Original Article
Original Article

Affiliation:
Department of Anesthesiology/ICU and Perioperative Medicine, Hamad General Hospital, Doha 3050, Qatar
Email: wsaleem@hamad.qa
ORCID: https://orcid.org/0000-0002-3748-629X
Affiliation:
Department of Anesthesiology/ICU and Perioperative Medicine, Hamad General Hospital, Doha 3050, Qatar
ORCID: https://orcid.org/0009-0008-1825-606X
Explor Musculoskeletal Dis. 2024;2:106–115 DOI: https://doi.org/10.37349/emd.2024.00039
Received: June 13, 2023 Accepted: November 21, 2023 Published: April 10, 2024
Academic Editor: Fernando Pérez-Ruiz, Cruces University Hospital, Spain
Aim: The relationship between chronic pain conditions and itch occurrence has been studied; however, reports on itch among patients with different chronic pain conditions are limited. It is also unclear how pain medications affect itch experienced alongside chronic pain. The primary aim of the current study is to investigate the occurrence of itch among patients with various chronic pain conditions, and the secondary aim is to assess the impact of pain medication on itch episodes.
Methods: In the initial quarter of 2019, three hundred seventeen patients with chronic pain conditions were followed up at Hamad medical corporation (HMC)’s pain clinics. Of these, 285 met the study criteria and consented to participate. For patients who reported itch during the routine pain assessment, the 5-D score was utilized for the itch evaluation. The effect of pain medications on itch was also documented.
Results: Among the 285 patients, 41 (14.4%) reported experiencing an itchy sensation. Out of those 41 patients, 31 (75.6%) were diagnosed with neuropathic pain. This condition was found to be significantly associated with itch (P < 0.0001) compared to other conditions such as musculoskeletal (MSK) and fibromyalgia/myofascial pain, which accounted for only 12% of those who reported itch. Moreover, 25 (60.97%) of the patients with itch reported that they experienced concomitant itch sensations with pain episodes. Notably, 28 patients (68.3%) responded positively to pain medication. Furthermore, the study identified a significant correlation between the duration of pain and the incidence of itch (P < 0.0001).
Conclusions: The current study findings highlight neuropathic pain as the most prevalent chronic pain condition associated with itch. Additionally, the duration of pain was found to impact itch incidence.
Itch, also known as pruritus, is an uncomfortable sensation that makes individuals to scratch. This response serves as a protective mechanism and sensorimotor response against potential harm from internal or external factors [1]. Meanwhile, chronic pain is characterized by its persistence beyond the expected healing period, typically exceeding three months [2]. Interestingly, chronic itch and chronic pain have similar underlying mechanisms. Recent studies suggest that the mechanisms causing sensitization in pain and itch are similar, both peripherally and centrally, despite traditionally being viewed as opposing sensations [3]. More research is needed to explore potential pain relief therapies and deepen our understanding of human nociception [3].
Chronic pain includes a diverse group of patients with mixed nociceptive and/or neuropathic pain [4]. Furthermore, itch is classified into six main types: dermatological, systemic, neurological, psychogenic, mixed, and other [5]. Neurological itch, in particular, is further categorized into neuropathic and neurogenic. Neuropathic itch is associated with neuronal damage, which can result from endogenous substances stimulating itch-related neurons, as seen in conditions such as trigeminal hypoesthesia [5, 6], or localized itch from spinal cord lesions, as seen in cases of syringomyelia, tumors, infections, and injuries [7, 8]. However, despite these insights, the prevalence of itch among various chronic pain conditions is still unknown.
The aim of this study is to explore the occurrence of itch episodes in individuals with various chronic pain conditions in a diverse population. Additionally, since different pain medications have been reported to alleviate chronic itch conditions [9], we also aim to assess the effectiveness of these medications within our study cohort.
A cross-sectional study was conducted during the first quarter of 2019 on patients who visited pain clinics to assess chronic pain and itch. The study included patients who were 18 years or older, experiencing chronic pain, and who had agreed to participate in the study. Clinical assessments were conducted, and patients were asked about their pain and itch [10, 11]. Patients with documented dermatological diseases linked to allergies or pruritus concomitant with renal or liver diseases were excluded from the study.
A quantitative approach was used to calculate the sample size for non-parametric data. The sample size was determined using the equation “(Z1 – α/2)2 × p × (1 – p)/d2”. Where the Z1 – α/2 corresponds to the desired confidence level, p is the estimated prevalence of itching, and d is the desired precision.
A cohort of 317 patients diagnosed with various chronic pain conditions who were receiving medical care at the pain clinics of Hamad General Hospitals and the National Center for Cancer Care and research participated in the study.
Pain assessment and management were conducted following standard protocols [10]. To determine the primary objective, we used a validated 5-D score [11] when patients reported an itching sensation related to their current condition. This score assessed five crucial aspects: duration, severity, direction, disability (including sleep and functional impairments), and distribution of the itch, as detailed in Table 1.
The 5-D itch questionnaire assessing the impact of itch on a daily function
| 5-D itch scale dimension | Total number of patients/frequency (n = 41) | Percentage % | *P-value | ||
|---|---|---|---|---|---|
| Duration of pain | > 6 h | 24 | 58.50 | 0.71 | |
| 6–12 h | 12 | 29.30 | |||
| 12–18 h | 0 | 0 | |||
| 18–23 h | 1 | 2.40 | |||
| All day | 4 | 9.80 | |||
| Degree of itch | Not | 0 | 0 | 0.58 | |
| Mild | 18 | 43.90 | |||
| Mod | 18 | 43.90 | |||
| Sever | 5 | 12.20 | |||
| Unbearable | 0 | 0 | |||
| Direction of itch | Completely resolved | 0 | 0 | 0.65 | |
| Much better but still present | 0 | 0 | |||
| A little bit better, but still present | 0 | 0 | |||
| Unchanged | 38 | 92.70 | |||
| Getting worse | 3 | 7.30 | |||
| Disability | Sleep | Never effect sleep | 36 | 87.80 | 0.82 |
| Occasionally delays falling asleep | 0 | 0 | |||
| Frequently delays falling asleep | 3 | 7.30 | |||
| Delay falling asleep and occasionally wakes me up at night | 2 | 4.90 | |||
| Delay falling asleep and frequently wakes me up at night | 0 | 0 | |||
| Function | Never affect this activity | 0 | 0 | 0.86 | |
| Rarely affects this activity | 36 | 87.80 | |||
| Occasionally affects this activity | 4 | 9.80 | |||
| Frequently affects this activity | 0 | 0 | |||
| Always affects this activity | 1 | 2.40 | |||
| Distribution# | Face | 4 | 9.80 | 0.12 | |
| Chest | 6 | 14.60 | |||
| Back | 5 | 12.20 | |||
| Thigh | 4 | 9.80 | |||
| Legs | 7 | 17.10 | |||
| Soles | 19 | 46.30 | |||
| Groin | 4 | 9.80 | |||
* Significance values represent the P-value from a Fisher’s exact test comparing the distribution of responses in each category; # Among the 41 patients, some patients have more than one itching location
We collected demographic information and recorded pain condition diagnoses to analyze the correlation between itch sensations and pain episodes. As part of our secondary objective, we examined prescribed pain medications and asked patients if these medications provided relief from itch sensations, to which they responded with “yes” or “no”. Additionally, we confirmed that patients were not taking any medication specifically for itch by direct inquiry and verification of their medical records.
We performed data analysis using IBM SPSS Statistics for Windows, Version 23.0. A frequency test was employed to determine the occurrence rate of each parameter individually. Due to small sample sizes for some variables in this study, we used the Fisher’s exact test to assess the association between categorical variables, comparing the musculoskeletal (MSK), non-MSK infection (MSKI) groups and the itch and non-itch groups. Additionally, the independent samples t-test was applied with a significance level of 5% (P < 0.05) to evaluate statistical significance.
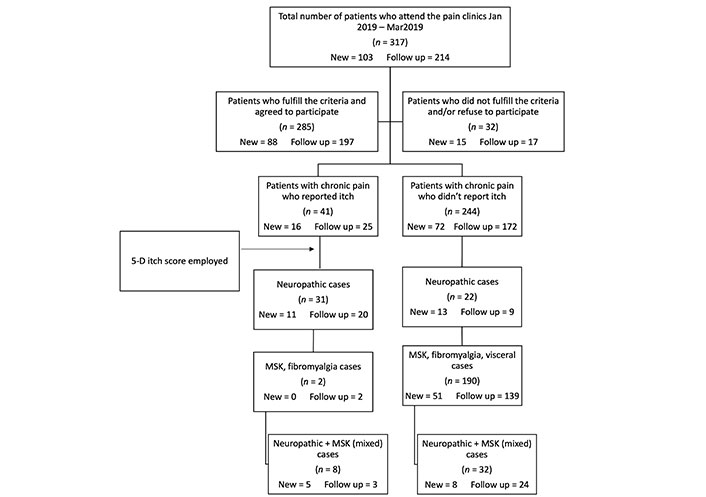
A total of 317 patients had visited HMC’s pain clinics. Out of the initial patient pool, 285 individuals met the inclusion criteria and agreed to participate in our research, as shown in Figure 1. The study analyzed a group of 285 participants with either MSK or non-MSK conditions, as detailed in Table 2. The average age of the MSK group was 52.30 years ± 13.74 years, and the non-MSK group had an average age of 51.77 years ± 14.07 years. Both groups had more females than males, with females comprising 25.30% and 30.50% of the MSK and non-MSK groups, respectively. The male demographic was 18.60% and 25.60% in the respective groups (Table 2).
Comparison of patients’ characteristics between MSK and non-MSK groups
| Characteristics | Total patients (n = 285) | MSK group (n = 125) | Non-MSK group (n = 160) | P-value | |||
|---|---|---|---|---|---|---|---|
| Number of patients/frequency | Percentage % | Number of patients/frequency | Percentage % | Number of patients/frequency | Percentage % | ||
| Gender | |||||||
| Male | 126 | 44.20 | 53 | 18.60 | 73 | 25.60 | 0.59* |
| Female | 159 | 55.80 | 72 | 25.30 | 87 | 30.50 | |
| Age (mean ± SD) | 51.20 ± 16.5 | - | 52.30 ± 13.74 | - | 51.77 ± 14.08 | - | 0.65** |
| Medication | |||||||
| Single | 111 | 38.90 | 42 | 14.70 | 69 | 24.20 | 0.10* |
| Multiple | 174 | 61.10 | 83 | 29.10 | 91 | 31.90 | |
| Pain duration | |||||||
| > 1 year | 270 | 94.70 | 124 | 43.50 | 146 | 51.20 | < 0.0001* |
| < 1 year | 15 | 5.30 | 1 | 0.40 | 14 | 4.90 | |
* Significance values represent the P-value from a Fisher’s exact test comparing between itch and non-itch groups; ** significance values represent the two-tailed P value from independent samples t-test comparing between the MSK and non-MSK groups. -: blank
Many individuals with MSK and non-MSK pain conditions had follow-up appointments that extended beyond one year at the pain clinic. The Fisher’s exact test revealed a significant association (P < 0.0001) between pain duration and both groups (Table 2).
The patients were analyzed based on the occurrence of itch and their diagnosed chronic pain, which was further classified in Table 3. Forty-one patients experienced itch alongside their pain condition, as indicated in Figure 1.
Comparative characteristics of patients with and without itch symptom
| Characteristics | Total group (n = 285) | Itch group (n = 41) | Non-itch group (n = 244) | P-value | |||
|---|---|---|---|---|---|---|---|
| Numbner of patients/frequency | Percentage % | Number of patients/frequency | Percentage % | Number of patients/frequency | Percentage % | ||
| Gender | |||||||
| Male | 126 | 44.20 | 22 | 17.50 | 104 | 82.50 | 0.58* |
| Female | 159 | 55.80 | 19 | 11.90 | 140 | 88.10 | |
| Age (mean ± SD) | 51.20 ± 16.50 | - | 56.50 ± 13.70 | - | 52.50 ± 13.80 | - | 0.65** |
| Diagnosis | |||||||
| Cancer | 84 | 29.50 | 19 | 22.60 | 65 | 77.40 | < 0.0001* |
| MSK | 116 | 40.70 | 1 | 0.90 | 115 | 99.10 | |
| Fibromyalgia/Myofascial | 9 | 3.2 | 1 | 11.1 | 8 | 88.90 | |
| Neuropathy | 34 | 11.90 | 12 | 35.30 | 22 | 64.70 | |
| MSK + neuropathy | 40 | 14 | 8 | 20 | 32 | 80 | |
| Visceral | 2 | 0.70 | 0 | 0.0 | 2 | 100 | |
| Medication | |||||||
| Single | 111 | 38.90 | 20 | 18.0 | 91 | 82 | 0.17* |
| Multiple | 174 | 61.10 | 21 | 12.1 | 153 | 87.90 | |
| Pain duration | |||||||
| > 1 year | 270 | 94.70 | 26 | 9.60 | 244 | 90.40 | < 0.0001* |
| < 1 year | 15 | 5.30 | 15 | 100.0 | 0 | 0 | |
* Significance values represent the P-value from a Fisher’s exact test comparing between itch and non-itch groups; ** significance values represent the two-tailed P-value from independent samples t-test comparing the two groups. -: blank
The demographic characteristics of the patient cohort are detailed in Table 3. The average age of the entire group was 51.20 years ± 16.50 years, with the itch group having a slightly higher average age of 56.50 years ± 13.70 years (P = 0.97). Regarding gender distribution, males made up 44.70% of the entire group, while females accounted for 55.30%. However, within the itch group, the proportion of males was slightly higher at 53.70%, compared to 46.3% for females (P = 0.23).
To further analyze the itch group (Table 3), we observed that out of the 41 patients in the itch group, 31 (75.60%) had neuropathic pain. This neuropathic pain included conditions such as chemotherapy induced peripheral neuropathy, trigeminal neuralgia, postherpetic neuralgia (PHN), post-burn peripheral neuropathy, and peripheral neuropathy.
In contrast, 8 (19.50%) patients in the itch group experienced mixed neuropathic cases, specifically radiculopathy associated with mechanical back pain. MSK conditions were the most prevalent among the cohort group, accounting for 40.70% of cases. However, only 2 (0.90%) patients reported itch incidence. For an overview of the chronic pain conditions considered in this study, please refer to Table 4.
Categorization of diagnoses among the study participants
| Category | Diagnosis |
|---|---|
| Cancer | Breast, renal, multiple myeloma, rectum, vulva, squamous cell carcinoma mandible, bladder, esophagus, lymphoma, tongue, and ovary |
| MSK | Facet arthropathy, tendon tear, joint degenerative disease |
| Fibromyalgia/Myofascial | Fibromyalgia/Myofascial |
| Neuropathy | Nerve/Root entrapment, diabetic, postherpetic, trigeminal, postsurgical and postburn neuropathies |
| Neuropathy + MSK | Spinal nerve root + facet degenerative/disc disease, post-trauma neuropathy |
| Visceral | Endometriosis, post-surgical abdominal pain |
We used Fisher’s exact test to analyze the relationship between variables within the itch and non-itch groups in Table 3. The results showed that itch is strongly linked to neuropathic conditions compared to MSK conditions (P < 0.0001). Additionally, chronic pain lasting for over a year is significantly associated with a higher likelihood of itch (P < 0.0001). These findings highlight the essential factors that contribute to itch in chronic pain.
Non-cancer cases made up a significant majority of the patient cohort, accounting for 70.50% of the total population (Table 3), while cancer cases represented 29.50% of the collected data. Among the cancer patients, 19 (22.60%) experienced both pain and itch symptoms, which they attributed to the chemotherapy they had undergone.
The chemotherapy regimens used in the study cancer group were diverse, including single and combination therapies such as trastuzumab, cisplatin, oxaliplatin, paclitaxel, docetaxel, bevacizumab, everolimus, vinblastine, capecitabine, gemcitabine, bortezomib, thalidomide, doxorubicin, and immunotherapy rituximab. The duration and number of cycles for each therapy regimen depended on the patient’s condition and the prescribed treatment protocol. Our analysis revealed no significant differences among patients who received different chemotherapy regimens concerning the presence or absence of itch symptoms in the current study.
To evaluate how itch affects the daily function of our patients, we utilized the 5-D itch dimension, as described in Table 1. Among the 41 patients, the majority (58.50%) experienced itch sensations for over 6 h a day, with a significant 9.80% experiencing itch sensations throughout the day. In terms of pain severity, most patients experienced mild to moderate itch 43.90% each, while 12.20% had severe itch. An overwhelming 92.70% of respondents reported no discernible changes in the direction of their itch, while only 7.30% noted a perceived worsening of their condition. The manifestation of itch affected sleep and daily function, with 12.20% reporting sleep disturbances and approximately 4.90% experiencing intermittent awakenings due to itch-related discomfort. In terms of daily functionality, 9.80% mentioned occasional impairment, while 2.4% reported that itch consistently interfered with their daily routines. The majority of patients experienced itch in their lower limbs (83.00%), followed by the trunk (26.80%) and the face (9.80%). Additionally, some patients reported itching sensations in more than one location, as detailed in Table 1.
Interestingly, when patients were asked about the timing of itch episodes that were associated with painful episodes, 25 individuals (60.97%) reported that itch occurred at various times, including during painful episodes, indicating mixed sensations during these episodes. Whereas, the remaining 16 patients in the itch group reported that itch episodes occurred at various times but never during painful episodes.
When patients were enquired about the effectiveness of the prescribed pain medications in relieving itch episodes, regardless of their temporal relation to painful episodes, a remarkable 68.3% reported positive responses to the medication. In comparison, 31.7% did not experience any improvement, not even partial relief.
Chronic pain and itch have been shown to be closely related in multiple studies [12–18]. Our current investigation builds upon this existing literature and sheds valuable insights on this connection. Consistent with earlier research [13–18], our study found that itch is more prevalent in neuropathic-related pain conditions than in isolated MSK pain. Specifically, conditions such as trigeminal neuralgia, postherpetic neuropathy, chemotherapy-induced neuropathic pain, lumbar radiculopathic pain, burn pain, and peripheral neuropathic pain have been associated with itch. However, we also found instances where patients with similar neuropathic conditions did not experience itch, and the underlying reasons remain unknown.
Our study is unique in that we investigated multiple chronic pain conditions that co-occur with itch in a clinical context. We also assessed MSK conditions, which constituted a large portion of the cases, although with a relatively low prevalence of itch in this cohort. Nevertheless, when MSK-related pain coexists with neuropathic pain, there is an increase in the incidence of itch. This observation supports the role of neuropathy in itch development. Furthermore, our study indicates that the duration of chronic pain is a contributing factor to the emergence of itch symptoms. Longer-lasting pain could lead to the initiation or worsening of itch symptoms, as demonstrated in our study.
Our study utilized the 5-D itch scale to minimize subjective reporting of itch. Our findings suggest that utilizing the 5-D itch scale can be beneficial for accurate itch reporting and tailoring our strategy to manage both pain and itch. It enables us to consider the dynamic changes from all five components of the scale [11, 19, 20].
Contrary to the traditional understanding of pain and itch as opposing sensory experiences, our research has shown that several patients in the itch group experienced episodes of itch along with pain. This unique combination of sensations often results in a strong urge to scratch the affected area, such as the mandibular or maxillary dermatomal region in trigeminal neuralgia or the area affected by herpes zoster. However, due to the presence of allodynia, scratching becomes challenging.
Chronic wounds can be associated with both itch and pain sensations. According to a study by Paul [21], 17.6% of the participants experienced both sensations simultaneously, either in or around the wound. The reason for this overlap between pain and itch is not fully understood, but it could be related to the extent of cutaneous deafferentation, whether complete or partial [22–23]. Research by Ständer and Schmelz et al.[18] suggests that the processing of pain and itch may not involve distinct brain centers but reflect different patterns of activation within the same centers [24]. Additionally, pruriceptive nerve fibers have different subtypes, such as mechano-sensitive and mechano-insensitive C-nociceptors. The diversity among pruriceptor classes could explain why patients experience various types of itch [25, 26] and why some patients experience both sensations simultaneously while others do not.
It is widely recognized that painful thermal, mechanical, and chemical stimuli can inhibit itch [26]. For instance, when histamine iontophoresis is used to trigger itch in healthy volunteers and patients with PHN pain, it frequently causes a burning sensation rather than pure itch [15, 27]. This indicates that neuropathic pain can affect both the immune system and peripheral nervous system, potentially leading to itch through the recruitment of mast cells and neurogenic inflammation, typically associated with an injury response [6, 27–28].
Additionally, the association between pain and itch in the patients studied can be explained by the altered response of itch to external/internal stimuli when activated in an excited state. There are overlapping receptor structures involved in pain and itch functions, such as protease-activated receptors (PARs) and transient receptor potential vanilloid (TRPV) [29, 30]. These similarities could help elucidate why pain medications often relieve itch. Central sensitization mechanisms underlying itch and pain, including allodynia and hyperalgesia, show significant similarities, as evidenced by neuroimaging studies [29] highlighting similar activated areas during pain and itch responses. However, the reasons for non-responsiveness in some patients require further investigation.
It is important to note certain limitations of this study. Both pain and itch are subjective sensations that depend on self-reporting, introducing a level of subjectivity. Additionally, due to the non-interventional nature of the study, we could not fully elucidate the mechanisms underlying the occurrence of itch during painful episodes, nor could we thoroughly investigate variations in the effectiveness of pain medication in the itch group. The role of duration in the incidence of itch in chronic pain cases remains unexplored. Multiple factors, including genetics, pharmacokinetics, and dynamics, may contribute to these variations, underscoring the need for further investigation in future studies.
HMC: Hamad medical corporation
MSK: musculoskeletal
We extend our appreciation to the Pain Management team at HMC for their valuable assistance in collecting part of additional data throughout the study period.
WS: Conceptualization, Methodology, Investigation, Formal analysis, Resources, Writing—original draft. MM: Conceptualization, Validation, Writing—review & editing. Both authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The study is approved by the ethical committee of both the anesthesiology department and the Hamad medical corporation board (approval no. CA00003/2019). The study took place from January 1st to March 31st, 2019 and was conducted in accordance with the Declaration of Helsinki.
Informed consent to participate in the study was obtained from all participants.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 4071
Download: 27
Times Cited: 0