Case Report
Case Report

Affiliation:
1Sports Physical Therapy Residency, Carolinas Rehabilitation, Atrium Health, Charlotte, NC 28211, USA
Email: Michael.Crinion@atriumhealth.org
ORCID: https://orcid.org/0009-0008-6794-1194
Affiliation:
2Mountain Island Lake, Carolinas Rehabilitation, Atrium Health, Charlotte, NC 28216, USA
Email: Andrew.Ball@atriumhealth.org
ORCID: https://orcid.org/0000-0002-0888-5363
Affiliation:
1Sports Physical Therapy Residency, Carolinas Rehabilitation, Atrium Health, Charlotte, NC 28211, USA
ORCID: https://orcid.org/0000-0002-9093-6077
Explor Musculoskeletal Dis. 2024;2:75–81 DOI: https://doi.org/10.37349/emd.2024.00036
Received: December 24, 2023 Accepted: January 30, 2024 Published: March 06, 2024
Academic Editor: Fernando Pérez-Ruiz, Cruces University Hospital, Spain
Following anterior cruciate ligament (ACL) injury of the knee, the functional hop test (an averaging of 4 component hop tests including single-hop, triple-hop, cross-over-hop, and 6-meter-hop) is commonly used by sports medicine physicians, doctors of physical therapy, and athletic trainers in return-to-practice and return-to-play decision making. In this case report, the functional hop test was applied to a 31-year-old recreational basketball player status-post full-tear of the anterior talofibular ligament (ATFL) to examine the applicability of a standardized, efficient, and easy-to-administer functional test in making return-to-play decisions following an ankle injury. The functional hop test was administered 5 times across a treatment course of 11 physical therapy sessions emphasizing pain-free range of motion, baseline strength, weight-bearing loading, and sport-specific training. The functional hop test was found to be a helpful (albeit imperfect) tool for clinical decision-making following an ankle injury. Specifically, improvements in landing skill/confidence of single hop accounted for the greatest gains in total score in the early phase of rehabilitation, while momentum and plyometric skill/control of triple hop accounted for the greatest gains in total score in the later phase of rehabilitation. Modification of the functional hop test to include sub-component tests of strength, endurance, and/or lateral hops are discussed.
Ankle injury, particularly in basketball and soccer athletes, has sparked significant attention in the realm of sports medicine [1]. Recent studies reveal that in girls’ basketball, the incidence of ankle injury stands at 2.08 per 1,000 athletic exposures while for boys, the incidence is slightly lower at 1.83 per 1,000 athletic exposures. Due to the demand of the ankle during repetitive cutting, running and posterior chain loading, soccer players face a common challenge [2]. The result of these high-speed lateral movements performed on the field or turf is that 66% of soccer injuries result in lateral ankle ligament injury with an additional 9% resulting in medial ankle ligament injury [3]. The primary mechanism of injury associated with anterior talofibular ligament (ATFL) injury is ankle plantarflexion (PF) with concurrent inversion (IV) [4]. Return-to-sport assessment status-post-ankle injury relies heavily upon objective measures, notably the single-leg calf raise to failure, whereby a threshold of 25–30 repetitions is considered indicative of sufficient strength [5]. However, the evaluation and treatment of ankle injury lacks uniformity among clinicians, both in terms of subjective surveys and objective measures and subjective assessments such as kinesiophobia surveys [6]. Y balance testing emerges as a valuable tool for assessing dynamic neuromuscular control, particularly in single-leg stance, serving as both a treatment modality and a potential screening tool for athletes prone to ankle injury [7]. Traditional return-to-play (RTP) testing encompasses a spectrum of assessment tools (from single-leg calf raises to sport-specific drills) aiming for an 80% success rate between the injured and non-injured limbs [4]. Initially proposed by Daniel et al. [8] to assist in clinical decision-making regarding RTP following anterior cruciate ligament (ACL) injury; the function hop test (FxlHT) is an assessment battery consisting of 4 component tests including the single-leg single-hop test, the single-leg triple-hop test, the single-leg cross-over hop test, and the 6-meter hop test [8]. The component tests are averaged, and the involved leg is compared to the uninvolved leg with a minimum threshold score of 90% being considered sufficient for return to play [9]. There is a paucity of literature on, and limited clinical use of, the FxlHT following ankle injury, ATFL specifically. Lateral hop abilities, however, exhibit a strong correlation with physical capability and return-to-sport confidence in ankle injury cases [10]. The primary aim of this case report was to assess the potential value of the functional hop test in tracking functional progress and in clinical reasoning regarding RTP status-post ankle sprain injury and rehabilitation. If suboptimal, we secondarily hoped to uncover additional efficient and effective component tests with which to modify the functional hop test for future case study and eventual validity testing.
A 31-year-old, 1.7 m tall, 72.57 kg male subject presented for evaluation with left ankle pain following a recreational basketball injury 2 weeks prior. The subject was playing basketball and landed on another player’s foot. The subject was quite active prior to injury, playing recreational basketball 2 to 3 times a week. Magnetic resonance imaging (MRI) confirmed full thickness tear of the ATFL. The subject had a functional pain scale (FPS) score of 6/10 pain [11]. He scored a 44 on a Focus on Therapeutic Outcomes (FOTO) survey with a predicted minimum important improvement/difference (MCII) of 70 [12]. The subject opted for conservative physical therapy intervention to address medical and recreational impairments versus cortisone injection or surgery.
The FxlHT, FPS and FOTO were utilized to assess and monitor pain intensity and physical functional status from evaluation through discharge. Upon initial evaluation of left ankle range of motion (ROM), a limitation of 0 degree dorsiflexion (DF), 25 degrees of IV, 15 degrees of eversion (EV), and 50 degrees PF was noted. Left ankle strength was similarly limited as manual muscle testing revealed DF 4–/5, PF 4–/5, IV 4/5, and EV 4/5. The subject’s maximal effort was inconsistent and questionable due to a subjective report of pain. The subject presented with positive anterior drawer and talar tilt and had severe tenderness to palpation of ATFL and calcaneal fibular ligament (CFL). Finally, the initial functional hop test score was 94% compared to the unaffected limb.
The subject’s episode of care included 11 visits during their care episode divided into four main phases (Table 1). Phase 1 spanned weeks 1–2, phase 2 covered weeks 3–4, phase 3 extended from weeks 5–6, and phase 4 involved a discharge assessment visit. The goal of phase 1 was to restore pain-free (ROM) and baseline strength necessary for light resistance and stability training in phase 2. Phase 2 involved weight-bearing loading activities, functional movements (such as lateral lunging and forward lunging on 3-way step taps) and proprioceptive feedback exercises. Ankle instability exercises, including Y balance testing, were employed to enhance ankle stability [13]. The subject demonstrated good tolerance for double leg (DL) depth drop landing in phase 2, absorbing force well from a 12-inch drop. Phase 3 consisted of sport-specific activities such as “euro step” driving, single-leg hopping to box, single-leg depth drops from a 6-inch step. The discharge phase encompassed single-leg balance treatment and final data collection of objective measures including FxlHT, ROM and single-leg calf raise test.
Rehab phases with exercises prescribed
| Clinical activity | Intervention | Outcome |
|---|---|---|
Evaluation Phase 1 Weeks 1–2 | Ankle ROM Ankle circles Bike Seated calf stretches Ankle isodynamic strengthening Theraband | Passive ROM DF 8 degrees PF 50 degrees IV 25 degrees EV 15 degrees MMT DF 4/5 PF 4/5 |
Treatment 1 Phase 2 Weeks 3–4 | Ankle isotonic strengthening Single-leg calf raises Single-leg shuttle press Ankle coordination training BAPS board Biodex single-leg stability training 3-Way step taps Single-leg balance Firm surface Foam surface Eyes open Eyes closed Blaze Pod training FxlHT (weeks 3 and 4) | Passive ROM DF 12 degrees PF 55 degrees IV 30 degrees EV 20 degrees MMT DF 4+/5 PF 5/5 |
Treatment 2 Phase 3 Weeks 5–6 | Lower extremity strengthening Deadlift barbell Star excursion exercise Y balance exercise Single-leg calf raises Plyometrics DL depth drop from 0.3 m Seated to DL hop to 0.3 m box Single-leg lateral hops (0.91 m, 1.22 m, 1.52 m) Elliptical FxlHT (weeks 5 and 6) | ROM DF 12 degrees PF 55 degrees MMT DF 5/5 PF 5/5 |
Discharge assessment Phase 4 | Lower extremity strengthening Single-leg calf raises, ×30 each Sport related exercises Z-cone drills T-cone drill Basketball shooting and layup drills Functional hop testing (discharge) | - |
BAPS: Biomechanical Ankle Platform System; MMT: manual muscle test; -: blank cell
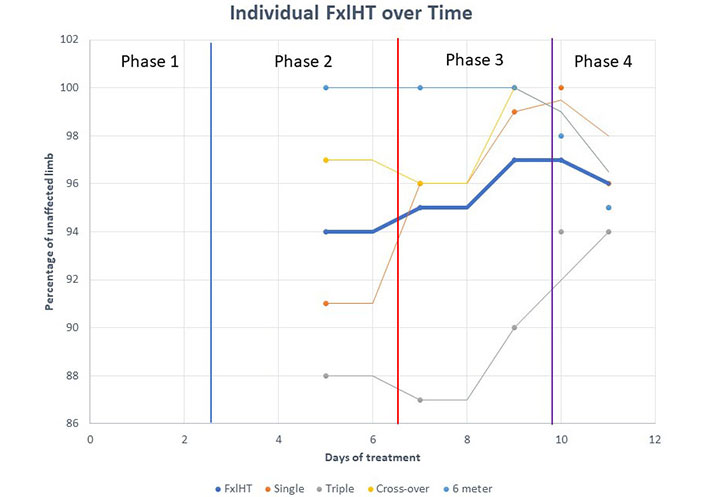
The primary focus of this case report was the exploration of the functional hop test as a tool for making RTP decisions following ankle injury. The prevalence of ankle injuries in sport underscores the need for standardized, efficient, and effective assessments from which to guide return-to-sport decisions. Incorporation of the functional hop test emerges as a valuable addition to the process but has some limitations of applicability when generalized from the knee and adapted to the ankle when used to guide rehabilitation strategies and inform decisions about readiness for return to competitive play. For example, a 2019 review published by Davies et al. [14] in the journal Sports Medicine recognizes that as applied to the knee, “hop tests display good reliability and are sensitive to change”. Although they go on to question the use of more than 2 hop tests “due to high collinearity and no greater sensitivity to detect abnormality” [14], when applied to the foot (recovery from ATFL injury in the athlete), we would encourage clinicians and researchers to use all 4 component tests of the functional hop test as the single-hop test appears more sensitive to change in the earlier phases of rehabilitation, while the triple-hop and cross-over-hop component tests appear more sensitive to change in the later phases of rehabilitation. Furthermore, just as Davies et al. [14] advocate the use of additional component tests that examine multiple planes of motion with respect to knee/ACL recovery, we advocate the use of the lateral hop test as an additional component test within a modified version of the functional hop test because studies have shown high electromyography (EMG) activity in differences between uninjured and injured ankles comparatively with EV and IV stabilizers [15]. The ankle then becomes a more stable base allowing for more dynamic movement and force production [16]. This allows clinicians to assess progression and develop increasingly sensitive RTS metrics as applied to athletes status-post ankle injury. The subject’s journey from initial testing to discharge unveils a narrative of progressive improvement, highlighting the intricate relationship between physical rehabilitation and self-report of readiness to RTP (Figure 1). Notably, the subject demonstrated improvements in the FxlHT through week 3 with a plateau and decline beyond that point. It is hypothesized by the authors that single-hop component test initially improved most rapidly and as it began to plateau, momentum-mediated component tests requiring balanced landing and immediate plyometric response (e.g., triple hop) then began to improve. With exercise prescription focusing on motor control and balance exercises, jump tests improved substantially as seen in Table 1. This was most notable between phases 2 and 3.
Across the episode of care, the FxlHT improved modestly from 94% to 97%, subsequently regressing to 96%. The score may be helpful in RTP decision-making based on the metrics of an ACL reconstruction [8, 10], but little is known regarding threshold measurements as applied to status-post ankle injury and rehabilitation. This improvement may be helpful in clinical decision-making regarding RTP and possible injury prevention, but in terms of RTP for ankle injuries additional tests may need to be included. The subject also demonstrated adequate gastrocnemius and soleus strength based on single-leg calf raise performance [17]. The subject increased FOTO score from 40 to 90 (well beyond MCII of 70), and furthermore verbalized feeling “very confident” and “100%” for RTP at his discharge visit.
The FxlHT emerges as a potentially useful tool for assessing the propulsion and deceleration phases of landing, crucial for athletes involved in activities with acceleration and sprinting [18]. Immediate feedback provided by these tests aids in evaluating an athlete’s ability to control force, influencing the progression toward RTP following ankle injuries. However, the FxlHT is limited in that it does not include a lateral hop component test. Modification of the functional hop test by incorporating a lateral hop component test may therefore provide a more comprehensive assessment by having the ankle joint go through a wide range of IV and EV in a dynamic situation [4]. The lateral hop test, for example, has shown significant value in RTP decision-making following ankle injury [14]. High muscle activity is also involved with stabilizing the ankle during lateral hop tests [15]. There may be a greater sensitivity to change in overall FxlHT test results by including a lateral hop test component. It is hypothized that doing so may provide more sensitive information for clinician use in RTP decisions [8]. The criterion validity of multi-planar testing in athletes engaging in multi-plane movements, as seen in sports such as soccer and basketball, cannot be underestimated. Lateral hop testing has been argued to be at least as important to forward hop component tests as applied to the knee [15] due to the high-speed lateral movements required of these athletes. Incorporation of a lateral hop test as an additional component test in an ankle-specific functional hop test may result in greater sensitivity to change, in a more linear fashion, throughout the entirety of the rehabilitation process. Finally, it must be considered that as a case report, caution should be taken in directly applying the ideas generated into clinical practice without further study. The FxlHT may in some cases prove to be a valuable tool in making RTP decisions following ankle injury, but may be insufficiently sensitive to nuanced change without additional modification (e.g., addition of lateral hop component test), particularly in phase 3. This case study also suggests that subjects with complete ATFL tear can return to sport without surgical intervention, but rather the application of physical therapy. Future research should explore modification of the functional hop test with additional component tests in pursuit of the optimal test-item-cluster in the determination of RTP.
ACL: anterior cruciate ligament
ATFL: anterior talofibular ligament
DF: dorsiflexion
DL: double leg
EV: eversion
FOTO: Focus on Therapeutic Outcomes
FxlHT: function hop test
IV: inversion
PF: plantarflexion
ROM: range of motion
RTP: return-to-play
MC and AB: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. MA: Conceptualization, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
All investigating authors/participants are Good Clinical Practice (GCP) certified by the Collaborative Institutional Training Initiative (CITI Program) for human subject research, ethics compliance and safety training. In addition, although Case Reports do not require IRB oversight, Atrium Health IRB Associate Director and Research Privacy Officer formally exempted this project from IRB oversight. Research coordinator of Atrium Health, Carolinas Rehabilitation, Sports Physical Therapy Residency program (Charlotte Campus), reviewed and verified manuscript for HIPAA and ethical compliance; and this study complies with the Declaration of Helsinki.
Informed consent to participate in the study was obtained from all participants.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 20442
Download: 137
Times Cited: 0