduce adherence to recommended rest or safety measures [7]. In contrast, supportive leadership and positive workplace relationships provide a buffer that can mitigate stress and reduce musculoskeletal complaints, highlighting the importance of a collaborative environment [46].
Job satisfaction and reward: Workers with low job satisfaction, perceived role monotony, or inequitable reward structures are more prone to musculoskeletal complaints [47]. When high effort is not matched with adequate recognition or reward, known as effort-reward imbalance, psychosocial strain rises, and the risk of pain and disability is augmented [48]. Such environments also foster negative affect and diminish engagement in health-promoting behaviors [47].
Work pace and rest breaks: Fast work pace, unpredictable workload surges, and insufficient rest breaks reduce opportunities for muscle recovery and exacerbate tissue overload [49, 50]. A stressful pace and skipped breaks can encourage unsafe behaviors, such as carrying heavier loads, rushing, or neglecting ergonomic precautions, all of which magnify WMSD risk [50, 51].
Workplace organization: Organizational structures that include shift work, temporary contracts, job insecurity, or a lack of participation in workplace decision-making further amplify risks of WMSDs [52]. The instability and unpredictability in such environments may increase perceived stress and reduce workers’ opportunities to access preventative resources or report symptoms early [52].
Emerging models emphasize the multifactorial nature of these interactions: psychosocial stressors may directly affect the musculoskeletal system via physiological pathways, such as prolonged muscle tension, altered blood flow, and impaired tissue repair, or indirectly by influencing behaviors that increase biomechanical load and risk exposure. Addressing these factors requires both organizational commitment to improved psychosocial working conditions and systematic risk assessment that goes beyond physical exposures alone [53].
Individual susceptibility to WMSDs is shaped by a multifaceted interplay of demographic, biological, genetic, and lifestyle-related variables [36] (Figure 3). These factors not only influence risk but also affect the onset, progression, and severity of symptoms across diverse occupational groups [54].
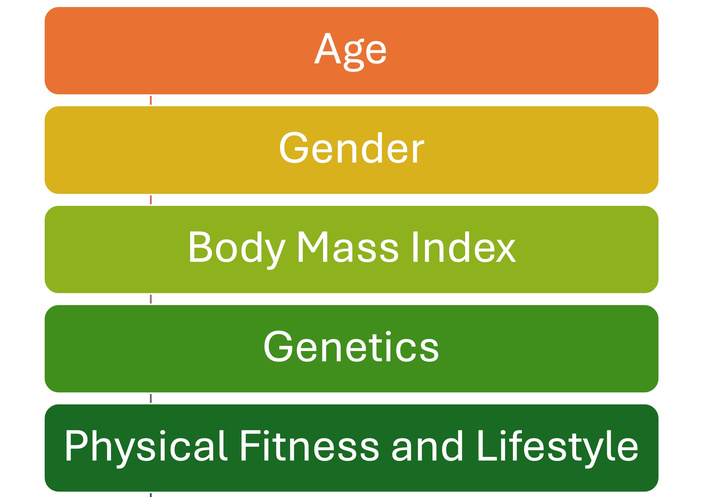
Individual and demographic factors in work-related musculoskeletal disorders (WMSDs).
Age: The incidence and severity of WMSDs increase with age, primarily due to natural biological changes such as reduced tissue elasticity, decreased muscle mass and strength, diminished proprioception, and slower tissue regeneration and repair capacity [55]. Age-related osteoarthritis, sarcopenia, and cumulative exposure to occupational risk factors over time contribute to heightened vulnerability in older workers [56]. As a result, even similar physical exposures may result in more severe or persistent symptoms in aging populations, underscoring the need for prevention strategies tailored to the aging workforce [55].
Gender: A wealth of epidemiological evidence demonstrates that female workers tend to report a higher prevalence of WMSDs than their male counterparts, even when exposed to comparable occupational hazards [57, 58]. This disparity may be attributed to a confluence of factors:
Anatomical and physiological differences, such as lower average muscle mass and joint size, hormonal variations, and pregnancy-induced changes, can influence injury risk and pain perception.
Task allocation in the workplace may disproportionately expose women to repetitive, fine-motor, or static postural work, while domestic roles add cumulative biomechanical loads.
Footwear choices also contribute to gendered patterns of WMSDs, as many women are expected to wear high‑heeled shoes in professional settings. Regular high‑heel use has been associated with increased forefoot loading, altered gait and spinal alignment, hallux valgus, and a higher prevalence of musculoskeletal pain and injury in the feet, lower limbs, and lower back among working women.
Psychosocial stressors, double work burden (“double presence”), workplace design not optimized for female anthropometry, and social inequalities further compound risk.
Despite these factors, studies also show that men have a higher risk of certain WMSDs (e.g., low back pain from heavy lifting), highlighting the role of differential exposure and task assignment [59, 60].
Body mass index (BMI): Obesity and overweight status increase mechanical stress on the musculoskeletal system, particularly in weight-bearing joints like the spine, hips, and knees, thereby elevating WMSD risk. Excess adipose tissue may contribute to systemic inflammation, impeding tissue recovery and increasing pain sensitivity. Excess adipose tissue releases chemical mediators that promote a persistent, low‑grade inflammatory state throughout the body. This chronic inflammation can elevate pain sensitivity and accelerate wear of joints and soft tissues, helping to explain the greater burden of work‑related musculoskeletal problems in workers with obesity. Furthermore, body type is generally considered a contributing rather than a deterministic risk factor for WMSDs, because its impact depends on the interaction with specific job demands and ergonomic conditions. For example, individuals with higher BMI or extreme body dimensions (very short or very tall stature) may experience greater joint loading, awkward reach distances, or equipment-fit mismatches during manual handling or repetitive tasks, which can increase musculoskeletal strain when workstations are not adequately adapted [61, 62].
Genetics: Recent research identifies genetic predisposition as a modulator of WMSD risk. Variants in genes involved in collagen synthesis, inflammation control, and pain modulation may alter susceptibility, with certain individuals being more prone to developing WMSDs even at lower levels of exposure [63, 64].
Physical fitness and lifestyle: Low levels of physical conditioning reduce musculoskeletal resilience, making tissues more susceptible to overload and injury. Sedentary lifestyle, smoking, inadequate nutrition, and high levels of psychosocial stress outside work all further heighten the likelihood of WMSDs [65]. Positive health behaviors, including regular exercise, maintenance of a healthy weight, and stress management, are protective and should be promoted as part of comprehensive prevention strategies [65].
By recognizing and addressing these individual and demographic differences, employers and occupational health professionals can more effectively develop targeted interventions to reduce WMSD risk and foster equal health and safety outcomes across the workforce [66].
The evolution of technology and methodological approaches continues to transform the understanding and management of WMSD-related risk [67]. Recent years have seen the introduction of sophisticated tools that enable more precise, real-time, and comprehensive assessment of biomechanical and psychosocial exposures in the workplace [68].
Biomechanical modeling: Advanced computer simulations now allow detailed estimation of joint loads, muscle forces, and postural stresses under varying work conditions. Motion capture data and musculoskeletal modeling frameworks predict high-risk postures and movements that contribute to WMSDs. This dynamic modeling informs ergonomic redesigns by identifying task modifications or assistive interventions that minimize harmful mechanical stress, optimizing worker safety and performance [69].
Wearable sensors: The widespread adoption of wearable technologies, such as inertial measurement units (IMUs), accelerometers, electromyography (EMG) sensors, pressure insoles, and textile-based strain sensors, has revolutionized exposure quantification. These devices capture objective, continuous data on posture, motion patterns, muscle activity, and force exertion in real-time during actual work tasks. Such granular monitoring enables personalized risk profiles, supports early symptom detection, and provides feedback for immediate corrective action [70]. Emerging soft wearable sensors embedded in clothing and gloves offer enhanced comfort and user acceptance while maintaining data fidelity. Despite challenges such as sensor placement, data processing, and ergonomics, ongoing miniaturization and integration with personal protective equipment hold promise for broader workplace applications [71].
Psychosocial surveys: Quantitative assessment of workplace psychosocial factors has been standardized through the use of validated questionnaires and scales that measure workload, stress, job control, social support, and reward. These tools identify workers at psychosocial risk and enable the examination of interactions between psychosocial stressors and biomechanical exposures [72]. Integration of psychosocial data enriches risk models beyond physical factors alone, capturing multidimensional contributors to WMSDs [73].
Multifactorial risk models: Current paradigms emphasize integrating physical, psychosocial, and individual factors into comprehensive risk assessment models. Statistical and machine learning approaches analyze complex datasets from wearable sensors, ergonomic observations, and psychosocial surveys to identify critical predictors and stratify risk levels across worker populations. Such integrative frameworks facilitate targeted preventive strategies, improving resource allocation and intervention effectiveness [74].
Overall, the integration of innovative technologies with comprehensive ergonomic and psychosocial assessment tools is shaping a new era in WMSD risk management. Continuous advancement in sensor technology, data analytics, and ergonomic modeling promises enhanced workplace safety through proactive, individualized risk detection and intervention.
Effective management of WMSDs demands a multidisciplinary and multilevel approach that tackles both the physical and psychosocial aspects of the workplace [75]. Prevention must be proactive, comprehensive, and participatory, engaging employers, workers, and health professionals collaboratively to sustain worker health and productivity [75].
Ergonomic interventions: The foundation of WMSD prevention lies in systematic ergonomic assessments followed by targeted workplace redesign. Ergonomic interventions aim to optimize workstations, tools, and task designs to promote natural postures, reduce repetitive motions, and minimize manual handling of heavy loads. Adjustable desks, mechanical aids, and ergonomic tools such as anti-fatigue mats or supportive seating are examples of practical solutions. These redesigns not only reduce physical stress but also improve comfort and efficiency. The implementation must be guided by expert evaluation and tailored to specific work environments for maximal effectiveness [76].
Training and education: Comprehensive worker training programs play an essential role in raising awareness of musculoskeletal risks and fostering safe work behaviors. Training includes correct lifting techniques, posture awareness, stretching exercises, and early symptom recognition. Evidence suggests that education significantly reduces injury prevalence and promotes long-term adherence to ergonomic principles, especially when combined with workplace modifications [77]. Training content should also be adapted to individual worker profiles. For example, education programmes for female workers engaged in patient handling or repetitive upper‑limb tasks can emphasise team‑based handling techniques, optimal use of mechanical aids, and strategies to manage combined occupational and domestic physical loads. In contrast, age‑adapted training for older workers should prioritise joint‑friendly movement patterns, pacing strategies, and exercises to preserve strength, balance, and flexibility.
Organizational policies: Addressing the psychosocial work environment through job redesign, such as increasing job control, improving task variety, scheduling adequate rest breaks, and fostering social support, has been shown to reduce the incidence of WMSD. Policies promoting a healthy workplace culture and participation in ergonomic decision-making enhance employee engagement and wellbeing, further mitigating risk [42, 78].
Health promotion: Encouraging physical fitness, weight management, and smoking cessation complements ergonomic and organizational interventions. Healthy lifestyle choices enhance musculoskeletal resilience and overall recovery potential. Workplace wellness programs integrating exercise, nutrition counseling, and stress management have demonstrated reductions in musculoskeletal pain and improved worker satisfaction [79, 80].
Technological innovation: Recent advances introduced exoskeletons, robotics, and wearable assistive devices designed to reduce physical loads and fatigue, particularly in high-risk sectors such as manufacturing, healthcare, and logistics. These technologies offer real-time feedback and mechanical support, enabling workers to perform tasks with decreased biomechanical stress. Ongoing research supports their potential but also notes the need for ergonomic integration and employee training to maximize benefits [81, 82].
Early intervention: Prompt access to clinical and occupational health services is critical to prevent acute musculoskeletal symptoms from progressing to chronic conditions and disability. Early diagnosis, individualized treatment plans, and workplace accommodations facilitate quicker recovery and reduce absence from work. Regular health surveillance and self-reporting tools help detect emerging issues before they escalate [83, 84].
Collectively, WMSD prevention and management require continuous collaboration across disciplines, embracing ergonomic science, organizational change, health education, and technological innovation. Integration of these elements fosters safer, healthier workplaces and supports the long-term well-being and productivity of workers.
This narrative mini‑review integrates evidence from epidemiological studies, systematic reviews, and recent advances in biomechanical and technological risk assessment to provide a comprehensive, multidisciplinary overview of WMSDs. The focus on multiple sectors, including healthcare, manufacturing, construction, transport, and office work, highlights common and sector‑specific risk factors, supporting the transferability of findings across diverse work environments. By combining physical, psychosocial, and individual determinants of WMSDs with discussion of emerging prevention strategies, the review offers a concise, practice‑oriented synthesis that can inform occupational health policies, workplace interventions, and future research priorities.
Several limitations should be considered when interpreting the findings of this narrative mini review, particularly from an occupational health and ergonomics perspective. First, the narrative design does not follow the structured methodology of a systematic review, and therefore lacks a predefined protocol, formal risk-of-bias assessment, and quantitative synthesis. While the included literature was selected based on relevance to occupational exposure, scientific quality, and contribution to the field, the possibility of selection bias and limited reproducibility cannot be excluded.
Second, the reviewed studies exhibit substantial heterogeneity in the definition, classification, and measurement of WMSDs. Variations in diagnostic criteria, symptom recall periods, body-region specificity, and outcome measures reduce comparability across studies and limit the strength of aggregated conclusions. The frequent reliance on self-reported symptoms, a common feature in occupational health research, introduces potential recall and reporting bias and may not accurately reflect clinically verified conditions or cumulative exposure.
Third, exposure assessment remains a key methodological limitation across the literature. Many studies rely on proxy measures of physical workload, such as job titles, task descriptions, or self-reported exposure, rather than objective or direct measures. Although recent advances in wearable sensors, biomechanical modeling, and digital exposure monitoring are promising, their application remains inconsistent, and validation across different occupational settings is still limited. Consequently, exposure misclassification cannot be ruled out.
Fourth, the predominance of cross-sectional study designs restricts causal inference between occupational exposures and WMSDs. While associations with physical, psychosocial, and organizational risk factors are well documented, longitudinal and prospective evidence remains insufficient in several sectors, particularly in emerging work arrangements such as remote, platform-based, or hybrid work. This limitation is especially relevant when interpreting findings for preventive policy and intervention planning.
Fifth, although this review addresses prevention strategies and risk assessment frameworks, the effectiveness of many ergonomic and organizational interventions remains context-dependent. Differences in implementation fidelity, workforce characteristics, regulatory environments, and organizational culture limit the transferability of intervention outcomes across industries and countries.
Finally, despite attempts to include studies from diverse geographical regions, the evidence base remains skewed toward high-income countries with established occupational health surveillance systems. Evidence from low- and middle-income countries, informal work sectors, and small enterprises is comparatively underrepresented, limiting global generalizability and policy relevance in these contexts.
Future research in occupational health would benefit from harmonized case definitions, improved exposure assessment methods, and greater use of longitudinal designs. In addition, intervention studies with robust implementation and process evaluations are needed to support evidence-informed prevention strategies and occupational health policy development.
This narrative mini‑review synthesizes contemporary evidence on the prevalence and multifactorial risk factors of WMSDs across diverse occupational sectors. It highlights the combined contribution of physical, psychosocial, and individual determinants, as well as emerging biomechanical and technological tools that enhance exposure assessment and early detection. The review also draws attention to high‑risk worker groups and body regions, emphasizing how sector‑specific task demands shape WMSD patterns and burden. By integrating findings from epidemiological studies and systematic reviews, it offers an accessible summary that can support evidence‑informed decision‑making in occupational health practice and policy. The evidence highlights the need for integrated, multidisciplinary prevention strategies that align ergonomic redesign, worker training, psychosocial risk management, and early clinical intervention. Translating this knowledge into coordinated occupational health policies and participatory workplace practices is crucial to sustainably reduce the burden of WMSDs and protect workers’ health and productivity worldwide.
BMI: body mass index
MSDs: musculoskeletal disorders
WMSDs: work-related musculoskeletal disorders
M Lopes: Conceptualization, Investigation, Writing—original draft, Writing—review & editing, Supervision. M Lages: Investigation, Writing—original draft, Writing—review & editing. Both authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Antonina D.S. Pavilanis ... Michael J.L. Sullivan
Philippe Gorce, Julien Jacquier-Bret
Raquel Ferreira Araruna de Carvalho, Márcio Alves Marçal
Philippe Gorce, Julien Jacquier-Bret
Youssef Habib ... Peter J. Keir
João Alberto de Souza Ribeiro, Luciana Aparecida Giacomini
Adrian Low, Benny Lam
Annalisa Bertoli ... Cesare Fantuzzi