Review
Review

Affiliation:
1Department of Cardiology, School of Medicine, Trakya University, Edirne 22030, Turkey
ORCID: https://orcid.org/0000-0002-7552-7654
Affiliation:
2Department of Physical Medicine and Rehabilitation, School of Medicine, Trakya University, Edirne 22030, Turkey
Email: nurkakilli@gmail.com
ORCID: https://orcid.org/0009-0005-3702-7973
Affiliation:
1Department of Cardiology, School of Medicine, Trakya University, Edirne 22030, Turkey
ORCID: https://orcid.org/0000-0001-5650-9066
Affiliation:
2Department of Physical Medicine and Rehabilitation, School of Medicine, Trakya University, Edirne 22030, Turkey
ORCID: https://orcid.org/0000-0002-1033-806X
Affiliation:
2Department of Physical Medicine and Rehabilitation, School of Medicine, Trakya University, Edirne 22030, Turkey
ORCID: https://orcid.org/0000-0003-0294-4155
Explor Musculoskeletal Dis. 2023;1:264–288 DOI: https://doi.org/10.37349/emd.2023.00028
Received: September 11, 2023 Accepted: October 26, 2023 Published: December 06, 2023
Academic Editor: Tony Kenna, Queensland University of Technology, Australia
The article belongs to the special issue Comorbidities in rheumatoid arthritis
Rheumatoid arthritis (RA) is the most common rheumatologic disease characterized by inflammation with a definite relationship with heart disease. Impaired immunity, chronic inflammation, genetic susceptibility, autonomic nervous system (ANS) dysfunction, altered metabolic profile have been blamed for ischemic and non-ischemic heart diseases in RA patients. Medications used in RA treatment can also modify the risk of heart diseases by different mechanisms. Understanding the pathogenesis is essential to prevent early cardiac dysfunction in RA patients. Fundamental cellular and molecular mechanisms of pathogenesis await further elucidation. Disease management is of great importance since the cardiovascular (CV) events are known to be reduced with low disease activity. Discovery of new mechanisms will pave the way for the development of novel treatment modalities. This review highlights the epidemiology, pathogenesis, risk factors, diagnosis and screening methods and management of CV comorbidities in RA patients. Besides impact of RA medications and exercise on CV risk are summarized.
Rheumatoid arthritis (RA) is the most common rheumatological disease characterized by chronic inflammation, seen in 1% of the population [1] affecting mainly hand, foot and knee joints as well as cardiovascular (CV), respiratory, visual and nerve systems. Extra-articular comorbidities are blamed for decreased life expectancy in RA patients. Among these, CV disease (CVD) is reported to be the main cause of death [2]. RA patients have 1.5 times higher risk of developing CVD compared to normal population [3]. Three to ten years of decreased life expectancy compared to the general population is reported due to excess CV events [4].
It has been shown that having an immune mediated disease is a risk factor for developing cardiac inflammatory conditions [5–9]. Coronary artery disease (CAD), heart failure (HF) and atrial fibrillation (AF) risk are known to be increased in RA patients [10, 11]. Nevertheless, RA patients still do not receive adequate diagnosis and treatment for CV risk factors. Although advances in RA treatment are thought to decrease CV risk to some extent, mandatory screening for CV risk factors is needed for all RA patients.
A nationally representative population-based study investigating the association between RA and CVD among US adults during 1999–2018, reported that strength of RA and CVD association reduced over time but the downward trend was not statistically significant [12]. They also reported that the relative risk of CVD is higher in younger adults (< 50 years), while the absolute risk is also higher in older adults which necessitates effective RA treatment regardless of age [12]. Another recent population-based cohort study stated that major CV events in RA has declined in recent decades and the gap between RA patients and general population in terms of CVD incidence is getting closer which is mainly attributed to early initiation of treatment, use of biologic disease-modifying anti-rheumatic drugs (DMARDs), effective control of disease activity and timely management of CVD risk factors [13]. Although the improvement was reported to be largely driven by > 50% decrease in the incidence of myocardial infarction (MI) in recently diagnosed RA patients, there was no statistically significant decline in ischemic or hemorrhagic stroke rates [13].
In this review by pooling up-to date information, the proposed mechanisms in the pathogenesis, clinical manifestations, risk factors, diagnostic strategies, prevention and treatment approaches of CV comorbidities in RA are summarized.
Higher frequency of heart diseases in RA patients can be analyzed under two major headings: “ischemic heart diseases” and “non-ischemic heart diseases”. The pathogenesis of ischemic heart diseases, which include angina, MI, cardiogenic shock, cardiac arrhythmia and sudden cardiac death, are attributed to endothelial dysfunction, atherosclerosis, aortic stiffness and vulnerable plaques [14]. Differently, non-ischemic heart diseases are associated with changes in cellular composition and architecture of cardiomyocyte such as myocarditis, pericarditis, myocardial fibrosis, systolic or diastolic dysfunction, conduction defects and valvular abnormalities [14]. Cardiac involvement patterns are examined in detail under the following headings.
Subclinical changes in heart have been observed despite the absence of evident cardiac symptoms in RA. Up to half of RA patients with no diagnosis and clinical manifestation of CVD showed cardiac fibrosis and inflammation [15, 16]. Systolic and diastolic left ventricle function was found to be reduced in up to half of RA patients with no cardiac manifestations [17, 18]. Echocardiographic studies also showed asymptomatic pericarditis and valvular involvement [19]. Another study revealed dysfunction of coronary microcirculation in 1/3 of cardiac asymptomatic RA patients via measurement of myocardial flow reserve [15]. Coronary plaques measured by computed tomography (CT) angiography were found out in higher prevalence and severity in RA patients [20] and the risk of having a silent (unrecognized) heart attack was observed to be doubled in rate [21].
Epidemiological studies showed that 51% of long-standing RA patients have a Framingham risk score over 20%, meaning increased frequency of CV ischemic events [22]. Therefore, an expert committee of the European Leage Against Rheumatism recommends that CV risk scores (e.g., Framingham) should be multiplied by 1.5 in RA patients to draw attention to the increased risk in this patient group [23].
Patients with a diagnosis of RA have 1.5–2 times higher risk of developing CAD compared to the general population [21, 24] and this risk is equivalent to that in type 2 diabetes patients [25, 26]. Similarly, Lindhardsen and colleagues [27] reported that the increased acute MI risk was similar in magnitude that was expected in diabetes mellitus patients. A cohort study of 1,135 patients with RA and acute coronary syndrome showed that sudden cardiac death, ST-elevated MI (STEMI), elevated levels of troponin, inpatient complications were more common in RA patients, implying that acute coronary syndrome is expected to be much more severe than in general population [28]. In another study the incidence of heart attack was found equal to 10 years older non-RA patients which was 70% higher compared to normal population of the same age [27]. Considering that the history of having a heart attack is 3 times higher in individuals diagnosed with RA for the first time, compared to the normal population [21], the CV risk should be considered to have increased long before the diagnosis was made.
Interestingly, CAD presents a silent clinic in most patients with RA [21]. Chest pain during an acute coronary event is less expected in patients with RA than in the general population [29]. Even though the exact cause is unknown, absence of clinical angina pectoris may be due to not being physically active enough to cause angina, attributing pain to RA itself or altered pain perception by RA medications.
Ischemic heart disease, inflammatory mediators, medications and amyloidosis can lead to the development of HF in RA [30]. The most frequently blamed factors in the development of HF in RA patients can be listed as follows: (1) ischemic cardiomyopathy due to increased CAD; (2) treatment-related cardiomyotoxicity; (3) granulomatous (less frequently necrotizing or non-specific) myocarditis secondary to inflammation and (4) infiltrative cardiomyopathy due to AA-type amyloidosis secondary to RA [31]. Patients with RA have 2-fold increased risk of HF [32]. This risk is more pronounced in patients who are seropositive for rheumatoid factor (RF).
Clinical presentation of HF is distinct in RA patients. Even though having a better cardiac function and lower blood pressure, higher mortality rates are expected [33]. RA patients rarely show expected sign and symptoms of HF and respond poorly to treatment with a worse prognosis [33].
Preserved ejection fraction (EF) is often expected (> 50%) in RA patients with HF and clinical findings of CAD are expected to a lesser extent [34] because HF seen in RA is often related to diastolic dysfunction, which may be related to systemic inflammation. The progression of HF in RA patients may be due to elevated levels of C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), RF, anti-citrullinated protein antibody (ACPA) [21]. Therefore, disease activity score-28 (DAS-28) can be used as a measure in the estimation of HF in RA patients [35].
Pericarditis is among the most common cardiac complications of RA and it may develop even before the disease is diagnosed. Even tough 20–50% of RA patients show pericardial involvement on echocardiography (ECG), less than 15% are clinically symptomatic with chest pain or dyspnea and less than 10% have hemodynamic abnormalities [36]. Autopsy studies showed that 20–40% of seropositive patients for RF had pericarditis [37]. Restrictive pericarditis with tamponade is extremely uncommon.
Myocarditis is a rare complication of RA. It is mostly seen in active disease with other extraarticular manifestations [38] and may be granulomatous or interstitial. Granulomatous type has higher specificity for RA. Endocardial involvement may result in mitral insufficiency while involvement of conduction system results in atrioventricular block.
Rheumatoid nodules can develop in the myocardium, pericardium, cardiac valves and can cause different manifestations such as syncope, arterial embolization, valvular insufficiency and death according to the site of formation. Furthermore, anti-rheumatic drugs may cause acute myocardial dysfunction [39].
Conduction abnormalities can be seen in RA patients due to local ischemia, rheumatoid nodules, HF or amyloidosis. Even in the absence of structural hearth anomalies, risk of fatal arrhythmias is found to be increased in RA patients [40].
In terms of AF, the results of the studies are conflicting. Atrial tissue affected by systemic inflammation in the background of RA undergoes structural and electrical remodeling. Greater than 40% increase in the incidence of AF and a 5-fold higher thromboembolism rate are reported in a prospective cohort study of 18,247 RA patients [11]. On contrary, another cohort study involving 20,852 RA patients and 104,260 control patients reported no difference in AF risk when comorbidities and medications are adjusted [41]. CRP level, evidence of systemic inflammation, is shown to be correlated with autonomic dysfunction and QT corrected for heart rate (QTc) prolongation [40].
Hypertension (HT) is a common CV comorbidity in RA patients. RA patients have increased peripheral vascular resistance due to oxidative stress, endothelial dysfunction and genetic polymorphisms resulting in increased blood pressure. Some agents used in RA treatment have been shown to cause HT via different pathophysiological pathways. Non-steroidal anti-inflammatory drug (NSAID) therapy may cause HT by activating the renin-angiotensin-aldosterone system, glucocorticoid therapy may increase sodium absorption and vascular tone (prednisolone ≥ 10 mg/day or equivalent), and leflunomide may cause HT by increasing sympathetic activation [42].
The effect of RA on non-cardiac vascular diseases is not clearly known yet. Although there are reports showing increased rate of cerebrovascular disease in RA patients [43], there are also publications claiming the opposite [44].
Venous thromboembolism risk is found to be increased 2–3 times compared to the general population [44, 45]. The risk of peripheral vascular disease seems to be increased, especially in patients with extra-articular involvement [46–48]. Pulmonary HT can also be a rare complication in patients with RA. Rheumatoid vasculitis may rarely cause coronary arteritis but in the absence of other extra-articular involvement, it is unlikely to cause MI.
Many different mechanisms have been proposed to explain cardiac involvement in RA patients. In addition to the previously known mechanisms, novel mechanisms under investigation are discussed below.
Impaired immunity and chronic inflammation seen in patients with RA may be responsible for the cardiac involvement and understanding them may shed light on the development of novel therapeutic targets for disease prevention. The cornerstone of the ischemic CV events is thought to be chronic inflammation. In patients with RA, elevated CRP, indicating systemic inflammation, is an independent prognostic marker of CV mortality [49]. Seven percent increase in CV risk was reported with each period of increased inflammation in the joints [50]. It has been shown that RA patients with increased disease activity have more unstable plaques at carotid artery by ultrasonography (USG) [51] and CT angiography [20].
Inflammation in the synovium is also seen in the vascular wall of RA patients [52] which explains why both the inflamed synovial membrane and the inflamed atherosclerotic plaques show similarity in terms of abnormal immune responses [53, 54]. An autopsy study comparing coronary artery pathology among RA vs. non-RA patients who died after having MI, showed that even though RA patients have less atherosclerosis compared to the control group, their plaques were more inflamed and unstable [55].
Unlike ischemic CV events, the role of chronic inflammation in non-ischemic CV events is less well known. Although atherosclerosis and chronic inflammation is mostly blamed so far, there may also be different mechanisms that can lead to cardiac dysfunction. It is discussed that diastolic dysfunction can be seen in RA patients even in the absence of detectable atherosclerosis. This situation gives rise to the hypothesis that there may be as yet unexplained mechanisms in the development of early cardiac dysfunction that precede the development of atherosclerosis.
It is thought that inflammation may cause myocardial fibrosis leading to systolic and diastolic dysfunction and arrhythmias. The correlation between RA disease activity and myocardial inflammation and fibrosis has been shown by cardiac magnetic resonance imaging (MRI) and positron emission tomography and CT (PET-CT) [15, 56]. Also, the prevalence of diastolic HF was increased in RA patients with increased disease activity and high CRP levels [57]. Another supporting data is that myocytes of RA patients with low disease activity showed normal structure and function [58, 59]. Inflammation is both cell and cytokine mediated.
Studies show that T lymphocytes play an important role in the pathogenesis of both RA and heart diseases [60, 61]. It is well known that T cells are pathogenic in both RA and heart disease. Antagonization of T cell co-stimulation is proven to be efficient in RA treatment [62]. Comparably T-cell inhibiting drug eluting stents (e.g., sirolimus) are proven to be efficient in preventing in-stent restenosis in CAD [63].
Both in RA and heart disease, CD4+ T cells lose expression of co-stimulatory molecule, CD28. The number of so called “CD28null T cells” is known to be related to the extent of extra-articular involvement [64, 65]. These cells have restricted antigen specificity due to limited T-cell receptor (TCR) Vβ chain, causing autoimmune diseases and first identified in the plaques of patients with unstable angina [66]. They are thought to produce cytokines and kill vascular smooth muscle cells [67]. A reduction of circulating CD28null T cells has been reported in RA patients treated with abatacept and this was correlated with reduction of disease activity [68–70].
Regulatory T (Treg) cells, known for their anti-inflammatory effect, are reduced in RA patients and the increase of CD28null T cells compared to Treg cells worsens the disease activity as well as thinning the fibrous cap, making the atherosclerotic plaque susceptible to rupture [71].
Another mechanism appears to be caused by premature senescence of T cells in RA. Thymic emigration of T cells is lost at fifth decade, which is the common time period for RA and heart disease onset. This suggests that T cell senescence plays a role in the pathogenesis of both diseases. In the future, drugs targeting rejuvenation of these senescent T cells could be a potential treatment option in prevention and treatment of CVDs [72].
Many effects of B cells on CV system have been described. In addition to autoantibodies released by memory B cells, B cell activating factor (BAFF) and chemokine CC motif ligand 7 (CCL-7) synthesized by mature B lymphocytes may also cause cardiac damage [73]. Metalloproteinase-9 which is responsible for degrading extracellular matrix both in joints and heart is also expressed by activated B cells in RA patients. B cells have also been implicated as key immune cells in the development of atherosclerosis. This effect was subset specific, with B1 cells inhibiting [74] and B2 cells promoting [75] atherosclerosis.
Increase in pro-inflammatory cytokines [tumor necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β), IL-6, IL-17] in RA have been associated with the pathogenesis of CV events. With the release of inflammatory mediators, endothelial barrier function is disrupted and up-regulated chemokine and adhesion molecule production promotes plaque formation by recruiting circulatory leucocytes. In addition, with chronic inflammation, bioavailability of nitric oxide (NO) decreases and reactive oxygen species are generated.
Interferon-γ (IFN-γ) and IL-17 production is shown to be enhanced in joints affected by RA, which causes chronic inflammation as seen in heart disease [76, 77]. Another observational study reported that, increased levels of TNF-α and IL-6 was associated with the development of subclinical atherosclerosis and this was independent of Framingham risk score and diabetes mellitus [78].
Increased cardiomyocyte apoptosis and hypertrophy and decreased contractility was reported due to IL-1 [79]. Prolonged exposure to increased levels of IL-6 negatively affects systolic function [80]. IL-17 plays role in the development of CVD and endothelial dysfunction by altering microvascular function and arterial compliance [81]. It is also shown to promote formation of atherosclerosis and cardiyomyocyte fibrosis in animal models without RA [82, 83].
Elevated levels of TNF-α were found to be associated with increased ischemia-perfusion injury, myocarditis, allograft heart transplantation and HF in RA [84]. Possible mechanisms of TNF-α in the development of atherosclerosis are endothelial dysfunction causing vascular instability, recruitment of inflammatory cells at injured site and reverse remodeling of smooth muscle cells. TNF-α also promotes cardiac hemodynamics by regulating contractility and peripheral resistance.
Before overt synovitis that is clinically detectable, genetically susceptible host for RA has a preclinical, asymptomatic phase in which behaviors and environment play crucial role in delaying or potentially preventing RA onset [85].
The major risk gene for RA, human leukocyte antigen-DR isotype1 (HLA-DRB1), promotes the selection and survival of auto-reactive CD4+ T cells which predisposes to disease. HLA-DRB1 alleles are also known to increase the risk of MI and other forms of non-RA associated heart disease [86, 87]. HLA-DRB1 positivity predisposes to expansion of CD28null T cells in RA and CAD [88].
From epigenetic perspective, non-coding RNAs, including microRNAs (miRNAs), long noncoding RNAs (lncRNAs) and circular RNAs (circRNAs), are known to play important roles in the regulation of inflammation and autoimmunity [89]. Epigenetic mechanisms may be responsible from enhanced inflammation and joint destruction in RA patients. Correlatively, non-coding RNAs are being studied as significant novel regulators of CV risk factors and cell functions which make them therapeutic target candidates [90].
It was shown years ago that RA patients have signs of autonomic dysfunction affecting CV nervous system. Chronic inflammation can lead to imbalances in autonomic nervous system (ANS) which then causes a vicious circle between inflammation and ANS [91].
Chronic inflammation in RA increases sympathetic activity while suppressing the parasympathetic function [92]. In a rat collagen-induced arthritis model study it is hypothesized that increased sympathetic drive of heart, so called “inflammatory reflex”, may cause CV problems [93]. The results of the study showed that even after the relief of arthritis attack and decline of sympathetic activity, the autonomic dysfunction in heart persists [93].
It has been found that that long term exposure of cardiomyoctes to high concentrations of epinephrine may lead to phosphorylation of beta-1 adrenergic receptors (β1-ARs) by G protein coupled receptor kinase-2 (GRK2), also known as β-AR kinase (βARK), resulting in receptor desensitization and endocytosis [94]. Chronic GRK2 hyperactivity may cause impairment in the contractility of cardiomyocytes leading to CV dysfunction [95]. Based on this hypothesis, it is proposed that GRK2 inhibitors can be used in the prevention of cardiac events and may modify disease activity in RA patients [96]. There is no doubt that further clarification is needed to understand the role of GRK2 to determine if GRK2 inhibition may be a new treatment target of cardiac therapy.
With the effect of chronic inflammation in RA, lipoprotein structure and function changes [97], serum amyloid A load carried by high-density lipoprotein (HDL) increases and apolipoprotein A-I decreases [98]. Furthermore, inflammation reduces the ability of HDL molecule to accept cholesterol from macrophages, so called “cholesterol efflux capacity” [99, 100] which turns the HDL effect from anti-atherogenic to pro-atherogenic [98].
Although the levels of total cholesterol, low-density lipoprotein (LDL) and HDL levels were all found to be decreased in RA patients, higher decrease in HDL cholesterol is observed. This increases CV risk by increasing atherosclerosis index (total cholesterol/HDL cholesterol) [101]. Lipid profile in RA patients is characterized by a higher suppression of HDL than LDL and total cholesterol during periods of high inflammation. This is called the “lipid paradox” and is associated with more severe systemic inflammation [102].
RA induced insulin resistance aggravates systemic inflammatory response and is associated with seropositivity [103, 104], pro-inflammatory cytokines, disease activity and glucocorticoid usage [105, 106]. Serum retinol binding protein 4 (RBP4) is found to be elevated in diabetes patients and it’s level is also detected higher in RA patients compared to controls and is relevant to the severity of RA [107]. Visceral adiposity seen in RA patients was found to be associated with insulin resistance, HT, metabolic syndrome and increased inflammatory burden [108].
Uncontrolled inflammation and lack of physical activity leads to decreased muscle mass resulting in low body mass index (BMI). It has been shown that RA patients have altered body composition (high fat mass, low muscle mass) and decreased physical function even when the disease is in the remission phase meaning that metabolic deficits sustain [109, 110].
Moreover, RA patients are reported to have reduced oxidative metabolism in both T cells and skeletal muscle via metabolic reprogramming, resulting in increased invasiveness of immune cells, disease activity and disability [111, 112]. It has been revealed that altered naive CD4+ T cell metabolism is associated with pro-inflammatory function and characterized by reduced glycolysis and low oxidative ATP production [112, 113] which adversely affects cardiorespiratory fitness.
Chronic inflammatory autoimmune diseases (CIADs) increase the possibility of mortality and morbidity by causing an increase in CV risk. According to the European Society of Cardiology (ESC) 2021 guidelines on CVD prevention; even the subclinical period, early arthritis period or symptomatic period of less than one year increases the risk of atherosclerotic CVD (ASCVD) by 50% in patients with RA [114, 115].
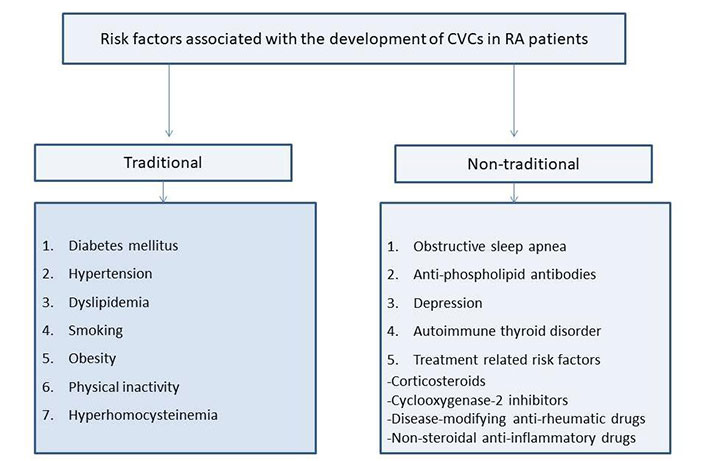
Increased CVD risk seen in RA patients cannot only be reduced to traditional risk factors but also RA-specific conditions such as seropositivity and disease activity [116]. In RA patients some traditional risk factors such as smoking, HT and dyslipidemia have increased prevalence compared to general population. So, it is critically important to control both the CV risk factors and the disease activity. While persistent disease activity was shown to increase CV events mainly in RA patients with pre-existing CVD, traditional risk factors like HT, hypercholesterolemia held responsible from CV events in RA patients without CVD [117]. Even if the risk factors and the disease itself are well managed, the risk of developing MI in RA patients is more than twice that of normal population [118]. The accepted traditional and non-traditional risk factors for CV comorbidities (CVCs) in RA patients are shown in Figure 1.
It is estimated that CV mortality accounts for half of all causes of death in RA patients. The aim of treatment in RA is to reduce the disease activity and to control chronic diseases that may develop due to it. This should be based on the suppression of inflammation [119].
“Lipid paradox” seen in RA patients is known to be associated with more severe systemic inflammation. Despite having lower levels of lipoprotein compared to general population, RA patients carry increased CVD risk [120]. Coronary artery calcium (CAC) scores were detected highest among patients whose LDL cholesterol level was below 70 mg/dL [121]. A cross-sectional observational study showed that, pro-atherogenic HDL form was importantly associated with disease activity and joint damage and was detected less frequently in patients using methotrexate (MTX) [122]. Again paradoxically, the incidence of CVD was found to be increased in RA patients with low BMI [123]. Low BMI is associated with worse prognosis [124]. Decreased muscle mass and accompanying increased fat mass poses CV risk [108]. These paradoxical situations suggest that mechanisms different from normal population may play a role in CV morbidity and mortality in RA patients.
HT is common in RA patients, mostly being underdiagnosed and undertreated. In RA patients, it has been shown that being diagnosed with HT or type 2 diabetes mellitus doubles the risk of CV morbidity [125].
In addition, high inflammatory markers (CRP, ESR, RF, ACPA) are associated with more active and severe RA [126]. RF and ACPA positivity were associated with increased heart disease and overall mortality, even in individuals without rheumatologic diseases [127]. Even though the mechanism is still unknown, RF-positive RA patients were detected to be more prone to CV events with high dose glucocorticoid exposure than those who are seronegative [128].
Duration of the disease can be a risk factor by itself. An ultrasonographic study has been shown that prevalence of carotid plaques was increased with the duration of disease [129, 130]. Conformably, other studies showed that patients with established RA had more calcification of coronary arteries detected by CT angiography than patients with early RA and healthy control group [131–133].
Apart from these general risk factors; high homocysteine level, being positively associated with RA disease activity and non-remission state, is shown among CV risk factors by several different mechanisms [134]. Proposed mechanisms are endothelial dysfunction and atherothrombosis due to oxidative stress, besides NO depletion. Release of pro-inflammatory cytokines and the formation of oxidized LDL (oxLDL), causes atherosclerotic plaque formation and vascular calcification [135].
The largest observational RA-related study involving 25,987 patients reported clinically relevant and meaningful variations of CVD and CV risk factors across different geographic regions [136]. This suggests that genetic predisposition and environmental factors may determine a RA patient’s CV risk. Nowadays, prevention of CV comorbidities is now among the targets of RA management. As our knowledge increases about the impacts of CVD risk factors in RA patients, clinical management approaches could be tailored to develop successful cardio-protective therapies for RA patients.
RA treatments mainly aim to suppress chronic inflammation, which is the main risk factor for CVD and thus may modify CV risk. However, no marked beneficial CV affect have been reported for any class of below mentioned medications. Drug selection should be patient-specific and the lowest effective dose should be used for the shortest time.
In addition to providing a beneficial anti-inflammatory affect, glucocorticoids may aggravate heart disease by increasing CV risk factors. Their adverse metabolic effects may outweigh their anti-inflammatory benefits. Blood pressure and glucose levels should be regularly monitored before and during treatment.
It has been reported that even 1-year treatment with corticosteroids in newly diagnosed RA patients, significantly increases the risk of non-ischemic HF [137]. The risk of heart disease in patients using high-dose (> 7.5 mg/day prednisolone) steroids is twice that of patients not using steroids [128].
Cyclooxygenase-2 (COX-2) inhibition increases blood pressure, promotes atherosclerotic plaque rupture and thrombosis by reducing prostacyclin levels [138]. The Vioxx Gastrointestinal Outcomes Research trial (VIGOR) study reported an increased risk of heart disease with use of rofecoxib, leading to withdrawal of the drug from the market [139]. In another study, no difference was found in the development of heart disease between patients using celecoxib and ibuprofen [140]. A meta-analysis of seven NSAIDs, 4 of which were coxib group, showed that naproxen had the lowest CV risk while other 6 NSAIDs were found similar in terms of CV risk [141].
MTX, the first line treatment, has been associated with lower CV risk. Recent meta-analysis reports that CV events decreased by 21% with MTX use [142]. Another meta-analysis also reports reduced risk of major CV events with MTX use [143]. Interestingly, in a recent study MTX failed to prevent CV events in non-RA patients with CVD [144]. This could be interpreted as cardio-protective effect of MTX can only be seen under inflammatory conditions. It is thought that MTX does not alter the lipid profile. It’s effect on insulin resistance, HT and atherosclerotic plaque formation is not yet known. Furthermore, MTX, itself, increases homocysteine production which has pro-atherogenic effects on endothelial cells and stimulates LDL oxidation.
Hydroxychloroquine is found cardio-protective in most studies [143, 145, 146] and may inhibit platelet aggregation and thrombogenic effects of anti-phospholipid antibodies [147]. It is known that hydrocychloroquine is known to reduce risk of diabetes [148], levels of LDL and total cholesterol/HDL ratio in RA patients [149]. However, anti-malarials may also cause cardiomyopathies in RA patients [150].
Treatment with sulfasalazine in RA patients has been associated with lower CV risk compared with patients who never used sulfasalazine, MTX or hydroxychloroquine [151]. Leflunamide is also associated with lower rate of MI in RA patients [146] but different from other conventional DMARDs it may aggravate HT by increasing blood pressure [152].
Rituximab (a humanized chimeric anti-CD20 monoclonal antibody) was shown to improve vascular pathophysiology in RA patients [153]. Depletion of B cells via CD20 monoclonal antibody was shown to inhibit atherosclerosis in mice [75]. Antibody therapy against BAFF, important for survival of B cells, has failed to decrease atherosclerosis in mice which suggests a distinct mechanism of action [154]. Clinical trials showed that safety profile of rituximab was similar to anti-TNF-α treatments [155]. Abatacept (T-cell co-stimulation inhibitor) is shown to have no effect on the risk of developing HF in RA patients when compared to etanercept [156].
TNF inhibitor therapy has been associated with a reduced risk of all heart events [157]. A recent clinical study reports that anti-TNF-α therapy effectively reduces the incidence of acute coronary syndrome in RA patients [158]. This effect is thought to be due to controlling inflammation rather than modifying CV risk factors. Myocardial inflammation on positron emission tomography (PET) imaging, which is correlated with disease activity, was shown to be reduced in patients using biological DMARDs compared to patients using conventional DMARDs [15, 16].
TNF inhibitors increase total and HDL cholesterol levels resulting in stable atherogenic ratio [159]. Since RA activity is inversely related to HDL level, it is thought that drugs regulating disease activity may improve HDL levels [160]. However, there is no clear information yet whether this effect on lipid profile is a class effect or whether specific TNF inhibitors provide a more favorable lipid profile. Conversly, anti-TNF-α therapies in RA patients may also be associated with elevated risk of developing HT [161].
Although most data [162–164] shows that anti-TNF-α treatment reduces HF risk and improves survival in RA patients, in elderly population it might worsen HF and decrease survival [165]. It’s beneficial effect might be more evident in women [163] and younger patients [162] with RA. Infliximab has been shown to increase heart function and preserve left ventricular function [166]. In contrast, Infliximab was shown to adversely affect the prognosis in patients with HF [167].
In summary, anti-TNF-α therapies reduce risk of CV events in RA patients with preserved cardiac function, but in patients with HF they may not improve cardiac function and even might worsen it. Further studies are needed to clarify the effects of anti-TNF-α therapies in RA patients with serious HF.
Tociluzumab (humanized antibody targeting IL-6) has been found to be associated with increased HDL, LDL and triglyceride (TG) levels [168]. It was shown to be a safe alternative for etanercept in terms of development of major CV events [121]. Although tocilizumab is successful in suppressing disease activity, it may impair lipid homeostasis meaning to have uncertain CV outcomes [169, 170].
Despite worsening the plasma lipid profile, tofacitinib or baricitinib were not associated with increased CV risk in RA patients. It is known that statins can reverse dyslipidemia in tofacitinib treated RA patients [170].
It seems rational for patients diagnosed with RA to undergo a baseline cardiac evaluation before the onset of CVD symptoms and signs to modify existing risk factors and to allow early recognition of all cardiac dysfunctions that may develop later. Lipid profile control is important for the primary prevention of CAD and is performed according to the systemic coronary risk evaluation-older persons (SCORE2-OP) scale under the guidance of the ESC [115]. Although patients with RA have an increased risk of CVD, the effectiveness of initiating lipid-lowering therapy for primary prevention in individuals with a SCORE2-OP value ≤ 5% has not been demonstrated. In patients with a SCORE2-OP value of 5–7.5%, it has been reported that it is useful to decide according to the calcium score, indicating the calcific lesion load in the coronary arteries [115].
The main point for early diagnosis of CAD in patients with RA is high awareness. The diagnostic algorithm should include follow-up in accordance with international guidelines. In addition to the cardiac treatments recommended by the guidelines DMARDs should be planned to control the risk factors and RA activity. The efficacy of acetylsalicylic acid (ASA) as prophylaxis in patients with RA has not been demonstrated [171]. The use of low-dose ASA (75–150 mg/day) for secondary prevention in these patients was similar to that in the general population. The addition of non-ASA NSAIDs to ASA-treated patients may decrease the antiplatelet efficacy of ASA and increase CAD activation. Therefore, the use of non-selective NSAIDs (including selective COX-2 receptor blockers) at a low dose for as short duration as possible is recommended for CAD prophylaxis [171]. The management of CAD (acute or chronic coronary syndrome) and treatment goals in patients with RA are similar to those in patients without RA [115]. In these patients, especially the use of potent statins (atorvastatin or rosuvastatin) reduces the development of new CVD and suppresses the inflammatory response. Again, effective inflammation control with DMARDs in this patient group reduces the risk of CVD development [172].
Pericardial involvement is mostly silent (symptom rate < 10%) and usually develops towards the end of the first decade after diagnosis but may be observed between 1–30 years depending on the course and severity of RA [173]. The disease usually presents with mild-to-moderate exudative pericardial effusion with symptoms of pericarditis and has a mild course. Advanced age, comorbid CVD and persistent fever increase the likelihood of a progressive and fatal disease course. Therefore, the management of the disease varies according to the symptoms and amount of pericardial fluid. For this purpose, echocardiographic examination is the gold standard for diagnosis and follow-up. Asymptomatic patients with pericardial fluid limited to a few millimeters do not require additional treatment or regimen modifications. Adding NSAIDs to the treatment regimen according to symptom status is sufficient. Invasive treatment is indicated in cases of tamponade or constrictive pericarditis. The agents used for treatment in the presence of pericarditis in RA patients are shown in Table 1 [174].
Medical management of RA patients with pericarditis
| Medical management |
|---|
| Prednisone 0.3–0.5 mg/kg per day taped over 2–4 weeks |
| MTX up to 20 mg per oral (PO) or subcutaneous (SQ) weekly |
| Leflunomide up to 20 mg daily PO |
| Optimization of DMARDs |
The evaluation of RA patients in the asymptomatic phase with conventional or advanced cardiac imaging modalities [such as 2 dimensional (2D)/3D ECG and strain ECG] allows the detection of subclinical left ventricular dysfunction. In cases of symptomatic HF developing in patients with RA, treatments recommended by current guidelines should be initiated immediately and RA medications that may cause cardiomyopathy should be discontinued. Prednisolone (or equivalent) at doses of ≥ 7.5 mg/day, NSAIDs, antimalarial drugs, especially choloroquine/hydroxychloroquine, and TNF-α inhibitors have been shown to cause cardiomyopathy in association with RA treatment. The recommended agents for RA patients with HF are shown in Table 2 [175].
Recommended RA medications in patients with moderate HF
| Recommended RA medications |
|---|
| Antimetabolite MTX |
| Selective T cell blocker: abatacept |
| Monoclonal antibody rituximab |
| NSAIDS: low dose ASA or selective COX-2 receptor blockers |
In resistant cases (New York Heart Association functional class 1–2) Infliximab ≤ 3 mg/kg Adalimumab ≤ 40 mg every two weeks Etanercept ≤ 50 mg/week |
Myocarditis is a rare complication that usually occurs during periods of disease exacerbation in patients with extensive extra-articular involvement [176]. The most common form is granulomatous, which may present with symptoms of mitral regurgitation or atrioventricular block. More rarely, there may be a nonspecific or necrotizing form with local involvement [32]. Although echocardiographic evaluation is initially recommended for diagnosis, cardiac MRI, 18-fluorodeoxyglucose (FDG) PET and cardiac biopsy are recommended in cases with rapid progression that are unresponsive to treatment. Treatment recommendations for myocarditis attacks in RA patients are shown in Table 3 [177].
Treatment of RA-related myocarditis
| Treatment |
|---|
| Methylprednisolone (pulse therapy 500 to 1,000 mg/day for three days or 80 mg daily) |
In cases unresponsive to glucocorticoid therapy Azathioprine Cyclophosphamide |
The use of anti-TNF in this group of patients is controversial and it is recommended that decisions be made according to the patient’s clinical condition. Although it is known to increase mortality, especially in patients with advanced HF with functional capacity class 3–4, use of anti-TNF was shown to suppress myocardial inflammation and reduce secondary myocardial fibrosis in mild cases [15, 178].
Long-term use of glucocorticoid therapy in RA patients increases the likelihood of AF development, whereas hydroxychloroquine and anti-TNF medications decrease AF development [179]. Another point to be considered in these patients is that the association of RA with amiadoran treatment given for rhythm control increases the risk of pulmonary fibrosis [180].
In terms of HT, regular blood pressure checks are recommended for all patients even if they are asymptomatic but especially for those receiving NSAIDs, glucocorticoids or leflunamide treatments.
Exercise, a widely used non-pharmacological prevention and treatment method in RA patients, shows promise in reducing symptoms and providing functional gain [181]. Furthermore, it may also increase cardiorespiratory fitness and reduce disease activity and severity [182]. Thus, European Alliance of Associations for Rheumatology (EULAR) has recommended combining drug and exercise therapy in 2018 guidelines [183].
Aerobic exercise has been reported to decrease CVD risk in RA patients. A meta-analysis with 13 RCTs including 967 RA patients reported that there was statistically significant improvement in functional ability and aerobic capacity besides decrease in pain scores with aerobic exercise [184].
Decreased cardiorespiratory fitness [as measured by relative oxygen consumption (VO2) peak] is a strong predictor of CVD and overall mortality. Improvement in cardiorespiratory fitness in RA patients with high intensity interval training (HITT) was reported to be associated with increase in the amount of anti-inflammatory cytokine IL-10 [185] and decrease in galectin-3, a marker of chronic inflammation and CVD risk [186]. A pilot study of 12 seropositive RA patients concluded that exercise induced improvements in the cardiorespiratory fitness and molecular markers of skeletal muscle oxidative metabolism were associated with changes in T cell metabolism which raises the question of whether exercise training, possibly through adaptations in skeletal muscle, can improve immune dysfunction [187].
In RA patients, moderate intensity exercise protocols ranging from 2 to 96 weeks are adopted for clinical safety for strengthening [i.e., 50–70% one repetition maximum: (1 RM)] and aerobic training [i.e., 50–70% maximum heart rate (HRmax) or peak oxygen (VO2max) uptake]. However, there are many studies showing that high intensity strengthening (i.e., 1 RM ≥ 70%) and aerobic (i.e., HRmax or VO2max ≥ 70%) exercises are also effective for RA patients without having any reported exercise related side effects [182, 188–193].
In summary, exercise training is essential for RA patients and has been proven to improve cardiorespiratory fitness. Exercise therapies should be seen as a “window of opportunity” for the early management of RA [194].
CV comorbidities cause serious morbidity and mortality in RA patients. Besides many different proposed mechanisms, systemic inflammation is the most implicated. Even nowadays, both the increased prevalence of traditional and disease specific CV risk factors are still not questioned sufficiently among physicians and remains overlooked.
Keeping the systemic inflammation under control and regular screening for CV risk factors are needed to minimize the risk of CV events. Better recognition of symptoms suggestive of CAD in RA patients, control of risk factors, early referral to a cardiologist and multidisciplinary management provides a chance to improve life quality and disease outcome. It should also be noted that CV events in RA patients may be more silent and severe than in the normal population.
Pathogenesis of synovial and vascular inflammation shows similar immune abnormalities. Thus, common target treatment modalities like T-cell directed and anti-cytokine therapies are used in both RA and CVD. Conventional and biological DMARDs appear to reduce the CV incidence successfully by suppressing systemic inflammation, but they may have potential adverse metabolic affects. Whereas, the use of NSAIDs and glucocorticoids may be a risk factor on their own. The net effect of RA therapies on CV risk may differ by patient characteristics. Despite aggressive RA therapy, individuals with uncontrolled disease activity should be evaluated for the use of cardio-protective agents.
There are still many questions in the pathogenesis of CVD in RA waiting to be clarified. In the future, with the understanding of these, it is hoped that more concrete guidelines will be available for CVD in RA patients in terms of risk assessment tools, biomarkers, prevention and treatment strategies.
ACPA: anti-citrullinated protein antibody
AF: atrial fibrillation
ASA: acetylsalicylic acid
BMI: body mass index
CAD: coronary artery disease
COX-2: cyclooxygenase-2
CRP: C-reactive protein
CT: computed tomography
CV: cardiovascular
CVCs: cardiovascular comorbidities
CVD: cardiovascular disease
DMARDs: disease-modifying anti-rheumatic drugs
ECG: echocardiography
GRK2: G protein coupled receptor kinase-2
HDL: high-density lipoprotein
HF: heart failure
HLA-DRB1: human leukocyte antigen-DR isotype1
HT: hypertension
IL-1β: interleukin-1β
LDL: low-density lipoprotein
MI: myocardial infarction
MTX: methotrexate
NSAID: non-steroidal anti-inflammatory drug
RA: rheumatoid arthritis
RF: rheumatoid factor
SCORE2-OP: systemic coronary risk evaluation-older persons
TNF-α: tumor necrosis factor-alpha
VO2: oxygen consumption
UÖ, NK, and MG: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. NT and MB: Validation, Writing—review & editing, Supervision. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2023.
Copyright: © The Author(s) 2023. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Gloria Candelas Rodríguez, Virginia Villaverde
Manolya Ilhanli, Ilker Ilhanli
Ozlem Pala ... Joel M. Kremer
Diego Benavent, Chamaida Plasencia-Rodríguez
Zehra Irshad, Nicola J. Gullick