Perspective
Perspective

Affiliation:
1Department of Medicine and Surgery, University of Enna “Kore”, 94100 Enna, Italy
2Department of Dental Research Cell, Dr. D. Y. Patil Dental College and Hospital, Dr. D. Y. Patil Vidyapeeth (Deemed to be University), Pimpri, Pune 411018, Maharashtra, India
Email: luca.fiorillo@unikore.it
ORCID: https://orcid.org/0000-0003-0335-4165
Explor BioMat-X. 2026;3:101359 DOI: https://doi.org/10.37349/ebmx.2026.101359
Received: July 09, 2025 Accepted: February 08, 2026 Published: February 11, 2026
Academic Editor: Kedong Song, Dalian University of Technology, China
The article belongs to the special issue Innovations in Biomaterials for Dentistry and Oral Surgery
The emergence of stem-cell-derived enamel organoids and dentin-producing dental pulp stem cell constructs presents new possibilities for restoring carious lesions using autologous enamel–dentin inlays. This overview outlines the biological and technological advances supporting this approach and proposes a workflow oriented toward clinical application. The benefits of tissue-based inlays, including inherent biomechanical compatibility, aesthetic accuracy, and potential for biological integration, are contrasted with those of purely artificial materials. Significant regenerative developments include the formation of human enamel organoids and odontoblast-lineage cells in vitro, 3D bioprinting of tooth-shaped constructs with demineralised dentin matrix and poly(ε‑caprolactone) scaffolds, and fibre-guiding periodontal ligament scaffolds that restore Sharpey’s fibres in vivo. The mechanical performance of adhesive resin cements, with bond strengths of approximately 4–7 MPa to enamel and dentin, and their durability in reattaching natural tooth fragments, supports the feasibility of bonding biological inlays. Practical considerations include controlling the slow degradation and hydrophobicity of poly(ε-caprolactone) through the use of ceramic or natural polymer additives, employing multi-material 3D printing to co-print mineralized enamel and cell-laden dentin layers, and achieving the desired shade, microstructure, and mechanical properties, exemplified by a compressive strength of approximately 677 MPa for 3D-printed zirconia crowns. Despite regulatory and translational challenges, the integration of digital dentistry, bioprinting, and stem cell science points toward future “grow and glue” restorations that may replace traditional drill-and-fill methods.
Dental caries are conventionally managed by drilling out decayed tissue and filling the cavity with artificial materials (composites, ceramics, or amalgam). These materials restore form and function but cannot truly replicate the complex biology of natural tooth structure. Critically, human teeth have almost no intrinsic regenerative capacity once formed, enamel is acellular and cannot self-repair, and dentin can only regenerate in a limited fashion via pulp cells (often insufficient in deep lesions) [1–3]. This leads to a paradigm in which restorations, while improving, remain replacements rather than true regeneration of tooth substance. Emerging advances in tissue engineering and 3D bioprinting suggest that biological restoration of lost tooth structure may eventually be feasible. Recent studies have induced human stem cells to form enamel-producing ameloblasts and dentin-forming odontoblasts, and even generated small enamel organoids that secrete enamel matrix and mineralize it. Likewise, whole tooth buds have been bioengineered in animal models to develop teeth with enamel, dentin, and pulp. These breakthroughs lay the groundwork for a future in which a dentist could replace a carious lesion with an anatomically precise inlay made of real enamel and dentin. This perspective article outlines a forward-looking clinical protocol for treating caries using bioprinted or tissue-grown enamel–dentin inlays that are bonded into the tooth using today’s adhesive techniques.
This manuscript discusses the current status of enamel and dentin regeneration, 3D bioprinting of dental tissues (including brief comparisons with soft-tissue and bone bioprinting), existing adhesive cementation techniques for tooth structures, and the challenges that must be addressed to translate this vision into practical applications [4]. Drawing on recent research and concepts highlighted in popular science media, this work aims to present a scientifically rigorous yet innovative roadmap for developing “living” dental fillings that restore teeth to their proper form and function.
Enamel is the hardest tissue in the human body, composed of highly organized hydroxyapatite crystallites, and is formed only during tooth development by ameloblast cells. After tooth eruption, all ameloblasts undergo apoptosis, leaving no cells to regenerate enamel if it is lost. Dentin, the bone-like substance beneath the enamel, is produced by odontoblasts at the pulp interface and can be deposited slowly in response to injury (tertiary dentin). However, this process is often limited and insufficient for addressing significant carious defects. Given these biological limits, researchers have long sought tissue engineering strategies to regenerate these hard tissues. Early approaches explored whole-tooth regeneration: For example, Nakao et al. [5] in Japan combined dental epithelial and mesenchymal stem cells to bioengineer a tooth germ that, when implanted in mice, developed a tooth with organized enamel and dentin layers. Subsequent experiments demonstrated that such lab-grown tooth buds could be transplanted into the jaw and integrate with the alveolar bone, effectively replacing a missing tooth with a biologically formed tooth unit. While whole-tooth engineering is remarkable, replacing an entire tooth is an extreme approach to caries treatment, whereas most of the natural tooth can be preserved. A more targeted approach is partial regeneration of lost enamel or dentin [6].
Recent breakthroughs in stem cell biology have opened the door to regenerating enamel, a tissue previously considered irreparable. In 2023, Alghadeer et al. [7] reported the creation of human ameloblast-like cells from induced pluripotent stem cells, identifying key gene pathways that drive ameloblast differentiation. When co-cultured with mesenchymal pulp-like cells, these cells self-organized into dental organoids, miniature tooth-like structures, that secreted the major enamel proteins (amelogenin, ameloblastin, enamelin) and mineralized them into an enamel-like extracellular matrix. This landmark demonstrated that functional enamel-forming tissue can be generated in vitro. Although the enamel produced was rudimentary, it exhibited the elemental composition and structural features of natural enamel. Parallel advances have demonstrated the generation of odontoblast-lineage cells from dental pulp stem cells (DPSCs) or other sources, which are capable of depositing dentin matrix proteins. Together, these findings suggest that it is conceivable to bioengineer a small volume of enamel and dentin, precisely what would be needed for an inlay-type restoration. Notably, these efforts are still in the early experimental stages (enamel organoids measuring only millimeters). Still, they provide proof of concept that the building blocks of tooth hard tissues can be grown on demand [8].
Other strategies for enamel/dentin regeneration have focused on biomaterial-mediated mineralization. For instance, biomimetic peptides and matrices can induce remineralization of incipient lesions (the regrowth of mineral in demineralized enamel). However, these data methods only fill in microscopic defects and do not reconstruct anatomy. A recent laser-assisted technique has been reported to rapidly mineralize a synthetic enamel-like layer onto teeth, suggesting potential in situ regeneration approaches. However, to restore a large cavity with proper tooth anatomy, a more cell-guided process is likely needed to lay down the highly ordered enamel rods and dentinal tubules in their proper arrangement. Table 1 summarizes key milestones in enamel and dentin tissue engineering relevant to this vision, from organoid and whole-tooth studies to biomaterial approaches and clinical demonstrations of bonding natural tooth fragments [9, 10].
Key studies and technologies underpinning enamel and dentin regeneration for inlay therapy
| Study/Technology (Year) | Approach | Tissues targeted | Key findings/Significance |
|---|---|---|---|
| Nakao, 2007 [5] | Cell-based organ engineering | Enamel, dentin, pulp (whole tooth) | Combined epithelial + mesenchymal stem cells to form a tooth germ in vitro; upon implantation in mice, it grew a structurally correct tooth with enamel and dentin. Pioneering demonstration of whole-tooth regeneration. |
| Oshima, 2011 [6] | Organ germ method, transplantation | Whole tooth unit + bone | Grew a tooth bud in vitro then transplanted into a mouse jaw defect; the bioengineered tooth achieved bone integration and functional attachment. Proved that engineered tooth units can integrate into the oral environment. |
| Pandya, 2019 [4] | Review of strategies (physicochemical, biomimetic, cellular) | Enamel (and tooth tissues) | Outlined five pathways for enamel regeneration: (i) synthetic crystal growth, (ii) protein-guided mineralization, (iii) surface remineralization (e.g., peptides), (iv) cell-based engineering (hampered by lack of immortal ameloblast lines), (v) whole-tooth biological development. Emphasized the need for ameloblast sources and the challenges in recapitulating enamel’s structure. |
| Alghadeer, 2023 [7] | Stem cell differentiation and organoid formation | Enamel (with dentin precursors) | Differentiated human iPSCs into ameloblast-like cells and neural crest-like cells; formed enamel organoids secreting amelogenin, ameloblastin, enamelin and producing mineralized enamel matrix. Also identified odontoblast precursor cells. First successful creation of human enamel-forming organoids—milestone for enamel regeneration. |
| Han, 2021 [10] | Hybrid bioprinting (cell-laden hydrogel + polymer) | Dentin/Pulp (tooth structure) | Used a bio-ink with demineralized dentin matrix particles and DPSCs, printed in shape of a human molar with supportive PCL frame. After 15 days in odontogenic culture, the construct showed calcified deposits and upregulation of dentin markers (DSPP, DMP-1). Demonstrated feasibility of printing a living tooth scaffold and partial dentin regeneration in vitro. |
| Zhao, 2024 [1] | Schematic & review (Frontiers in Bioeng Biotech) | Multi-tissue (enamel, dentin, PDL, bone) | Described a digital process for dental tissue bioprinting: CT/scan to get 3D model, CAD design of scaffold including macro- and micro-structure, selection of suitable biomaterials and cells, then printing via extrusion, inkjet or laser methods. Highlighted current 3D printing applications in pulp, dentin, ligament, bone regeneration. Serves as a blueprint for integrating bioprinting with clinical workflows. |
| Sargod, 2010 [14] | Clinical case (9-year follow-up) | Enamel and dentin (natural fragment) | Reported a coronal tooth fracture repaired by bonding the original fragment with resin. After 9 years, the reattached fragment remained esthetic and functional. Illustrates that adhesive bonding to natural enamel/dentin is durable, supporting the concept that a natural tissue inlay can be securely cemented with existing adhesives. |
| Jablonski-Momeni, 2014 [9] | Self-assembling peptide applied clinically | Enamel (early caries lesions) | Although not a restoration, P11-4 peptide technology (Curodont™) induces mineralization in small enamel lesions, achieving lesion regression by regrowing hydroxyapatite in situ. Shows a current biomimetic tool for enamel repair in early-stage caries, foreshadowing more extensive regenerative treatments. |
3D bioprinting is a technology that precisely deposits living cells and biomaterials layer by layer to create tissue constructs with predetermined architectures. In the context of dental tissues, bioprinting offers the intriguing ability to fabricate a replacement tooth structure that matches a patient’s defect exactly in shape and potentially in composition [11]. High-resolution bioprinters can theoretically position different cell types or materials in distinct regions, for example, a more rigid, enamel-like material on the outside and a more resilient, dentin-like material beneath. Indeed, researchers have begun printing tooth-mimetic structures: Han et al. [10] developed a hybrid bioprinting approach using a bio-ink laden with DPSCs and a supporting polymer frame to fabricate a tooth-shaped construct. After culturing in odontogenic media, the printed tissue showed markers of dentin formation (e.g., dentin sialophosphoprotein expression and mineral deposition), indicating that the printed DPSCs were maturing into odontoblast-like cells within the construct. This study, while preliminary, demonstrated the feasibility of creating a cellular 3D-printed tooth portion in the lab. Other groups have bioprinted simpler tooth components; for example, collagen hydrogel scaffolds with embedded cells have been printed to regenerate dental pulp-like tissue and vasculature, and periodontal ligament scaffolds have been printed with precise fiber alignments to support tooth attachments. Advancements in printing soft and hard dental tissues highlight the “architectural control” offered by bioprinting, an essential feature for fabricating complex structures like enamel and dentin.
Moreover, 3D bioprinting has already established a foothold in related areas of medicine, such as bone and cartilage regeneration, which strengthens its case for dental applications. Bioprinted bone grafts and scaffolds (often using hydroxyapatite composites) have demonstrated success in healing segmental bone defects, and similar calcium-phosphate inks could be adapted for printing dentin or enamel. The ability to incorporate cells into these prints means a living interface or even tissue integration could be achieved. In dentistry, a recent review highlighted myriad potential uses for bioprinting, from periodontal tissue scaffolds and gingival grafts to drug-delivery devices, noting that the technology’s precision and customization capabilities are especially relevant to the small, complex structures of the oral cavity. Bioprinting an enamel–dentin inlay would leverage these strengths: Using a digital design obtained from a scan of the patient’s cavity, a multi-material print could recreate the inner dentin core and outer enamel cap of the missing tooth portion. Such a print might use a high-strength acellular ceramic for enamel and a cell-laden hydrogel for dentin/pulp, or other combinations that yield a functional layered structure. This conceptually illustrates how a digital workflow can produce a bioprinted inlay. First, a 3D model of the tooth defect is obtained. Then, appropriate bio-inks (with or without cells) are prepared and printed to the exact shape. Finally, the construct is matured and conditioned for placement. Notably, 3D printing is compatible with current digital dentistry tools (like intraoral scanners and CAD software), which would facilitate integration of bioprinted inlays into clinical practice when the biological technology matures [1].
A recently published fluorescence micrograph by the UW Dental Organoid Research of a developing enamel organoid (artificial tooth tissue) generated from human stem cells, showing organized regions of differentiating ameloblasts and odontoblast-lineage cells surrounding a dentin-like papilla [7]. This proof of concept for enamel regeneration demonstrates the production of enamel matrix proteins and mineral by lab-grown cells. Beyond tooth‑like constructs, bioprinting has been used to regenerate other dental tissues that are relevant for integration. Image‑based, fibre‑guiding scaffolds printed from composite materials can control the orientation of periodontal ligament fibres and promote integration of Sharpey’s fibres into cementum and alveolar bone [8–11]. In animal models, such scaffolds improved perpendicular and oblique fibre orientation compared with random scaffolds, demonstrating the importance of architectural guidance for periodontal regeneration. Bioprinted dental pulp constructs have also been achieved by encapsulating DPSCs and vascular endothelial growth factor in porous GelMA–dextran hydrogels; these constructs formed vascularised pulp‑like tissues with functional odontoblasts and showed enhanced cell viability, migration, and odontogenic differentiation compared with conventional scaffolds [10, 11]. These examples illustrate how 3D printing can orchestrate cell behaviour and microarchitecture to regenerate the soft tissues that support enamel and dentin.
Bioprinted inlays will rely on tailored bioinks and scaffold materials. Poly(ε-caprolactone) is a widely used aliphatic polyester for bone and dental scaffolds; however, it degrades slowly and exhibits hydrophobic properties. The incorporation of ceramics, such as hydroxyapatite, and natural polymers (collagen, chitosan) can accelerate degradation and improve bioactivity. Multi-material 3D printing platforms (e.g., photopolymer jetting or hybrid extrusion systems) enable the simultaneous deposition of stiff mineral inks for enamel and soft, cell-laden hydrogels for dentin; however, print head clogging and limited mechanical properties remain significant challenges. Digital light processing of ceramic suspensions can produce high-strength zirconia components with compressive strengths of approximately 677 MPa [12] demonstrating that printed mineral layers can approach the hardness of teeth. The selection of appropriate bioinks must therefore strike a balance between printability, mechanical properties, and biological signaling [9–11].
A critical aspect of the proposed protocol is that the bioengineered enamel–dentin inlay must be affixed into the patient’s tooth using adhesive dentistry techniques. Modern adhesive systems, principally resin-based dental adhesives and cements, are well-proven for bonding restorations to natural tooth structure. They achieve micromechanical interlocking and chemical coupling to enamel and dentin, resulting in durable bonds with strengths on the order of tens of MPa.
Recent in vitro evaluations of self‑adhesive resin cements report shear bond strengths of approximately 3.7–6.8 MPa to enamel and 4.5–5.9 MPa to dentin, with predominant adhesive failure occurring at the resin–tooth interface [13]; these values provide realistic expectations for the mechanical performance of cementing bioprinted inlays. Significantly, these adhesives can bond to tooth tissue itself, as evidenced by the success of tooth fragment reattachment in trauma cases. For example, reattaching a broken incisor fragment with resin bonding can restore the tooth’s function and esthetics for many years. In a 9-year clinical follow-up, a re-bonded tooth fragment remained intact and functional, illustrating that the adhesive interface between two pieces of natural tooth can be remarkably resilient [14]. This bodes well for our concept: If an inlay composed of enamel and dentin is prepared, current adhesives should similarly bond it to the remaining tooth structure. The protocol would borrow heavily from the adhesive cementation of ceramic inlays or onlays, which is a routine procedure in restorative dentistry. The cavity surfaces would be conditioned (e.g., acid-etched if bonding to enamel, or treated with a dentin bonding agent for exposed dentin) in the same way as for a conventional filling. The internal surface of the bioprinted/natural inlay could be etched or cleaned as needed. Interestingly, if the inlay’s internal side is dentin, one could apply the same dentin primer/adhesive to that surface as one would on the tooth, essentially creating a hybrid layer on both the cavity side and the inlay side. A thin layer of biocompatible resin cement (such as a light-cure or dual-cure resin cement commonly used for porcelain inlays) would then be used to lute the inlay into place. Because both the tooth and the inlay are made of human hard tissue, excellent wettability and adaptation of the adhesive resin on both sides can be achieved, potentially improving the seal compared with bonding dissimilar materials (such as composite-to-enamel or ceramic-to-enamel interfaces). The polymerization of the resin would lock the inlay in place, and any excess cement would be cleaned from the margins. What results is, in theory, a tooth that is once again made entirely of tooth, with the junction between original and restored portions sealed by a microscopically thin layer of cured resin. Over the long term, such a restoration might also have advantages: A natural enamel surface is less prone to staining or plaque accumulation than composite resin, and it maintains a normal wear profile against opposing teeth (preventing excessive abrasion of antagonists, which can be an issue with ceramic restorations).
One concern is whether bonding an inlay containing vital cells (in a cell-seeded bioprinted construct) could harm those cells or prevent integration. Adhesive resins involve chemicals (e.g., monomers, initiators) that can be cytotoxic before polymerization. In our envisioned protocol, however, the inlay would likely be used in a matured, acellular state—akin to an ex vivo tissue graft. The enamel portion would certainly be acellular (enamel is a mineralized matrix), and the dentin portion could be decellularized or at least not rely on live cells at the time of implantation. Another possibility is that the inlay could include a small portion of organic matrix at the pulp side to encourage bonding with the patient’s pulp or remaining odontoblast processes. Still, such integration is beyond current adhesive concepts and more aligned with transplant biology. For now, the safest assumption is that the inlay would be an inert (non-living) piece of tissue when it is cemented. Thus, existing adhesive protocols are fundamentally compatible with this approach—a significant advantage, as it means dentists would not need an entirely new bonding methodology. Minor adjustments, like specialized primers for the inlay’s dentin surface, could be developed to optimize bond strength, but these are refinements. In summary, adhesive dentistry bridges futuristic bioengineered tissues and present-day clinical techniques, retentioenabling to retain and use of all regenerated tissue by securing it to the surrounding tooth structure [2–5].
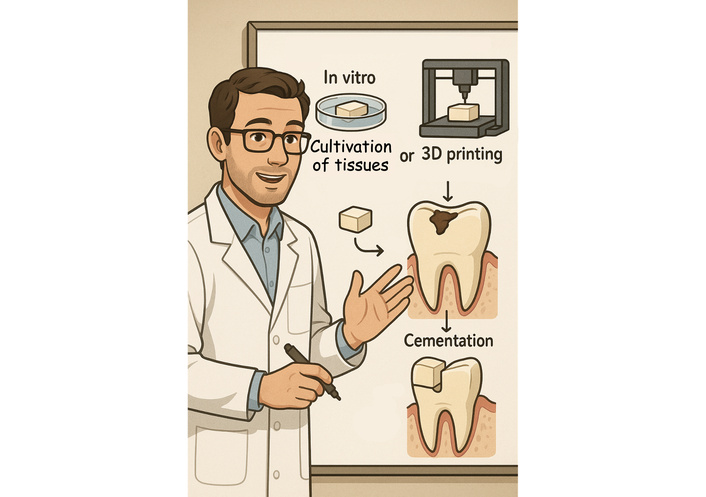
Bringing together the elements above, a hypothetical clinical protocol is proposed for treating a carious lesion with a bioprinted or tissue-engineered enamel–dentin inlay. The steps from diagnosis to cementation are outlined in Figure 1.
The patient is evaluated using standard diagnostic tools (visual exam, radiographs, and, if indicated, novel imaging such as optical coherence tomography to assess lesion depth). Once the carious lesion is indicated for restoration, the dentist conservatively removes the decayed enamel and dentin, preserving as much healthy structure as possible (similar to a minimally invasive inlay/onlay preparation). Care is taken to create a preparation with clear margins and slight divergence, suitable for inserting a preformed inlay. Suppose the caries is very deep and the pulp is exposed. In that case, additional regenerative endodontic procedures (such as pulp stem cell therapy or a pulp cap with growth factors) might be performed concurrently. However, this section focuses on hard-tissue restoration. After caries removal, a clean, shaped cavity remains in the tooth. At this stage, unlike a conventional filling that would be placed immediately, an impression is taken.
A digital intraoral scanner captures the 3D geometry of the prepared cavity and the surrounding tooth anatomy. This yields an accurate virtual model of the defect. Using CAD software, the practitioner or lab technician designs the inlay to fit the cavity precisely, restoring the tooth’s original surface contours. This design process would be analogous to designing a CAD/CAM ceramic inlay, ensuring proper contact points with neighboring teeth and occlusion with opposing teeth. The design includes a map of internal enamel vs. dentin regions. For example, the outer 1–2 mm of the occlusal surface might be designated as enamel, and the underlying bulk as dentin, mirroring the natural tooth structure. The margins would be matched: If the cavity has an enamel margin, the inlay design will have enamel at that edge; if the margin is on root dentin/cementum, the inlay design might incorporate a dentin or intermediate layer there to ensure appropriate bonding [1, 14].
The finalized digital design is sent to a specialized fabrication unit. In a future clinical setup, this could be an in-office bioprinter or a centralized laboratory, depending on the complexity. Two main fabrication routes are possible:
Bioprinting route: A multi-material 3D bioprinter prints the inlay layer-by-layer. For the enamel portion, an acellular mineral ink (consisting of hydroxyapatite or other ceramic, possibly with enamel matrix proteins or amorphous calcium phosphate that will crystallize) is printed in the shape of enamel prisms or a dense layer. For the dentin portion, a bio-ink containing DPSCs or other odontogenic cells in a gelatin/fibrin matrix is printed, allowing it to interface with the enamel layer at the dentin–enamel junction (DEJ) and fill the rest of the shape. Alternatively, a scaffold of dentin matrix (e.g., pulverized dentin from extracted teeth) could be printed and seeded with cells. Some printing approaches may also incorporate reinforcing fibers or polymer networks to achieve immediate strength (similar to printing a PCL lattice, as done by Han et al. [10]). Once printed, the construct might be placed on a tray that exactly replicates the tooth’s cavity shape, ensuring the printed inlay fits. The printed inlay then undergoes a post-print maturation. For example, it could be incubated in culture medium to allow the cells to lay down dentin matrix and mineralize it for a period of days. Concurrently, the enamel layer could be hardened—perhaps by a brief high-temperature sintering (if ceramic) or a chemical treatment that crystallizes the mineral. At the end of this fabrication step, a discrete, handleable enamel–dentin piece matching the cavity is produced.
Natural tissue engineering route: In this scenario, rather than using an automated printer, a lab could engineer the inlay using cellular processes more directly. For instance, a mold of the cavity could be used to culture cells: Ameloblast-like cells could be layered to form enamel on the mold surface, and pulp stem cells could be injected to form dentin underneath. This may involve organoid culture or co-culture, as seen in research settings, guided by signaling factors. Techniques such as organ-on-a-chip or tooth-on-a-chip could provide the necessary microenvironment for cells to form tissues in the correct shape. Compared to bioprinting, this method leverages the natural self-organizing ability of cells, but still requires a mold or scaffold to achieve the desired anatomical form. After a suitable culture period (which could be weeks), the formed complex tissue piece is removed from the mold. It should have a layer of enamel-like mineral, dentin, and possibly predentin. Any viable cells remaining (e.g., within dentinal tubules) could either be retained for potential integration or deliberately devitalized (to avoid immune issues), depending on the strategy.
Before delivery to the clinic, the engineered inlay undergoes quality checks—e.g., verifying its dimensions (it can be tried in on a 3D-printed tooth model of the patient), verifying the hardness of the enamel layer (to ensure it will withstand occlusal forces), and checking that no harmful residuals (unreacted monomers, bacterial contamination) are present. The shade and translucency can also be evaluated; since it’s real enamel and dentin, it should match the patient’s tooth quite well, but slight adjustments or characterizations could be made (for example, adding staining pigments in the lab if needed, though ideally the natural color is correct). One could also incorporate a fluoride-releasing component or an antimicrobial agent into the material as a preventive measure, similar to how some restorative materials are formulated. This is speculative, but it could be an added benefit of the fabrication stage [11, 12].
The patient returns for the insertion of the inlay (this can be done on the same day if fabrication is rapid, or on a second visit if it takes longer). The tooth is isolated under a rubber dam to ensure a dry field of work. The inlay is tried in the cavity to confirm fit; because it was digitally designed, the fit should be very accurate. The dentist then proceeds with bonding: etching the tooth enamel margins with phosphoric acid, applying a bonding agent to the dentin as needed, and also treating the inlay’s internal surface (for example, etching the enamel backing of the inlay if present, and priming any dentin on the inlay). A dual-cure resin cement is applied, and the inlay is seated into the cavity. It should sit fully with minimal pressure if the fit is correct. Excess cement is cleaned, and the cement is light-cured to set it. The margins are then finished and polished. At this point, the carious defect is officially restored—The tooth has regained its full anatomical shape, with a “patch” that is materially the same as what was lost (Figure 1) [13, 14].
The regenerated inlay restoration would be evaluated periodically. Ideally, the junction between the inlay and natural tooth would mineralize further over time, perhaps blurring the line between them. Dentin tubules at the interface could facilitate nutrient diffusion or collagen fiber growth, thereby bonding the two parts (this is speculative, but minor integration could occur if vital cells were present). The patient would treat it like a regular tooth–brushing, flossing, and the restoration should respond to these forces similarly to a healthy tooth. If a pulp vitality test is done and if the inlay contained any living odontoblasts that connected to the pulp, the tooth might even retain normal vitality and sensory function; however, if the inlay were acellular, the tooth’s overall vitality would depend on the original pulp status (which ideally remains healthy if it wasn’t exposed).
This workflow, although complex, leverages several existing technologies (digital scanning, CAD design, and adhesive bonding) and introduces new biofabrication steps that replace the milling or filling processes typically used in traditional methods. The conceptual Figure 1 illustrates this stepwise process, from diagnosis and scanning to bioprinting and cementation, emphasizing how each stage corresponds to current practice with an innovative twist. The prospect of same-day lab-grown fillings might ultimately become akin to how same-day CAD/CAM ceramic crowns are made today—Perhaps an in-office bioprinting unit could produce a finalized inlay within an hour or two, especially as bioprinting speeds and tissue maturation protocols improve [11, 15–17].
While the vision of biologically regenerated inlays is compelling, significant challenges and translational barriers must be addressed before this approach reaches the clinic. Biological complexity: Natural enamel has an intricate hierarchical structure, interlocking enamel prisms with a specific orientation, a gradient of hardness from the outer surface inward, and a seamless interface with dentin. Replicating this precisely via engineering is non-trivial. Current lab-grown enamel does not yet achieve the full mechanical properties of native enamel. It may be necessary to supplement biological processes with advanced materials science (for example, using ceramics or synthetic hydroxyapatite that is then enhanced by cell-derived proteins) to get a functional enamel layer. Manufacturing time and scalability: Growing or printing tissues typically takes hours to weeks. In a fast-paced dental practice environment, a chairside solution must be efficient and effective. One way to mitigate this is through pre-fabrication: Banks of generic enamel and dentin tissues could be grown and stored (either cryopreserved or maintained in a viable state in nutrient solutions), then custom-shaped as needed. However, this raises concerns about immunogenicity, particularly if it is not autologous. Alternatively, one could envision taking a small sample of the patient’s own tissue (such as a pulp biopsy or peripheral blood) well before they need a restoration, and maintaining a personalized cell line that can be used to fabricate any needed tooth parts in the future. This scenario is highly forward-looking and would necessitate changes in dental record management and disease anticipation. In the near term, initial clinical trials of this concept might be in situations like restoring a tooth after endodontic therapy, or in pediatric patients with developmental enamel defects, where traditional restorations have shortcomings—Essentially, high-need cases where a biological repair would be especially advantageous even if it’s a complex process [4, 7].
Material behavior and longevity: Even if an enamel–dentin inlay is successfully developed, its long-term behavior in the mouth remains uncertain. Ensuring durable bonding over time is essential, as the resin bonding layer may remain the weakest link, as in current bonded restorations. There is a possibility of bond failure or microleakage, which could necessitate developing improved adhesive strategies or a biointegrative approach—such as chemically bonding the inlay to the dentin via collagen cross-linking or mineral bridging. Additionally, if the inlay’s dentin is at all porous or contains tubules, they need to be sealed, as they could provide pathways for bacteria or cause sensitivity. One potential advantage, however, is that an enamel/dentin inlay may have thermal expansion and wear characteristics similar to those of the host tooth, thereby reducing secondary stresses and marginal gaps that can sometimes occur with mismatched restorative materials. Additionally, the edges of a natural enamel inlay are expected to undergo remineralization and establish a tight seal with the adjacent enamel, a process not possible with inert materials. Long-term in vivo studies would be needed to validate such benefits [14, 18].
Printed constructs must also recapitulate the optical properties and microstructure of enamel and dentin. Enamel is semi-translucent and exhibits anisotropic refractive indices due to its prismatic architecture. Multi-material printing platforms capable of delivering multiple viscosities and colours can approximate these gradients [19], but achieving seamless shade matching and surface finish will require advances in post-processing and pigmentation. Furthermore, 3D‑printed ceramic restorations, such as zirconia crowns fabricated via digital light processing, demonstrate that sintering temperature and solid content critically influence compressive strength, hardness, and fracture toughness—For example, an 80 wt% zirconia suspension sintered at 1,500°C yielded compressive strength of about 677 MPa and Vickers hardness of 12.6 GPa [11, 13, 16, 17]. Translating these insights to enamel‑like biomineral layers suggests that careful control of particle size, solid loading, and sintering schedules will be necessary to approach the mechanical resilience of natural enamel.
Immunological and safety considerations: If the inlay is produced from the patient’s own cells or tissue (autologous), immunologic rejection is unlikely. However, if any allogeneic components are used (such as a universal cell line or a tissue bank from donors), there is a risk of immune response or disease transmission. Strict protocols, akin to those for organ or bone graft transplants, would be required. Achieving regulatory approval for a living dental implant will require demonstrating safety—No tumor formation from any stem cells, no unintended differentiation, and no harmful degradation byproducts. The field of regenerative medicine is actively addressing these issues (for example, “printing” tissues with precise control to avoid residual undifferentiated cells), and lessons from other tissue-engineered products (such as skin or cartilage grafts) will be instructive [19, 20].
Regulatory and practical barriers: From a regulatory standpoint, a bioprinted tooth patch would likely be classified as an Advanced Therapeutic Medicinal Product (ATMP) or similar, which involves rigorous oversight. The cost of developing and approving such a product will be high, which means initial treatments could be costly. Over time, as technology matures and becomes more routine, costs may decrease. It’s worth noting that dentistry has been at the forefront of adopting new technologies (e.g., widespread use of CAD/CAM, lasers, intraoral scanners), especially when they improve patient outcomes and convenience. If regenerative inlays can be shown to significantly extend the lifespan of a restored tooth (perhaps eliminating the need for a crown or root canal down the line by preserving more natural structure), they could prove cost-effective in the long run [1, 20].
Interdisciplinary collaboration: Making this vision a reality will require cooperation among dental clinicians, biomedical engineers, stem cell scientists, and materials experts. It also invites a rethinking of dental education—Future dentists might need to be trained not just to cut and fill cavities, but also to handle biofabricated grafts, work in partnership with biologic laboratories, and manage biologically restored teeth. It is anticipated that specialized centers or dental laboratories will increasingly focus on producing restorations on demand, similar to the current existence of specialized implant or orthotic laboratories [13, 17, 21–23].
In summary, the path toward bioprinted or regenerated enamel–dentin inlays is challenging but increasingly navigable. The past few years alone have delivered pivotal advances, including the first human enamel organoids, bioprinted tooth analogues, and early-phase clinical trials aimed at regrowing whole teeth (e.g., by modulating the Wnt pathway). Each of these advances addresses a part of the puzzle. It is reasonable to be optimistic that, over the next decade, the shift will be from inert fillings to bioactive, tissue-based restorations. Such a shift would be paradigm-changing, a move from reparative dentistry to true regenerative dentistry. The proposed protocol in this article is admittedly forward-looking, but it aligns with the trajectory of current science and the ever-present dental aspiration to preserve natural tooth structure. By keeping one foot grounded in proven adhesive techniques and the other on the frontier of tissue engineering, the dental profession can aspire to treat a cavity not by substituting foreign material, but by restoring the tooth with itself. This convergence of biology and technology could herald a future where the phrase “drill and fill” is replaced by “grow and glue,” finally curing dental cavities with living solutions [12, 13, 24–27].
Enamel- and dentin-derived inlays for caries lesions represent a visionary intersection of restorative dentistry and regenerative medicine. While significant research and development are still required to bring this concept to clinical fruition, the building blocks are rapidly assembling. Enamel cannot heal itself, but current research enables the growth of enamel-like tissue in the laboratory. Dentin does not readily regenerate significant defects; however, stem cells can be stimulated to form dentin matrices and bioprinted into specific shapes. Adhesive dentistry provides a ready vehicle to deliver and secure these bioengineered tissues into patients’ teeth with minimal intervention beyond the status quo. Early translational steps may involve hybrid approaches, such as partially biological fillings or biomimetic enhancements to current materials. Still, the ultimate goal described here is an anatomically and materially authentic restoration of a tooth. Achieving that will mean a restoration that is not just tooth-like; it is a tooth. The benefits to patients could be immense: longer-lasting restorations, a reduced risk of secondary decay (since margins can remineralize and bond naturally), and the psychological advantage of truly having one’s own tooth back rather than an artificial repair. As this perspective has detailed, numerous challenges remain on the road to clinical implementation, from scaling up tissue fabrication to ensuring safety and integration. Yet, given the pace of advances and the convergence of digital and biological techniques, it is not far-fetched to imagine that, within a generation, dentists will routinely discuss biological inlay options with their patients in some cases. Drawing inspiration from recent scientific literature and innovative future perspectives, this approach maintains scientific rigor while embracing innovation. The concept of a ‘living filling’, previously discussed in popular science articles, is moving toward scientific reality. This development could revolutionize dental healing and potentially serve as a model for regenerating other complex tissues within the body. The restoration of a decayed tooth with bioprinted or regenerated enamel and dentin inlay would be a triumph of interdisciplinary innovation and a milestone for regenerative dentistry, ultimately fulfilling the age-old dental mandate: replacing what is lost with something of equal nature.
DPSCs: dental pulp stem cells
The author may acknowledge those individuals who provided help during the research and preparation of the manuscript. During the preparation of this work, the author used ChatGPT 5.2 to schematically create a workflow figure (Figure 1). After using the tool, the author reviewed and edited the content as needed and takes full responsibility for the content of the publication.
LF: Writing—review & editing, Supervision. The author read and approved the submitted version.
Luca Fiorillo, who is the Editorial Board Member and Guest Editor of Exploration of BioMat-X, had no involvement in the decision-making or the review process of this manuscript.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 4260
Download: 42
Times Cited: 0
Wendy A. Clark ... Ingeborg J. De Kok