Mini Review
Mini Review

Affiliation:
Department of Surgical Oncology, Max Hospital, Gurugram 122002, Haryana, India
Email: Kaushalyadavoo7@yahoo.com
ORCID: https://orcid.org/0000-0002-2087-7585
Affiliation:
Department of Surgical Oncology, Max Hospital, Gurugram 122002, Haryana, India
Explor Dig Dis. 2025;4:100592 DOI: https://doi.org/10.37349/edd.2025.100592
Received: April 29, 2025 Accepted: August 19, 2025 Published: September 18, 2025
Academic Editor: Roberto Cirocchi, University of Perugia, Italy
The article belongs to the special issue Diverticulitis: Pathomechanism, Diagnosis and Treatment
This article evaluates contemporary and evolving surgical techniques in diverticulitis management. A comprehensive literature search was conducted using PubMed on guidelines for articles on surgical interventions for diverticulitis. The relevant data were extracted and synthesized to identify trends, advancements, and gaps in the current understanding of surgical interventions for diverticulitis. Many patients with uncomplicated diverticulitis can achieve favourable outcomes through conservative management strategies. Surgical interventions are increasingly tailored based on individual risk profiles and disease severity. Recent methods for managing diverticulitis highlight the significance of personalized treatment, which can lead to faster recovery times and better overall quality of life. More patients are now considered appropriate candidates for primary anastomosis, with or without a stoma in place of Hartmann’s procedure, where reversal is often tricky. Additionally, minimally invasive surgical techniques are being employed more frequently.
Diverticulitis, characterized by the inflammation of diverticula in the colon, has been a focal point in gastrointestinal research and surgical innovation. Recent advancements in surgical interventions reflect a paradigm shift towards less invasive techniques and individualized management strategies, which have significantly improved patient outcomes. The introduction of laparoscopic approaches for both diagnosis and treatment of complicated diverticulitis has demonstrated shorter hospital stays. Still, the choice of required surgery should not be influenced by the mode of access, whether laparoscopic or open [1]. Laparoscopic resection and anastomosis may be preferred in uncomplicated sigmoid diverticulitis requiring surgery [1]. For diverticulitis cases complicated by abscess, the emergence of percutaneous drainage of abscesses has allowed for a more conservative initial treatment, often facilitating a one-stage resection and anastomosis [2]. Research highlights the importance of customizing treatment plans for diverticulitis, indicating that many uncomplicated cases can be managed without hospitalization or antibiotics. As the medical field continues to examine the advantages of laparoscopic and robotic-assisted surgeries, the primary emphasis is placed on enhancing recovery times and reducing complications. This focus ultimately aims to improve patients’ quality of life.
Recent advances in the surgical management of diverticulitis have significantly improved patient outcomes and treatment strategies. One notable development is the laparoscopic approach, which has been introduced for the diagnosis and definitive treatment of uncomplicated diverticulitis [3]. Laparoscopic surgery offers several advantages over open surgery across various fields, including reduced blood loss during the procedure, shorter duration of the operation, a quicker recovery time in the hospital, and a decreased rate of postoperative complications [4]. Surgical outcomes remain the same between the laparoscopy and open groups [5]. The percutaneous drainage of the diverticulitis abscesses permits a less invasive therapeutic approach before definitive surgery and reduces the risk of a permanent stoma [2, 6]. After the successful drainage, a semi-elective resection is frequently conducted, while in some high-risk and limited disease cases, drainage alone may be therapeutic [6, 7]. Additionally, resection surgery has been identified as the optimal management for acutely complicated diverticular disease, demonstrating significant benefits such as reduced mortality, shorter hospital stays, and lower wound infection rates [8]. Overall, diverticulitis management now trends towards more effective, less invasive surgical options that improve recovery and reduce complications in patients suffering from diverticulitis.
Recent studies have indicated that many patients with uncomplicated diverticulitis can achieve favourable outcomes through conservative measures such as dietary modifications and symptom management without surgical intervention [9]. Advances in computed tomography (CT) reporting have facilitated better stratification of patients, allowing for tailored interventions based on individual risk profiles [10]. Colonic wall thickness > 15 mm and peridiverucular inflammation of grade 4 are significant predictive factors for recurrence and requirement of surgical interventions [11, 12]. Peridiverticular inflammation grade 4 has more chances of recurrence, while grades 1 and 2 have less, and colonic wall thickness of 18.5 mm is indicative of chances of recurrence within 90 days (Tables 1 and 2) [11, 12]. Along with imaging, C-reactive protein (CRP) is also advised to be included in laboratory evaluation, with CRP > 50 having prognostic value [13]. These findings, along with clinical parameters, help in identifying patients requiring surgical intervention.
Wall thickness grading on CT scan.
| Grade | Wall thickness on CT scan |
|---|---|
| 1 | < 1 cm |
| 2 | 1–1.5 cm |
| 3 | > 1.5–2 cm |
| 4 | > 2 cm |
CT scan grading of peridiverticular inflammation.
| Grade | CT peridiverticular inflammation |
|---|---|
| 1: Minimal | Rare fine threads of high attenuation |
| 2: Mild | Multiple threads of high attenuation that remain distinct, vessels are clearly visible |
| 3: Moderate | Many threads are difficult to resolve individually, and vessels are difficult to discern |
| 4: Severe | Dominant pattern of increased attenuation in the fat could be mistaken for fluid collection, vessels not visible |
Percutaneous drainage of diverticular abscess is a minimally invasive procedure that has become an essential component in managing complicated diverticulitis [14]. This technique involves the insertion of a catheter through the skin to drain the abscess. Ideal candidates typically present with a well-defined abscess that is accessible via imaging studies, such as ultrasound or CT scans. Hemodynamically stable patients, without signs of systemic infection or perforation, are preferred. Successful drainage can lead to significant symptom relief and may allow for conservative management of diverticulitis [13, 15]. Most guidelines suggest thresholds for percutaneous drainage of 3 cm [15].
Minimally invasive surgical (MIS) techniques for diverticulitis management have gained prominence due to their potential benefits over open surgery [16]. These techniques, including laparoscopic surgery, offer advantages such as reduced blood loss, less postoperative pain, and shorter hospital stays [16, 17]. While some studies reported improvement in mortality, others did not [16, 17]. Cochrane review concludes that evidence to support or refute laparoscopy over open is insufficient [18]. With advances in surgical techniques, MIS techniques are now well established in advanced colorectal surgery for malignant cases. Similarly, they are gaining evidence and acceptance in instances of complicated diverticulitis [19]. Robotic surgery has also shown fewer morbidity and shorter hospital stay with longer operative time and increased cost compared to laparoscopic and open approaches [20]. Patient selection for these procedures is crucial and depends on the severity of the disease, the patient’s overall health, and the presence of complications [21].
Laparoscopic surgery: This is the most studied minimally invasive technique, showing benefits like reduced complications and improved recovery times compared to open surgery [22, 23].
Laparoscopic peritoneal lavage: Gained popularity for the potential to avoid a stoma in Hinchey III [24]. However, the SCANDIV and Ladies/LOLA trials, along with a meta-analysis, found that laparoscopic lavage and drainage (LLD) are associated with a higher rate of peritonitis and reoperation [25, 26]. LLD should be used cautiously and in carefully selected patients [27].
Robotic surgery: Offers similar benefits to laparoscopic surgery, with some studies suggesting even greater reductions in morbidity [20]. Evidence at present to support superiority over laparoscopy is insufficient [28].
Severity of disease: Patients with Hinchey III/IV diverticulitis may be candidates for minimally invasive approaches if they are hemodynamically stable (Table 3) [9, 10].
Performance status of patient: Patients must be stable enough to undergo surgery, with considerations for factors like steroid use and blood supply to minimize risks such as anastomotic leaks [9].
Response to conservative management: Patients who do not respond to antibiotics or percutaneous drainage may require surgical intervention [9].
Hinchey classification of grades of diverticulitis.
| Hinchey grades | Findings |
|---|---|
| I | Pericolic abscess/phlegmon |
| II | Contained pelvic or retroperitoneal abscess |
| III | Generalized purulent peritonitis |
| IV | Fecal peritonitis |
Elective surgery: Recommended for patients with recurrent episodes or complications that do not resolve with conservative treatment [8, 21, 29].
Emergency surgery: Indicated in cases of perforation or failure of non-operative management, with minimally invasive techniques preferred when feasible [29, 30].
While minimally invasive techniques are increasingly favoured, the choice of procedure must be tailored to the individual patient’s condition and response to initial treatments [29]. The complexity of diverticulitis and the variability in patient presentations necessitate a careful, case-by-case approach to surgical decision-making.
The management of complicated diverticulitis has evolved with advancements in surgical techniques, offering a range of options from traditional open surgeries to modern minimally invasive approaches. Traditional surgical approaches include mainly:
Open colectomy: Historically, open colectomy has been a standard treatment for complicated diverticulitis, especially in cases involving perforation and peritonitis. It is often recommended for critically ill patients with multiple comorbidities, where the Hartmann procedure is preferred due to its safety in unstable conditions [1, 31, 32].
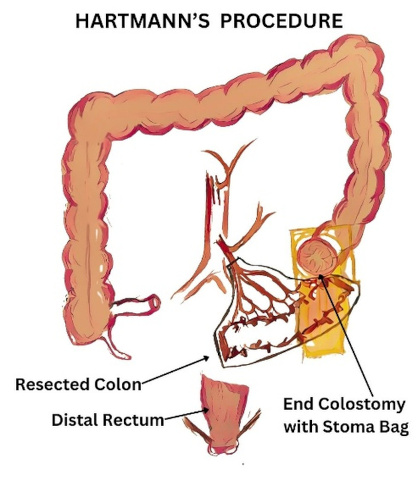
Hartmann procedure: This involves resection of the diseased colon segment with the creation of a colostomy, which is often irreversible, leading to a permanent stoma in many cases (Figure 1) [1, 21, 31].
Modern surgical options focus on early recovery, smaller incisions, and quicker healing while maintaining effective treatment outcomes.
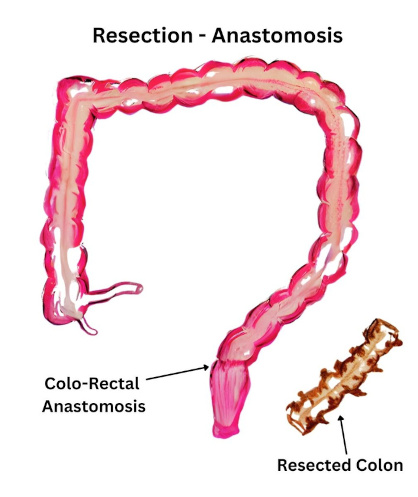
Primary anastomosis vs. Hartmann procedure: Primary anastomosis is favoured in stable patients as it avoids the need for a permanent stoma, which is often associated with the Hartmann procedure (Figure 2). Studies have shown that primary anastomosis can be safely performed in selected patients with perforated diverticulitis, with low rates of anastomotic leaks [21].
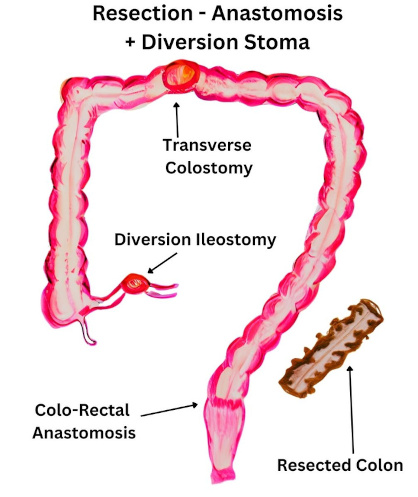
Primary anastomosis with diversion stoma: is considered a safer alternative in infected cases (Figure 3). With careful selection, more patients can be selected for primary resection anastomosis with diversion stoma, having a higher rate of reversal compared to Hartman’s procedure [21, 31].
Minimally invasive techniques: MIS approaches are now being utilized increasingly for complicated diverticulitis. These techniques, including laparoscopic surgery and robotic surgery, are preferred due to their potential benefits, such as reduced postoperative pain, minimized scarring, and shorter recovery times, which enable patients to resume normal activities more quickly [17]. The natural orifice intracorporeal anastomosis with specimen extraction (NICE) procedure, a robotic intracorporeal anastomosis, offers a minimally invasive option for complicated diverticulitis, reducing the need for abdominal incisions and potentially lowering conversion rates [32]. It should be viewed as an alternative to the transperitoneal approach in appropriately selected patients, although long-term safety needs to be proven by further studies.
Patient selection: The decision to perform primary anastomosis should be based on a thorough preoperative assessment, considering factors such as the patient’s comorbidities, the extent of intra-abdominal contamination, and the presence of sepsis or septic shock [21, 31].
While primary anastomosis with or without diversion stoma is increasingly preferred in suitable patients, the Hartmann procedure remains a viable option for those with severe comorbidities or hemodynamic instability [21].
Perforation and peritonitis: Surgery is often necessary for patients with perforation and generalized peritonitis. Options include resection with primary anastomosis or Hartmann’s procedure, depending on the patient’s stability and the extent of contamination [21, 27].
Abscess: Patients with diverticular abscesses may initially be managed with antibiotics and percutaneous drainage, but surgery is considered if these measures fail [21].
Fistula: Surgery for fistula resulting from diverticulitis involves surgical intervention to remove the diseased segment of the colon and repair the surrounding tissue, ensuring that healthy bowel continuity is restored while minimizing complications associated with the condition [33].
Obstruction: Surgical intervention is typically required for bowel obstruction due to diverticular disease, with resection being the preferred approach [13, 21, 31].
Recurrent diverticulitis: Elective surgery after two episodes of uncomplicated diverticulitis is now debated. Current guidelines suggest a more selective approach, reserving surgery for patients with complicated cases, rather than routine prophylactic colectomy [21, 29].
Quality of life and cost-effectiveness: Elective surgery may improve long-term quality of life and cost-effectiveness, but it is not recommended solely to prevent emergency colostomy or complications [21, 29, 31].
While surgical intervention remains crucial for cases of complicated diverticulitis, the trend is towards more conservative management where feasible in uncomplicated and Hinchey I & II cases. The decision to operate should be individualized, considering the patient’s overall health, disease severity, and personal preferences (Table 4).
Treatment selection criteria in diverticulitis.
| Surgical intervention | Ideal candidate | Less favoured condition |
|---|---|---|
| Percutaneous drainage | Localized diverticular abscess formation > 3 cm; patients who are critically ill or unsuitable for surgery. | Ineffective for extensive abscesses or diffuse peritonitis. |
| Open colectomy | Complicated diverticulitis with perforation and peritonitis; critically ill patients with multiple comorbidities. | Limited abscess, significant comorbidities; preference for minimally invasive techniques in stable patients. |
| Hartmann procedure | Severe comorbidities or hemodynamic instability; patients requiring a safe approach in complicated conditions. | Stable patients who can tolerate primary anastomosis; patients wishing to avoid a permanent stoma. |
| Primary anastomosis | Stable patients with perforated diverticulitis and low risk of anastomotic leaks. | Severe intra-abdominal contamination; presence of sepsis or septic shock. |
| Primary anastomosis with diversion stoma | Infected cases where restoration of bowel continuity is easier than Hartmann’s procedure. | Severe contamination and comorbidities in hemodynamically unstable patients. |
| Laparoscopic approach | Complications such as abscess formation, perforation, or obstruction; preference for reduced postoperative pain and quicker recovery. | Patients unsuitable for laparoscopic surgery due to comorbidities, extensive disease, or severe intra-abdominal contamination, and hemodynamically unstable patients. |
| Robot-assisted approach | Enhanced precision for complex procedures; suitable for patients requiring delicate dissection or suturing. | High cost; patients with contraindications for pneumoperitoneum or those with extensive contamination and hemodynamic instability. |
The future directions in diverticulitis surgery research are shaped by evolving understandings of the disease’s natural history and the effectiveness of less invasive management strategies.
Traditional guidelines recommended elective colectomy after recurrent diverticulitis episodes, especially in younger patients. However, recent evidence suggests that recurrence rates are lower than previously thought, prompting a re-evaluation of these indications [8, 9, 29, 34].
Minimal invasive surgical techniques like laparoscopy and robotic surgery require further strong evidence for general recommendation in emergency settings [18, 28, 35].
Endoscopic assessment of the colon can be performed to identify associated pathologies such as malignancy. Procedures such as colonoscopy stenting for diverticular strictures, controlling bleeding, and performing endoscopic ultrasound-guided abscess drainage are some of the described endoscopic techniques. These procedures should be used selectively, considering the potential complications, and their proper application requires further substantial evidence [36].
The landscape of surgical interventions for diverticulitis is shifting towards more effective, less invasive techniques that enhance patient recovery and quality of life. Minimally invasive strategies, like percutaneous drainage for abscesses, allow for a conservative approach in complicated cases while ensuring timely surgeries when needed. Minimally invasive strategies, like percutaneous drainage for abscesses, allow for a conservative approach in complicated cases while ensuring timely surgeries when required. Advancements in laparoscopic and robotic-assisted surgeries have led to improved outcomes, including reduced morbidity and shorter hospital stays. The focus on individualized treatment plans, guided by advanced imaging and patient risk stratification, highlights the importance of tailoring management to each patient’s needs. Ongoing research is crucial for refining techniques, establishing protocols, and understanding the long-term effects of non-operative management and minimally invasive approaches, promising better patient outcomes and satisfaction in diverticulitis treatment.
CRP: C-reactive protein
CT: computed tomography
LLD: laparoscopic lavage and drainage
MIS: minimally invasive surgical
KY and SA: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. Both authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 15244
Download: 93
Times Cited: 0
Valter Nilton Felix
Andrew P. Zbar, Nir Horesh
Nicholas B. D’Alessandro ... David A. Johnson