 Case Report
Case Report

Affiliation:
V.A. Nasonova Research Institute of Rheumatology, 115522 Moscow, Russia
Email: elicmax@yandex.ru
ORCID: https://orcid.org/0000-0003-1191-5831
Affiliation:
V.A. Nasonova Research Institute of Rheumatology, 115522 Moscow, Russia
ORCID: https://orcid.org/0009-0006-6138-9736
Affiliation:
V.A. Nasonova Research Institute of Rheumatology, 115522 Moscow, Russia
ORCID: https://orcid.org/0000-0002-8777-7597
Explor Musculoskeletal Dis. 2025;3:1007113 DOI: https://doi.org/10.37349/emd.2025.1007113
Received: October 24, 2025 Accepted: December 23, 2025 Published: December 24, 2025
Academic Editor: Fernando Pérez-Ruiz, Cruces University Hospital, Spain
The article belongs to the special issue Evaluation and Outcomes in the Management of Gout
The most common clinical manifestation of hyperlipidemia is the formation of xanthomas, which are most often localized subcutaneously, sometimes involving tendons and ligaments, and are usually asymptomatic. A fairly rare manifestation of hyperlipidemia is hypercholesterolemic arthritis caused by cholesterol crystals. In this article, we present a case of atypical xanthoma formation in a patient in the area of the first metatarsophalangeal joint, which resembled a gouty tophus. Taking into account the presence of hyperuricemia in the blood and the “classic” lesion of the first metatarsophalangeal joint, gout was primarily suspected in the patient. The diagnosis of arthritis associated with cholesterol crystals was confirmed using the “gold standard” diagnosis of microcrystalline arthritis—crystal detection using polarization microscopy. This case gives a clear idea of how important it is not to rely solely on the clinical picture when diagnosing gout.
Gout is a chronic systemic disease caused by the deposition of monosodium urate (MSU) crystals in organs and tissues in individuals with elevated serum uric acid (sUA) levels [hyperuricemia (HU)]. This occurs due to genetic and environmental factors, and clinically manifests itself as acute attacks of arthritis. A “classic” gout attack, with its typical symptoms of severe pain, swelling and redness primarily in the joints of the feet, usually raises few doubts about the diagnosis. However, the diagnosis should be based not only on clinical presentation but also confirmed by laboratory and instrumental testing, especially when acute arthritis may be associated with a bacterial infection. Obtaining synovial fluid or tophus contents and subsequent evaluation of the obtained material under a polarizing microscope is the preferred diagnostic method. This is indeed crucial, as definitive proof of gout depends on the detection of MSU crystals in the synovial fluid. But what we might consider a “classic” manifestation of gout is not always so.
Hyperlipidemia is characterized by elevated levels of one or more plasma lipids (triglycerides, cholesterol, cholesterol esters, phospholipids) and/or plasma lipoproteins [very-low-density lipoproteins (VLDL) and low-density lipoproteins (LDL)], and/or reduced levels of high-density lipoproteins (HDL) [1]. Depending on the etiology, hyperlipidemia can be classified into primary (familial or hereditary) and secondary (acquired) types. Hyperlipidemia is typically asymptomatic, although there are cases where hypercholesteremic arthritis can occur, which is a type of microcrystalline arthritic [2]. One of the visual clinical manifestations of hyperlipidemia is the presence of yellowish xanthoma deposits, which consist of lipids and are found within foamy macrophage cells and collagen, typically located around the eyes, tendons, and extensor surfaces of the limbs [3]. Differential diagnosis of xanthomas is carried out with benign skin formations such as syringoma, elastic pseudodoxanthoma, and in the area of tendons and ligaments, it is more often necessary to differentiate between lipomas, subcutaneous cysts, neurofibromas, and gouty tophi, although differential diagnosis with the latter is quite rare.
We report a case of a solitary, massive xanthoma located on the first toe of the left foot, mimicking a gouty tophus, in a patient with hyperlipidemia and asymptomatic HU. This study complies with the Declaration of Helsinki (2013).
The timeline is shown in Table 1.
Timeline.
| Date | Event overview |
|---|---|
| 2017 | Injury in the area of the 1st toe and the formation of a seal, a slow increase in the size of the node, which was asymptomatic until September 2024 |
| 2024-09-04 | The appearance of pain in the area of 1 MTPJ |
| 2024-09-06 | Ulceration of the node, consultation with a traumatologist |
| 2024-09-09 | Consultation with a rheumatologist, instrumental and laboratory examination |
| 2024-09-16 | Verification of diagnosis and prescription of therapy |
MTPJ: metatarsophalangeal joint.
A 49-year-old patient first applied to the V.A. Nasonova Research Institute of Rheumatology in September 2024 with complaints of pain in the area of the first toe of the left foot (25 mm on the visual analog scale) and discomfort when walking. In 2017, at the age of 42, he suffered a soft tissue injury to the first toe of his left foot (he stepped on a nail). Subsequently, he developed a thickening of the soft tissues and the formation of subcutaneous nodules at the site of the injury, which slowly increased in size. In early September 2024, there was a dull pain in the area of the first metatarsophalangeal joint (MTPJ), followed by spontaneous opening of the node with the discharge of white exudate. The surgeon suspected the patient had gout and referred him to a rheumatologist.
A subcutaneous, nodular lesion up to 3 cm in diameter with a small ulcerated surface (site of spontaneous drainage) was noted on the plantar aspect of the left first MTPJ (Figure 1).

Photo of the patient’s left foot before arthrocentesis. A subcutaneous nodule is visible in the area of the first MTPJ (metatarsophalangeal joint), resembling a tophus.
There was moderate pain on palpation in the area of the first MTPJ; no other inflamed joints or subcutaneous formations were found. Complete blood count was within normal limits; ESR: 18 mm/h; sUA: 7.43 mg/dL; creatinine: 86 µmol/L; GFR was 91 mL/min/1.73 m2.
Radiography revealed no destructive changes, but a large radiolucent lesion and soft tissue compaction were detected in the area of the first toe of the left foot. Ultrasound of the feet showed no signs of gout. The subcutaneous lesion projecting under the head of the first metatarsal bone was an extensive, non-vascular, multiloculated bursitis containing heterogeneous material.
A puncture of the node yielded 2.5 mL of whitish-yellow fluid. Polarized light microscopy revealed colorless, notched plate-like crystals consistent with cholesterol crystals (Figure 2); no other types of crystals were identified.
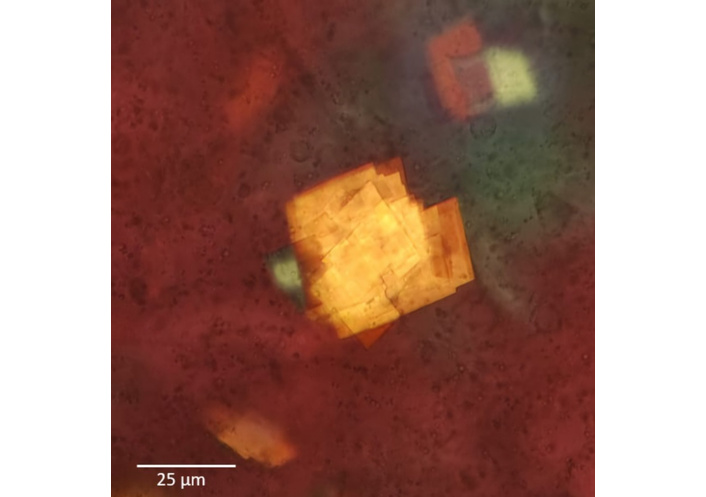
Cholesterol crystals viewed under a polarization microscope. Polarization microscopy by microscope Olympus СХ31-Р, Japan, ×400.
Lipid profile: total cholesterol 315 mg/dL; triglycerides 784 mg/dL; non-HDL cholesterol 284 mg/dL. Carotid artery ultrasound showed stable atheroscleotic plaque with calcium in right common carotid bifurcation with stenosis up to 26% without hemodynamic effect. Lower limb arterial ultrasound revealed forming plaque in femoral bifurcates with stenosis up to 30%.
Gout was excluded based on the results of the examination. Arthritis associated with cholesterol crystals and asymptomatic HU was verified.
The patient was under the supervision of a cardiologist and was prescribed fenofibrate at a dose of 145 mg per day. The tolerability of the therapy was satisfactory, but after 4 months, the patient was lost to follow-up.
Our case demonstrates that, even with characteristic symptoms, it is important to take a critical approach when making a diagnosis of gout and conducting differential diagnosis. In our case, we initially suspected gout based on the clinical symptoms alone: an elevated sUA level and the presence of a nodule in the area of the first MTPJ, which are very similar to subcutaneous tophi. Although the patient had no typical acute attacks of arthritis and the symptoms were limited to mild pain, in some cases, tophi may be the first manifestation of the disease [4, 5]. However, although subcutaneous tophi have the highest specificity of all clinical symptoms of gout, it is characterized by low sensitivity [6], and visualization of tophi-like formations during a physical examination cannot establish a diagnosis unless confirmed by instrumental methods. This case confirms this fact.
Polarized light microscopy of the resulting fluid revealed no MSU crystals, but all fields of view were covered with crystals of cholesterol crystals. Cholesterol crystals in synovial fluid are most commonly observed in rheumatoid arthritis [7], but it may also occur in gout, albeit without diagnostic significance [8]. Lipid crystals may also be present, distinguishable by their smaller size (1–30 µm) and characteristic Maltese cross appearance, whereas cholesterol crystals measure 5–40 µm and appear as notched plates [8].
HU is often linked to hyperlipidemia, especially hypertriglyceridemia [9]. However, it can also be associated with cholesterol and its fractions. A five-year cohort study involving 6,476 healthy Japanese adults (aged 30–85 years) demonstrated that for each 1 mg/dL (60 µmol/L) increase in sUA, the risk of elevated LDL rose by 16% in men and 22% in women [10]. Among the factors contributing to dyslipidemia, elevated sUA was the most significant.
Xanthomas are the most common visible sign of hyperlipidemia, usually appearing around the eyes and causing no symptoms. [11]. Musculoskeletal issues in hyperlipidemia can be symptomless or present as joint pain, tendinitis, mono- or oligoarthritis, or widespread polyarticular disease [12]. Tendinous xanthomas, often found in the Achilles tendon, are commonly linked to familial or mixed hypercholesterolemia [13]. Cases of hypercholesteremic arthritis have also been reported [14, 15]. One case involved a young woman with arthritis of the small joints of the hands and subcutaneous nodules near inflamed joints, raising suspicion for rheumatoid arthritis or gout. Another case described arthritis in the tarsometatarsal joint of the right foot, without subcutaneous nodules. In both cases, the diagnosis of hypercholesterolemic arthritis was confirmed by detection of lipids in nodule biopsy (first case) [14] and joint aspiration (second case) [15], along with hyperlipidemia.
This case illustrates a rare example of xanthoma localisation in a patient with hyperlipidaemia, without any other typical xantomas. Despite classic features of gout, such as asymptomatic HU and involvement of the first MTPJ, polarising microscopy was essential for diagnosis. This case emphasises the importance of testing synovial fluid in the differential diagnosis of suspected microcrystalline arthritis.
HDL: high-density lipoproteins
HU: hyperuricemia
LDL: low-density lipoproteins
MSU: monosodium urate
MTPJ: metatarsophalangeal joint
sUA: serum uric acid
MSE: Conceptualization, Supervision, Writing—review & editing. YIK: Conceptualization, Investigation, Writing—original draft. MNC: Investigation, Writing—original draft. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The work was carried out by the study “Development of approaches to phenotyping autoinflammatory degenerative rheumatic diseases based on a comparative study of biochemical, immunological and genetic factors associated with the state of bone, cartilage, muscle and adipose tissue” No. 125020501433–4. The study was approved by the local ethics committee at the V.A. Nasonova Research Institute of Rheumatology. This study complies with the Declaration of Helsinki (2013).
Informed consent to participate in the study was obtained from the participant.
The patient has been informed about this publication, and he gave written consent.
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 1326
Download: 11
Times Cited: 0
John S. Richards ... Mohan Ramkumar
Nuria Perez-Herrero ... Fernando Perez-Ruiz
