 Original Article
Original Article

Affiliation:
1Department of Statistics, University of Manitoba, Winnipeg, Manitoba R3T 2N2, Canada
Email: harshani.desilva@umanitoba.ca
ORCID: https://orcid.org/0009-0001-6719-8379
Affiliation:
2Raksha Health Care, Haveri 581110, Karnataka, India
Affiliation:
3SDM College of Physiotherapy, Shree Dharmasthala Manjunatheshwara University, Dharwad 580009, Karnataka, India
ORCID: https://orcid.org/0000-0001-7186-0532
Affiliation:
4Department of Physical Therapy, College of Rehabilitation Sciences, University of Manitoba, Winnipeg, Manitoba R3E 0T6, Canada
ORCID: https://orcid.org/0000-0002-1450-0693
Affiliation:
5Department of Mechanical Engineering, University of Manitoba, Winnipeg, Manitoba R3T 5V6, Canada
ORCID: https://orcid.org/0000-0002-6384-8776
Affiliation:
1Department of Statistics, University of Manitoba, Winnipeg, Manitoba R3T 2N2, Canada
ORCID: https://orcid.org/0000-0001-8942-5352
Explor Digit Health Technol. 2026;4:101195 DOI: https://doi.org/10.37349/edht.2026.101195
Received: November 17, 2025 Accepted: March 18, 2026 Published: June 16, 2026
Academic Editor: J. G. Manjunatha, Mangalore University, India
Aim: Cerebral palsy (CP) is one of the most common motor neurodevelopmental disorders, affecting approximately three in every thousand live births in North America. The study aims to investigate and identify the factors influencing manual dexterity performance among children with CP and typically developing (TD) children according to the Manual Ability Classification System (MACS) levels.
Methods: A total of 100 children aged 4 to 12 years were enrolled, including 50 diagnosed with CP and 50 TD children. Manual dexterity performance was assessed across MACS levels. A Bayesian seemingly unrelated regression (BayesSUR) framework was applied to identify influential factors, explicitly accounting for interrelationships among multiple response variables. This probabilistic approach allowed for robust estimation under uncertainty while incorporating correlations across outcomes.
Results: The BayesSUR analysis revealed distinct factor influences MACS levels. For children with mild CP (MACS level 1), object type had the strongest effect on response time. For moderately affected children (MACS level 2), direction most strongly influenced movement error, while age impacted both error and success rate. Among severely affected children (MACS level 3) and TD children, gender emerged as the dominant factor influencing response time. However, the low inclusion probabilities of other factors suggest that additional data and validation are warranted.
Conclusions: The findings highlight the importance of considering both individual characteristics and task-specific factors when designing interventions to improve manual dexterity in children with CP. These results contribute to a better understanding of the key determinants influencing motor performance and may guide the development of more effective therapeutic and rehabilitation strategies. The Trial Registration Number: CTRI/2018/07/014900.
Canada and India face a growing population of children with cerebral palsy (CP), with the condition occurring in 2 to 4 of every 1,000 live births in North America and India, respectively [1]. Children with CP often have deficits in the performance of manual dexterity [2]. This deficit is clinically significant, as functional hand use is a strong determinant of a child’s autonomy in daily living, as well as their ability to successfully integrate into educational and social environments [3].
Because it is difficult to engage young children with CP in repetitive, long-term exercise programs, there is a need for effective approaches that motivate children to participate in clinical and, importantly, home exercise programs. One emerging way to keep children interested in therapy is to use computer games that require specific physical movements. These interactive challenges help children perform necessary but repetitive motor activities without getting bored. As a result of this approach, developers have created specialized systems known as computer game rehabilitation (CGR) platforms. Studies indicate that these games effectively improve motor skills and daily participation. To maximize their impact, these programs should be extended to home-based care, particularly for rural communities. Through the use of appropriate telemonitoring technology, clinicians can facilitate this remote rehabilitation, provide ongoing virtual support, and manage the long-term progression of personalized exercise regimens [4].
A game-based assessment neurofunction software application is a critical feature embedded into the CGR. It produces standardized computer-generated tasks with choices to guide and elicit goal-directed movement responses. The software automatically records a child’s choices and movements for each game task by using advanced data logging methods. Electronic outcome measures derived from the automated assessment tool can inform a therapist when and how a child is performing, whether they are experiencing any difficulty, and how they are progressing in their home exercise program. In this manner, parents or children will be able to interact with their therapists through a number of mechanisms: e-mail, telephone, and other methods, and thus obtain timely support regularly.
The computerized upper extremity (CUE) system was engineered to provide a quantitative analysis of object manipulation capabilities. The CUE assessment software automatically logs the client’s movement response to each game event and computes various performance-based metrics such as success rate, movement error, response time, and proportion of valid traces, and averages over several game events (i.e., 30 game movement responses in one minute of gameplay). Thus, the CUE assessment tool can provide objective, performance-based outcome measures for a broad range of goal-oriented object manipulation tasks for children with impairments of the upper extremity (UE).
Various tests and rating scales are available to assess the function of the UE in children with CP. For example, the Jebson-Taylor test measures UE function by the time taken to complete several tasks, with up to 100 seconds allowed to complete each task. Similarly, several pegboard tests have been developed, such as the Purdue Pegboard Test, 9-Hole Silverman Hand Function Test, and the Functional Dexterity Test [5]. These various pegboard tests are also graded by the time taken to complete them. However, time measurements alone have limited value. Other important performance metrics include movement quality, accuracy, and variation, as well as types of movement errors [6].
A number of assessment tools utilize therapists ‘and/or parents’ observation of task completion by a child for rating performance. For example, Peabody Developmental Motor Scale version-2 evaluates activities such as drawing, paper cutting, and the use of cubes and pellets in play activities, etc [7, 8]. Another test commonly used for UE assessment is the quality of upper extremity skills test (QUEST), which examines both the range of motion and grasp used in handling and manipulating three objects: a cube, a crayon, and a pellet [9]. Both these tests use composite scores that do not provide detailed information on object manipulation task performance. In addition, the above-mentioned assessments are limited to a narrow range of objects and tasks such as blocks, balls, pegs, coins, pens, and cans.
The CUE assessment tool offers distinct advantages over the previously discussed methods. Through its interactive software, the system employs standardized activities, specific time constraints, and analytical procedures to objectively quantify motor performance metrics. A key feature of the tool is its versatility; by attaching the miniature sensor with Velcro, the system can transform hundreds of objects varying in mass, shape, size, and surface friction into functional input devices. This adaptability allows clinicians to select objects that require specific prehension patterns, such as two-finger, three-finger, or bimanual grips, as well as distinct movements of the wrist, elbow, and shoulder. Consequently, a detailed understanding of an object’s physical and functional characteristics enables clinicians to establish precise therapeutic goals and objectively monitor patient progression.
It is essential to establish the psychometric robustness of digital technologies as they continue to emerge as therapeutic and assessment tools. A key aspect of this is known group validity, a critical psychometric property that determines whether the CUE can distinguish between groups with different levels of motor impairments. Confirming this property provides necessary insights into the tool’s capacity to detect clinically significant differences, a prerequisite for its application in diverse populations. Kanitkar et al. [10] examined a computer game-based upper extremity (CUE) assessment tool for children with CP and reported good test-retest reliability but weak associations with conventional measures, indicating that the CUE tool captures distinct components of manual dexterity.
Consequently, this study sought to identify the factors influencing manual dexterity performance among children with CP and typically developing (TD) children according to the Manual Ability Classification System (MACS) levels.
The primary objective of this study was to evaluate how factors such as age group, gender, direction of movement, game difficulty level, and the type of object used in the game influence game performance, including success rate, movement error, and response time across different MACS levels.
The MACS aims to classify how children with CP use their hands when handling objects in their daily activities, and the impact that these environmental and personal activities may have on the children’s performance. MACS levels are based on children’s ability to initiate handling objects by themselves and their need for assistance or adaptation to perform manual daily life activities that are appropriate for their age [11]. The MACS distinguishes between participants as follows: level 1 (mildly affected), level 2 (moderately affected), and level 3 (severely affected). To assess the influence of each factor on performance metrics individually, a frequentist analysis of variance (ANOVA) could be used. However, there is a strong correlation between success rate and movement error. Given the interdependencies among these performance metrics, a multivariate analytical approach is more appropriate. Therefore, we employed the seemingly unrelated regression (SUR) method, a high-dimensional, multiple-response regression framework, to examine how each factor affects game performance separately for each MACS level.
Our sample consisted of 15 mildly affected, 20 moderately affected, 15 severely affected, and 50 TD children. Recognizing that smaller sample sizes can challenge statistical reliability and increase variability, we implemented a Bayesian framework. Bayesian methods generally outperform traditional approaches with limited samples by accounting for uncertainty in parameter estimation and leveraging prior information. Unlike frequentist methods, which treat parameters as fixed, Bayesian statistics accommodate parameter variability over time and across conditions, enhancing flexibility and robustness particularly in studies like ours where sample sizes are constrained [12].
Fifty children with a diagnosis of CP and fifty healthy, TD children between the ages of 4 and 12 were enrolled in the study. Children from both groups performed an identical object manipulation task while they were seated at a desk to play the CUE assessment game. The children were allowed to play the CUE assessment game with a standard optical mouse until they became familiar with the game activities [10]. During the assessment, participants were comfortably seated at a table with an adjustable height. The four test objects were placed on the table at a comfortable reaching distance within arm’s length of the children [10].
Figure 1 represents the illustration of the game considered in this study. The CUE assessment software was used to guide object manipulation tasks. The software presents a target object appearing at random locations at the top of the display. It moves to the bottom of the display within two seconds and then disappears. One game event is defined as the time between the appearance of a target and its disappearance. The children handle and move each test object [i.e., rotate the inertial-based (IB) mouse] to move the game paddle and catch the moving target objects [10].

Screenshot of the game interface used in the CUE assessment software, developed and provided by author Prof. Tony Szturm. CUE: computerized upper extremity.
The CUE assessment tool uses a wireless IB mouse (Scoop™ Pointer Remote Model: RXR1000-0302E, Hillcrest Labs, United States) which links physical movements with interactive computer games [13]. The IB mouse contains a multi-axis gyroscope that detects instantaneous angular velocity. Internal mouse firmware filters and integrates the instantaneous velocity signal to produce the instantaneous angular position. This angular position signal is a rotation of the mouse in the air, which is slaved to the motion of a computer cursor or game paddle. The precision and responsiveness of the IB mouse are equivalent to those of a standard optical computer mouse. Therefore, the natural motion of an instrumented object can be used to control the motion of the computer game paddle [13].
The IB mouse features a plug-and-play design that allows any object to function as a mouse once the device is attached via Velcro, as shown in Figure 2. This setup enables users to guide on-screen elements, such as a cursor or game paddle, by manipulating the object naturally. The mouse can be mounted on objects of varying sizes, shapes, and weights ranging from toys to utensils as detailed in Figure 2. In this study, four test objects with different physical properties and anatomical demands were instrumented with the IB mouse [10].
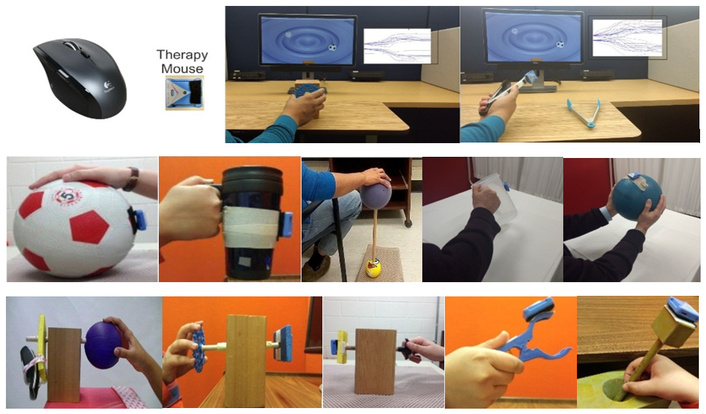
The IB mouse and different object types. Reproduced from Parmar et al. [13]. © 2021 by the authors. Distributed under the terms of the CC BY 4.0 license.
In this study, there are 5 factors that have been considered, and Table 1 illustrates the description of factors in the dataset.
Description of the factors considered in this study.
| Factor | Levels/Description |
|---|---|
| Direction | 1-Rightward, 2-Leftward |
| Object type | 1-Cone, 2-Fork, 3-Plastic ring, 4-Tennis ball |
| Age | 1-(4–6) years, 2-(6–12) years |
| Gender | 1-Male, 2-Female |
| Game difficulty level | 1-Target only, 2-Target + Distractor |
The four objects used for this study were a fork, a ring, a tennis ball, and a cone which differ in the type of grasp and functional demand. The fork was held in a tripod grasp in a mid-prone position performing wrist flexion and extension, the ring was in a cylindrical grasp performing radio-ulnar deviation, the tennis ball was held with fingers performing fine finger movements, and the cone was also held in a cylindrical grasp performing supination and pronation [10].
Three performance-based outcome measures were quantified in the present study: the success rate of each game event, total movement error and movement response time, which are represented in Table 2.
Description of Performance Metrics Quantified from the CUE Assessment Tool.
| Performance measure | Description |
|---|---|
| Success rate | The percentage of objects the player managed to catch out of the total number available in a session |
| Movement error | The distance between the paddle and the target at the moment the target disappears. If the player successfully catches the target, the error is recorded as zero. |
| Movement response time | This refers to the reaction speed, specifically the number of milliseconds that pass between the target appearing and the player physically starting to move the paddle. |
The selected metrics capture diverse characteristics of the recorded signals and the underlying cognitive processes. Specifically, they quantify task success, the speed of cognitive processing and motor planning, spatial accuracy, and the consistency of movement across repeated trials. For this experiment, the game session lasted 60 seconds with individual events occurring every 2 seconds. This protocol yielded a total of 30 movement samples for analysis, distributed evenly with 15 movements in each direction. In this case, the success rate is based on 30 game movement responses, and movement onset, movement error, and movement variation are the averages of 5 movement responses in each direction [10]. This study was undertaken to identify the significant impact of factors such as object type, direction, gender, game difficulty level, and age of children on performance metrics, which are movement error, response time, and success rate of the computerized game, considering the MACS levels [11].
Parents of all study participants provided informed consent. Children with a diagnosis of CP were recruited from S.D.M. Hospital, Dharwad, and Ushas’ School for Exceptional Children, Hubli. TD children were recruited from an elementary and middle school in Gadag, India.
Inclusion criteria of children diagnosed with CP included:
MACS level I–III [11].
Modified Ashworth scale was used to determine the level of spasticity in biceps brachialis, pronator quadratus, and finger flexors, from grade 1 to 1+ [14].
Pediatric version of the mini-mental state exam for children (MMC) score above 17.
TD children were based on the pre and post-natal history obtained from parents. Exclusion criteria included:
Visual or auditory impairment or a communication disorder that would prevent a child from being able to follow instructions, comprehend computer games, or see the computer game targets/paddle [10].
Recent orthopedic impairment or botulinum toxin injection to the UE within the last six months.
History of convulsion disorder within the last six months.
The Bayesian framework offers a probabilistic approach to learning from data. Bayesian and frequentist statistics offer fundamentally different interpretations of model parameters [12]. In the frequentist approach, parameters are treated as fixed values within the population. Probability is viewed through the lens of repeated sampling, and significance testing relies on a counterfactual assumption, specifically, how a test statistic would behave if the null hypothesis were true [15]. In contrast, in the Bayesian approach, parameters are treated as uncertain and are described using probability distributions. This method utilizes a “prior distribution” (formulated before data collection), which is then updated with observed data to create a “posterior distribution” [16].
While the frequentist approach is generally based on the likelihood, the Bayesian approach prescribes how priors are updated with the likelihood to yield a posterior probability distribution.
Where, P(β|data)—posterior, P(β)—prior, and L(data|β)—likelihood.
The posterior distribution characterizes the researcher’s uncertainty about the parameter after the data are observed. It takes a central place in the Bayesian approach and serves as the basis for inferences and tests of hypotheses. Bayesian Inference is performed using Markov Chain Monte Carlo (MCMC) methods when the posterior distribution is complicated and high-dimensional [16].
The Bayesian framework is often favored for its adaptability, particularly its capacity to integrate pre-existing knowledge and refine predictions as fresh data is acquired. Furthermore, it offers a more intuitive interpretation of probability compared to other methods. However, a significant limitation is the necessity of defining prior distributions. This requirement can introduce an element of subjectivity that may ultimately affect the analytical outcomes.
Before observing any data, beliefs or knowledge about the parameters of interest are represented by a prior distribution. The prior distribution incorporates existing information or beliefs, and it can be subjective or based on previous data or expert opinions [16].
The likelihood function describes the probability of observing the data given the parameters [16]. It quantifies how well different parameter values explain the observed data, assuming the model is true.
The posterior distribution represents the updated beliefs about the parameters after taking into account the observed data. It is obtained by combining the prior distribution and the likelihood function using Bayes’ theorem [16]. The posterior distribution summarizes the uncertainty in the parameters given in the data.
Bayesian inference involves summarizing the posterior distribution to make inferences about the parameters or to perform hypothesis testing. This can be done by calculating point estimates such as the posterior mean or median, or by constructing credible intervals that contain a specified proportion of the posterior distribution [16]. Bayesian inference allows for a direct interpretation of probabilities, such as the probability that a parameter falls within a specific range.
Bayesian SUR (BayesSUR) is an approach for estimating a system of regression equations where the error terms across different equations are correlated [17]. This framework allows for robust parameter estimation and uncertainty assessment, particularly when outcomes are interdependent. We employed a BayesSUR framework to identify the determinants of manual dexterity in children with CP and TD children.
The SUR approach acknowledges that while the equations for different motor outcomes may appear independent, their error terms are correlated [18]. By analyzing these outcomes simultaneously, the model gains statistical power and provides a more accurate estimation of how factors such as age, gender, and object type influence performance across different MACS levels. A core advantage of the BayesSUR framework is its ability to perform automated variable selection. In this study, we utilized marginal inclusion probability (MIP) to quantify the importance of each predictor [19]. MIP represents the probability that a specific factor is truly influential in the model. A high MIP suggests a robust relationship between the factor and the motor outcome, even when accounting for the uncertainty present in clinical neurodevelopmental data.
The model was implemented using the BayesSUR package in R, which utilizes MCMC algorithms to estimate the posterior distributions of the parameters. This framework is particularly effective for high-dimensional clinical data, as it is designed to perform automated variable selection. By prioritizing predictors with the highest MIPs, this method effectively identifies the most influential factors, such as age, gender, or object type, while mitigating the risk of noise or overfitting. A comprehensive description of the mathematical derivations and prior specifications is provided in the Supplementary material.
Exploratory data analysis has been conducted to identify the variation in manual dexterity performances between children with CP and TD children. The study considered three measurements: success rate, movement error, and response time.
Figure 3 represents the variation of success rate, movement error, and response time among children with CP and TD children. It indicates that TD children have a higher success rate in the game and less movement error compared to children with CP. Moreover, it depicts that most children, both children with CP and TD children, demonstrate similar performance on the response time. However, a smaller subset of children with CP exhibits longer response times compared to the TD children.
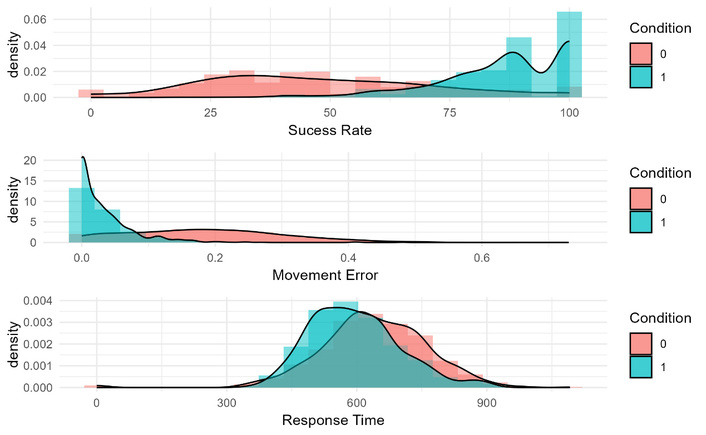
Variation of success rate, movement error, and response time among children with CP and typically developing children. 0—children with CP; 1—typically developing children. CP: cerebral palsy; MACS: Manual Ability Classification System.
Figure 4 illustrates the variation of success rate, movement error, and response time observed in both children with CP and TD children according to the MACS levels. As depicted in Figure 4, we observe clear differences between TD children and those at all MACS levels. TD children show higher success rates and lower movement errors compared to children with any level of impairment. However, when comparing the different MACS levels with each other in terms of success rate and movement error, there are no substantial differences, and the distributions across the MACS levels appear similar, with no noticeable changes. For response time, we observe that children who are severely affected (MACS level 3) have lower density values compared to other groups and generally exhibit higher response times in regions of higher density.
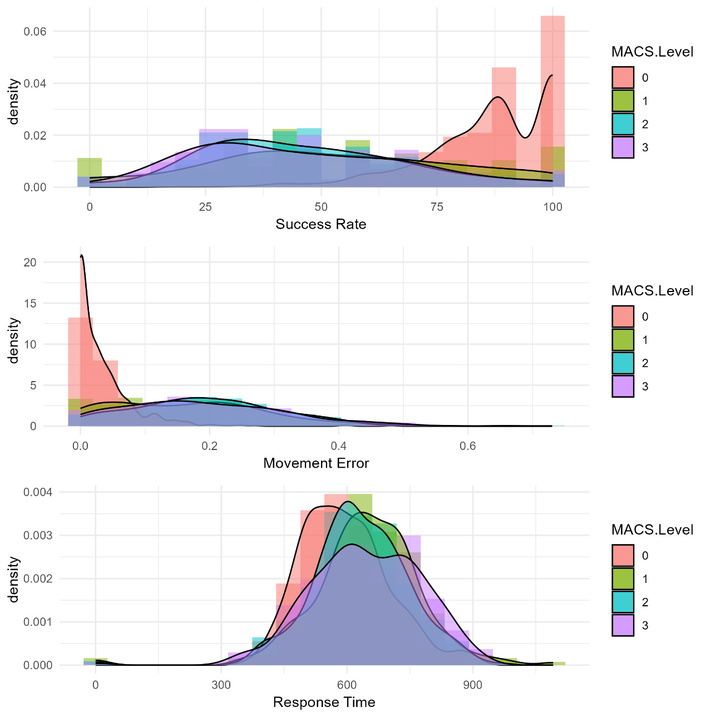
Variation of success rate, movement error, and response time among children according to the MACS levels. 0—Typically developing children; 1—mildly affected children with CP; 2—moderately affected children with CP; 3—severely affected children with CP.
The BayesSUR approach was applied to identify the factors influencing manual dexterity performance metrics through a variable selection procedure. The study examined five factors: direction of the movement, object type, age group, game difficulty level, and gender. Several performance measures were considered, including success rate, movement error, and movement response time. Importantly, the analysis accounted for both the CP sample (children with CP) and the TD sample (typically developing children) during the assessment process.
Children were classified according to the MACS, which categorizes manual ability in children with CP and TD children. MACS level 0 represents TD children, while levels 1, 2, and 3 indicate increasing severity of CP (mild, moderate, and severe, respectively). To identify factors influencing manual dexterity performance, we conducted separate analyses for each MACS level. This approach allowed us to investigate how these factors affected performance across the spectrum of manual ability.
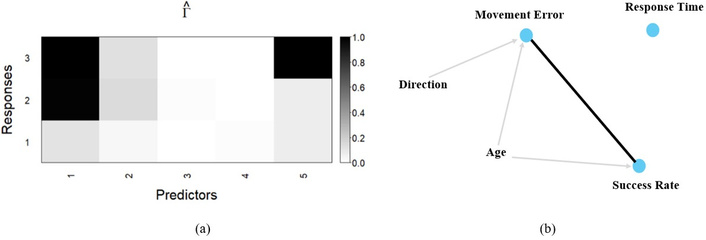
Figure 5 represents the results of the BayesSUR analysis for children classified as MACS level 1 (mildly affected CP). The first panel shows the variable inclusion probability. Rows correspond to the performance measures: 1—response time, 2—success rate, 3—movement error. Columns represent the predictor variables: 1—age, 2—gender, 3—game difficulty level, 4—object type, 5—direction. Color intensity indicates variable inclusion probability, with darker shades representing a higher probability of a variable being included in the model for that specific performance measure. The second panel depicts the network structure of the BayesSUR model. Nodes represent variables, and edges connect variables that are likely to be related based on the model. The thickness of the edges reflects the strength of the connections.
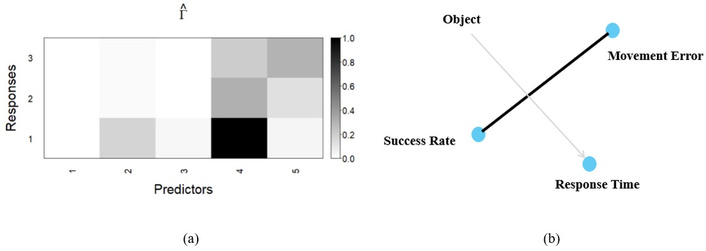
Results of BayesSUR model for mildly affected CP children. Panel (a): Variable inclusion probability (
The BayesSUR analysis (Figure 5) suggests that for children with mild CP (MACS level 1), object type has the strongest influence on response time among the factors considered. Other factors, including age, gender, game difficulty level, and direction, appear to have little to no influence on any of the performance measures (response time, success rate, movement error) based on their low inclusion probabilities in the model. This finding implies that for mildly affected children, the type of object they manipulate during the game might be a key factor affecting how quickly they respond.
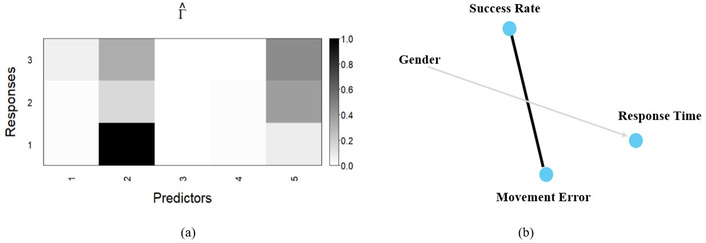
Figure 6 presents the results for children with moderate CP (MACS level 2). The analysis suggests that direction has the strongest influence on movement error. Additionally, age appears to influence both movement error and success rate. Other factors, including gender, game difficulty level, and object type, seem to have minimal influence on performance measures based on their low inclusion probabilities in the model. These findings indicate that for moderately affected children, the direction of movement (rightward or leftward) might be a crucial factor affecting how many errors they make. Furthermore, age seems to play a role in both movement accuracy (error rate) and successful task completion (success rate).
Results of BayesSUR model for moderately affected CP children. Panel (a): Variable inclusion probability (
Figure 7 shows the results for children with severe CP (MACS level 3). The analysis suggests that gender has the strongest influence on response time. All other factors, including age, game difficulty level, object type, and direction, appear to have no influence on any performance measures (response time, success rate, movement error) based on their low inclusion probabilities in the model. According to the figure, we can conclude that for severely affected children, gender might be a key factor affecting their response time. This means their response time could potentially differ based on whether they are male or female.
Results of BayesSUR model for severely affected CP children. Panel (a): Variable inclusion probability (
Figure 8 depicts the BayesSUR findings for TD children. The analysis indicates that direction has the strongest influence on response time. Other factors, including age, gender, game difficulty level, and object type, seem to have minimal impact on any performance measures (response time, success rate, movement error) based on their low inclusion probabilities in the model. This suggests that for TD children, the direction of movement (rightward or leftward) might be a significant factor affecting how quickly they respond.
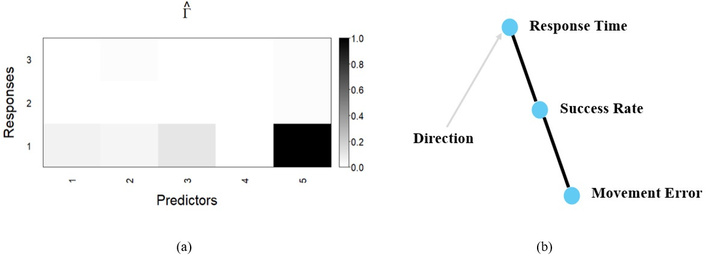
Results of BayesSUR model for TD children. Panel (a): Variable inclusion probability (
Methodological validity was established through the examination of diagnostic plots. The clear convergence of all chains indicated that the model stabilized, confirming the robustness of the reported findings. To further assess the predictive accuracy and stability of the model within each subgroup, we calculated the expected log pointwise predictive density (ELPD) using Leave-One-Out cross-validation (LOO-CV) and the Watanabe-Akaike information criterion (WAIC). Across all cohorts, the LOO and WAIC estimates showed near-perfect agreement. This consistency between predictive metrics provides objective evidence of model stability, confirming that the Bayesian framework effectively handled the varying sample sizes and preserved data integrity across the different functional levels.
Jaspers et al. [20] studied which three-dimensional spatiotemporal and kinematic parameters differentiate upper limb movement characteristics in children with hemiplegic CP (HCP) from those in TD children (TDC), during various clinically relevant tasks. They used 3 reach tasks, 2 reach-to-grasp tasks, and 3 gross motor tasks. The children were made to sit in a custom- made chair that was adjustable. Results showed that children with HCP had longer movement durations, fewer straight-hand trajectories, and lower maximum velocities compared to the TD children. The timing of maximum velocity did not differ between the two groups [20].
Butler et al. [21] in their study on Three-dimensional kinematics of the upper limb during a Reach and Grasp Cycle for children used light reflective markers on the upper limb at the specific bony landmarks. They placed a cylindrical cup at a distance of 75% of the child’s maximum reach. The 3-dimensional marker data was recorded using an 8-camera optoelectric motion analysis system. They found that there was a significant correlation between age and joint position at the point of task achievement for 3 of the 40 kinematic measures during the Reach and Grasp Cycle. Younger children had less elbow flexion and less wrist radial deviation. The utility of the Reach and Grasp Cycle was demonstrated by the consistent kinematic patterns that emerged among the TD children, as well as the clinically significant differences in joint motion that arose between the children with CP and the TD children. The reach and grasp cycle provides a quantitative analysis of motor deficits during a functional task. The study on UE using computer adaptive testing was done, which was parent-reported; this testing balances the greater ease in the burden of administration of the different scales. However, it does not measure the hand function of the child by observing or evaluating the performance, and only measures the questionnaire in the objective form, which is reported by the parents, measuring parent-reported outcomes [22].
In the above studies, the psychometric properties are movement durations, straight-hand trajectories, and maximum velocity profiles. In the present study, we have used this neuro-functional evaluation software, which gave us the outcome in the form of success rate, response time, and movement error, which are lacking in the above-mentioned tools. In the above-mentioned articles, there is a lack of variety of objects used and also variation of movement; this aspect is covered in the present study by using different objects and different movement variations.
Moreover, unlike traditional assessments such as the Jebson Taylor, Purdue Pegboard, or Functional Dexterity Test, which rely primarily on time-to-completion, the CUE system captures multi-dimensional movement quality. Observational scales like the PDMS-2 and QUEST often use broad 4–5-point composite scores that do not provide information on specific object manipulation. In contrast, the CUE tool quantifies onset time and movement error for specific tasks. While commercial systems like the WII or Kinect detect gross limb motion, they lack the sensorimotor processing of skin tactile information regarding object stability and slip, which is a key advantage of the CUE system.
This study aimed to investigate and identify the various factors that have an impact on the manual dexterity performance matrix among children with CP and TD children according to the MACS levels. To achieve this, the study utilized advanced neurofunctional evaluation software, which was mentioned above, to assess and analyze the manual dexterity performance of the children. By gaining insights into the influencing factors, this research aimed to contribute to the development of effective interventions and strategies that can optimize the manual dexterity skills of children with CP, ultimately improving their quality of life and functional outcomes.
In this study, we employed the BayesSUR method to identify the influential factors affecting the manual dexterity performance matrix. This method allowed us to consider the response variables collectively, taking into account their interrelationships and dependencies. By utilizing BayesSUR, we aimed to comprehensively analyze the factors and their joint influence on the performance matrix, capturing the combined effects across multiple response variables. SUR is a method that treats each response variable as a separate regression equation and assumes that the error terms for each equation are uncorrelated but allows for heteroscedasticity and different error variances across equations.
The results of this study suggest that the key to progress changes depending on a child’s functional level. Our model shows that clinicians should prioritize different therapeutic targets for each MACS category. For children with mild impairment (MACS I), the physical features of the Object being handled are the most important factor, specifically affecting their Response Time. Because these children already have a high level of function, they are sensitive to the challenge of the tool itself. Clinically, this means that for high-functioning children, therapy should focus on increasing variety in object shapes, sizes, and textures to help sharpen their motor planning speed. As impairment increases to the moderate level (MACS II), the focus shifts from the object to Age and Direction. In this group, age is the primary factor of both the overall Success Rate and Movement Error. Younger children in this category show significantly more difficulty with accuracy than older children, even when performing the same task. Furthermore, the direction of movement is a major barrier to accuracy. For these children, clinicians should prioritize spatial reaching exercises while recognizing that younger children will need much more environmental support and adaptation to achieve the same results as the older children. In the most severely affected group (MACS III), the factors become less distinct, but Gender emerges as a notable influence on Response Time. While therapy for this group remains focused on basic functional engagement, clinicians should be aware that biological factors like gender may influence the speed of motor initiation. Finally, our observations of TD children showed that the direction of movement was the primary factor influencing their response speed. This suggests that even in a healthy motor system, spatial planning remains a significant challenge. However, due to the low inclusion probabilities of other factors in these models, further investigation is needed to confirm these findings and explore potential underlying reasons. Overall, the results emphasize the importance of considering individual characteristics (MACS level, gender) and task-specific factors (object type, direction) when designing interventions to improve manual dexterity in children.
The interpretation of our results requires caution due to certain limitations regarding confounding variables and study design. First, regarding subject characteristics, the study focused on five specific factors (direction, object type, age, gender, and game difficulty) but overlooked other potential confounders that could bias results. Specifically, the influence of comorbidities, previous rehabilitation history, and varying levels of cognitive ability was not analyzed. Furthermore, the exclusion of children at MACS levels IV and V was a necessary limitation of the study design, as children at these functional levels lack the minimum motor threshold required to initiate or perform object manipulation tasks. At these levels, the success rate would consistently be zero according to the assessment protocol, making the CUE tool inappropriate for this specific subgroup. Moreover, physical limitations such as the severity of spasticity, visual impairments, and sensory deficits were not controlled for, despite their potential impact on CUE performance. Second, environmental factors, such as the level of family support, were not included. Finally, the generalizability of the results is limited by the single-center source of the sample and the cross-sectional nature of the data. This limitation to external validity is significant, as the findings specifically characterize children with mild-to-moderate CP and may not generalize to those with the most severe impairments or to non-digital clinical settings. To address these limitations and enhance statistical robustness, future research will incorporate a larger dataset. Additionally, studies should employ a longitudinal design across multiple centers to better account for these unmeasured confounders.
Moreover, this study benefits from further exploration using a non-parametric Bayesian approach. Non-parametric Bayesian methods offer an alternative way to analyze the data without making assumptions about the underlying distribution or functional form of the variables. This additional investigation can provide valuable insights and strengthen the validity of the results, ensuring a comprehensive understanding of the influential factors on manual dexterity performance in children with CP.
BayesSUR: Bayesian seemingly unrelated regression
CGR: computer game rehabilitation
CP: cerebral palsy
CUE: computerized upper extremity
HCP: hemiplegic cerebral palsy
IB: inertial-based
LOO-CV: Leave-One-Out cross-validation
MACS: Manual Ability Classification System
MIP: marginal inclusion probability
QUEST: quality of upper extremity skills test
SUR: seemingly unrelated regression
TD: typically developing
WAIC: Watanabe-Akaike information criterion
Detailed mathematical derivations of the Bayesian framework and prior probability distributions are available at: https://www.explorationpub.com/uploads/Article/file/101195_sup_1.pdf.
HDS: Conceptualization, Data curation, Formal analysis, Software, Validation, Visualization, Writing—original draft, Writing—review & editing. SM: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Writing—review & editing. TS: Investigation, Resources, Software, Validation, Writing—review & editing. NS: Investigation, Software, Validation, Writing—review & editing. SP: Investigation, Funding acquisition, Resources, Writing—review & editing. SBH: Investigation, Resources. All authors reviewed and approved the submitted version.
The authors declare that they have no conflicts of interest.
Ethical approval for the study was obtained from the Institutional Ethical Committee of S.D.M. College of Medical Sciences and Hospital, Dharwad (Ref: SDMIEC:091:2018; dated 23-03-2018). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki (2013 revision), and this trial was prospectively registered with the Clinical Trials Registry - India (CTRI) under the registration number: CTRI/2018/07/014900.
Parents of all study participants provided informed consent.
Not applicable.
Data used in this paper is available from the first author upon request.
This research has been partially supported by Dr. Muthukumarana’s (Grant Number: RGPIN-2024-05460) and Dr. Sepehri’s (Grant Number: RGPIN-2018-05352) Natural Sciences and Engineering Research Council of Canada (NSERC) Discovery grant. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 426
Download: 28
Times Cited: 0
